










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.71 n.9 Johannesburg Oct. 2016
CLINICAL WINDOWS
What's new for the clinician? Summaries of and excerpts from recently published papers
V Yengopal
BChD, MChD (Community Dentistry) Stellenbosch. Department of Community Dentistry, School of Oral Health Sciences, University of the Witwatersrand. E-mail: Veerasamy.Yengopal@wits.ac.za
1. Using social media to improve compliance and duration of treatment in orthodontic patients: A RCT
Li, X., Xu, Z., Tang, N. et al. Effect of intervention using a messaging app on compliance and duration of treatment in orthodontic patients. Clin Oral Invest (2016) 20: 1849
Depending on the individual case, orthodontic treatment usually takes a long time to obtain the desired result. Studies have also found that behaviour-related factors such as missed appointments, unplanned debonding of brackets, and poor oral hygiene, could significantly prolong the duration of orthodontic treatment.1 These might imply poorer compliance of the patients. Therefore, reducing these factors has become an important element when managing these patients in an orthodontic practice.
Communication via cellphones has become an important tool in the health care arena. The use of short message services (SMS) and other applications such as WhatsApp, We Chat, BBM, etc have revolutionised the manner in which we can communicate with patients. In Dentistry, evidence has shown that attendance could be notably improved by simply sending a reminder of any type before the appointments.1 Similarly, education and reminder messages were found to effectively enhance patients' oral hygiene and knowledge.
In the past few years, WeChat (Tencent Ltd., Shenzhen, China. 'Weixin' in Chinese version) has become one of the most popular messaging software on cell phones, especially among Chinese young people.1 There are more than 1.12 billion registered users and 600 million active users of WeChat worldwide, mostly in China.1 It is not only a software for chatting like WhatsApp and Facebook Messenger but also one of the most trendy platforms for news reading, blogging, and social networking.1 WeChat has a multifunctional background interface