










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.71 no.10 Johannesburg nov. 2016
RESEARCH
Styloid process elongation according to age and gender: a radiological study
NJ ChabikuliI; CEE NoffkeII
ISenior Lecturer, Unit Radiology, School of Oral Health Centre, Sefako Makgatho University of Health Sciences, Pretoria, South Africa
IIBChD, MSc Odont. Professor, Unit Radiology, School of Oral Health Centre, Sefako Makgatho University of Health Sciences, Pretoria, South Africa
SUMMARY
The aim of the study was to investigate the ossification patterns and types of elongated styloid process (ESP) in relation to age and gender in patients attending the Medunsa Oral Health Centre at Sefako Makgatho Health Sciences University. Out of the 102 panoramic images evaluated, 40.2% and 59.8% were male and female patients respectively. Type I ESP was the most frequent type (59.1%), followed by Type III (24.8%), Type II (9.4%) and Type IV (7.7%). The Type A calcified outline pattern of ossification was the most common (48.9%), followed by Type D (28.9%), Type C (14.1%) and Type B (8.1%).
Panoramic images are vital in evaluating ESP seen as incidental findings and dental practitioners need to be aware of its variations.
INTRODUCTION
The styloid process (SP) can be seen on both sides of a panoramic radiograph as a slender bony projection extending inferior and slightly mesially just beneath the external auditory meatus.1 It gives rise to two ligaments, the stylohyoid and the stylomandibular ligament and provides attachment for three muscles, the styloglossus, stylohyoid and stylopharyngeus which act together during normal oropharyngeal functions.1 The apex of the styloid process is continuous with the stylohyoid ligament which is attached to the lesser horn of the hyoid bone.1,2 The apex is situated between the internal and external carotid arteries,2 the clinical significance of which will be explained.
The styloid process arises from the second branchial arch, Reicher's cartilage.3 There are two cartilage centres from which the SP develops, first the tympanohyal one which is present at birth. It becomes calcified and only attached to the temporal bone in the first year of life. The second cartilage centre which appears after birth is termed "stylohyal". The two centres normally fuse at puberty. Radiologically, absence of fusion is indicated by a radiolucent line which can be mistaken for a fracture line.4 Terms used in the literature such as "stylohyoid chain", "stylohyoid complex" and "stylohyoid apparatus" all refer to the anatomical configuration of the styloid process together with its stylohyoid ligament and the lesser horn of the hyoid bone at which the ligament is inserted. These terms are often used interchangeably.1,5 The normal length of the SP in an adult varies from 20-30mm and is considered elongated when it measures more than 30mm.1,3 Components of the stylohyoid chain may undergo ossification, in particular the stylohyoid ligament (SHL). When ossification occurs, the styloid process appears elongated and is referred to as an "elongated stylohyoid process".2 The term elongated styloid process (ESP) was first described by Watt Eagle, an Otolaryngologist in 1937 who also found that the ESP may produce head and neck pain and other symptoms, known collectively as Eagle's Syndrome.
This is a fairly rare condition.3,6 The exact aetiology of ossified and elongated SP is unknown.3 It is important for clinicians and radiologists to have a sound knowledge of the normal anatomy and to be aware of abnormalities of the styloid process. Depending on the size, shape and orientation, an ESP may cause a stroke due to the compression of the carotid artery.7 Since stroke is among the top four causes of death in South Africa and the top ten leading causes of disability internationally,8 it was decided to investigate the ossification patterns and types of ESP and its relation to age and gender in patients attending the Medunsa Oral Health Centre at Sefako Makgatho Health Sciences University. The ESP was detected as an incidental finding on panoramic radiographs of patients who consulted for dental care at the Institution.
MATERIALS AND METHODS
This study was a retrospective, descriptive cross sectional study in which measurements were performed on archived radiographic images. Ethical approval for the study was granted by the Ethics Committee of the Sefako Makgatho Health Sciences University. The study population consisted of routinely taken panoramic radiographic images of adult patients who had visited the Oral Health Centre of Sefako Makgatho Health Sciences University between January 2013 and December 2014. The panoramic radiographs had been taken with a digital panoramic system (SIRONA Orthophoss XG5) using digital sensors under standard exposure factors as recommended by the manufacturer. A total of 147 images were archived. Accurate measurements were performed for a convenient sample of 69% (102/147) of diagnostically acceptable images of patients with styloid process/processes of a length greater than 30mm. The radiographic images were stored on Dicom Carestream software. Measurements of the lengths of styloid processes were performed on diagnostically acceptable images from the tympanic plate to the tip of the styloid process by two experienced calibrated radiologists as described by Ilguy and colleagues (2005).9 The types of appearance of the styloid process elongation seen in this study were classified using the numerical method described by Langlais et al (1986)10 with modifications reported in other studies.3,11
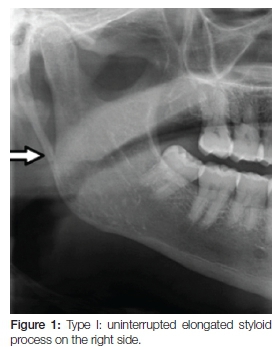
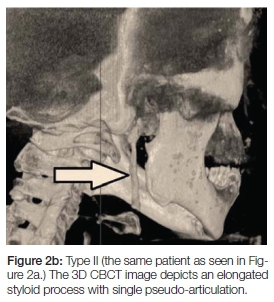
Type I: Uninterrupted integrity of styloid process (> 30mm) (Figure 1); Type II: Styloid process joined to the mineralized stylomandibular or stylohyoid ligament by a single pseudo articulation (Figures 2a and b); Type III: Segmented styloid process containing multiple segmented pseudo articulations (Figure 3) and Type IV describes elongation of styloid process due to distant ossification and is derived from a variant published by Reddy et al.3 as a modification of the "H" and "J" patterns described by MacDonald-Jankowski which were presented as a possible classification.11 (Figure 4).



The patterns of styloid process ossification were also recorded, classified using Langlais' system which differentiates the calcified ESP's into Types A to D.10
Radiographic Modified Langlais et al10 classification of patterns of ossification of elongated styloid processes (Figures 5-8)
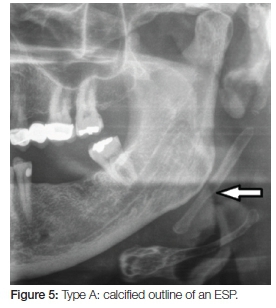


Type A: Calcified outline of styloid process (Figure 5);
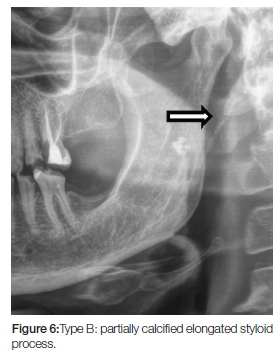
Type B: Partially calcified styloid process with discontinuous radiolucent core (Figure 6);
Type C: Nodular appearance of styloid process with varying degrees of central radiolucency (Figure 7) and
Type D: Completely calcified styloid process with no evidence of a radiolucent interior structure (Figure 8).
Data of demographic characteristics was extracted. The variables for which data were available included age and gender. Data was coded and cleaned in Microsoft Excel software and then transferred to SAS software (SAS Institute Inc, Carey, NC, USA) for statistical analysis.
RESULTS
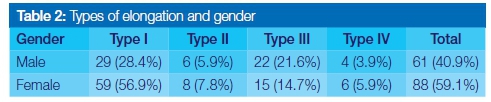
A total of 147 panoramic images had styloid processes measuring more than 30mm, however only 102 images were of acceptable diagnostic quality with a total number of 149 elongated styloid processes. Forty one (40.2%) patients were males and 61 (59.8%) were females. Table 1 showed that the male patients most affected by ESP were in the age group 18-29 years. The 50-59 age group of males showed the least number of ESPs while the majority of the female patients with ESP were in the older age groups i.e. 24% for 50 -59 years and 21% for 60 years and older. Type I ESP occurred most frequently for both male and female patients, whereas Type IV ESP showed the least occurrence (Table 2). Type I ESP was also most frequently found in all age groups (59.1%), followed by Type III, Type II and Type IV (Table 3). The calcified outline pattern of ossification occurred the most frequently in both genders (48.9%), followed by the distant ossification pattern (28.9%) and nodular pattern (14.1%). The partially calcified pattern was the least common (8.1%%) (Table 4). Table 5 showed that the calcified outline pattern occurred most frequently in all age groups and type B pattern the least (8.1%).




DISCUSSION
Elongated styloid process is a term used by Eagle, an Otorhinolaryngologist, in an article published in 1937 to describe SP longer than 30mm on lateral skull radiographs of dentomaxillofacial and ear-nose-throat patients.6 Panoramic radiography, lateral oblique and cone-beam computed tomography are other imaging modalities used by several authors to diagnose ESP.7,9,12,14 Panoramic images were used in this study for diagnosis of ESP types and patterns of ossification. The elongated styloid processes in this study were reported as incidental findings, the panoramic radiographs were requested for other indications, which was in accord with Alpoz et al.14
In the present study females were more commonly affected than males (59.8 and 40.2% respectively), which was in accordance with other studies conducted in Turkey, Brazil and Japan,12-15 however some studies have found males to be more commonly affected.7,16-19 Type I elongation was found to be the most common in the present study which was in accord with studies done by various authors.2,3,16,19
The present study also found that the calcified outline pattern of ossification was the most common, and several studies had the same findings.2,9,19 Most of Type I ESP showed a calcified outline, however a study conducted by Reddy et al.3 in India found Type I in most patients to be completely calcified (Type D ossification pattern). In a Turkish population the most frequent type and pattern of ossification was Type II and Type B.20
CONCLUSION
In the population sample studied, Type I with calcified outline ESP was observed the most frequently.
ESP is often an incidental finding and awareness of the styloid process variations by Dental Professionals is important.
Conflict of interests: None declared.
ACRONYMS
ESP: elongated styloid process
SP: styloid process
SHL: stylohyoid ligament
References
1. Scarfe WC, Farman AG. Soft tissue calcifications in the neck: maxillofacial CBCT presentation and significance. AADMRT Currents 2010; 2:3-15. [ Links ]
2. Anbiaee N, Javadzadeh A. Elongated styloid process: Is it a pathologic condition? Indian J Dent Res 2011; 22: 673-7. [ Links ]
3. Reddy R, Sai Kiran Ch, Sai Madhavi N, Raghavendra MN, Satish A. Prevalence of elongation and calcification patterns of elongated styloid process in South India. J Clin Exp Dent 2013; 5: 30-5. [ Links ]
4. Worth HM. Principles and Practice of Oral Radiologic Interpretation, 1st ed. Chicago: Year Book Medical Publishers, 1963. [ Links ]
5. Noffke C, Raubenheimer E, Chabikuli N. Radio-opacities in soft tissue on dental radiographs: diagnostic considerations. SADJ 2015; 70: 54-9. [ Links ]
6. Eagle WW. Symptomatic elongated styloid process: report of two cases of styloid process-carotid artery syndrome with operation. Arch Otolaryngol 1949; 49: 490-503. [ Links ]
7. Bagga MB, Kumar C, Yeluri G. Clinicoradiologic evaluation of styloid process calcification. Imaging Sci Dent 2012; 42: 155-61. [ Links ]
8. Mudzi W, Stewart A, Museng E. Case fatality of patients with stroke over a 12-month period post stroke. SAMJ 2012; 102: 765-7. [ Links ]
9. Ilguy D, Ilguy M, Fisekcioglu E, Dolekoglu S. Incidence of the type and calcification patterns in patients with elongated styloid process. J Int Med Res 2005; 33: 96-102. [ Links ]
10. Langlais R, Miles D, Van Dis M. Elongated and mineralized stylohyoid ligament complex: a proposed classification and report of a case of Eagles Syndrome. Oral Surg Oral Med Oral Pathol 1986; 61: 527-32. [ Links ]
11. MacDonald-Jankowski D. Calcification of the stylohyoid complex in Londeners and Hong Kong Chinese. Dentomaxillofac Radiol 2001; 30: 35-9. [ Links ]
12. Gokce C et al. Prevalence of styloid process elongation on panoramic radiography in the Turkey population from Cappadocia Region. Eur J Dent 2008; 2:18-22. [ Links ]
13. Rizzati-Barbosa C, Ribeiro M, Silva-Concilio L, Di Hipolito O, Ambrosano G. Is an elongated styloid process prevalent in the elderly? A radiographic study in a Brazilian population. Gerodontology 2005; 22: 112-5. [ Links ]
14. Alpoz E et al. Prevalence and pattern of styloid chain complex patterns detected by panoramic radiographs among Turkish population. Surg Radiol Anat 2014; 36:39-46. [ Links ]
15. Okabe S, Morimoto Y, Ansai T, Yamada K, Tanaka T, Awano S, Kito S, Yakata Y, Takehara T, Ohba T. Clinical significance and variation of the advanced calcified stylohyoid complex detected by panoramic radiographs among 80-year old subjects. Dentomaxillofac Radiol 2006; 35: 191-9. [ Links ]
16. Shaik M, Naheeda, Kaleem S, Wahab A, Hameed S. Prevalence of elongated styloid process in Saudi population of the Aseer region. Eur J Dent 2013; 7: 449-54. [ Links ] .
17. More CB and Asrani MK. Evaluation of the styloid process on digital panoramic radiographs. Indian J Radiol Imaging 2010; 20: 261-5. [ Links ]
18. Scaf G, Freitas DQ, Loffredo Lde C. Diagnostic reproducibility of the elongated styloid process. J Appl Oral Sci 2003; 11:120. [ Links ]
19. Shah S, Praveen N, Subhashini A. Elongated styloid process: A retrospective panoramic radiograph study. World J Dent 2012; 3: 316-9. [ Links ]
20. Oztunc H, Evlice B, Tatli U, Evlice A. Cone-beam computed tomographic evaluation of styloid process: a retrospective study of 208 patients with orofacial pain. Head Face Med 2014; 10: 5. [ Links ]
 Correspondence
Correspondence
Ntombizonke J Chabikuli
Senior Lecturer, Unit Radiology
School of Oral Health Centre
Sefako Makgatho University of Health Sciences, Pretoria
South Africa
Email: Ntombizonke.Chabikuli@smu.ac.za
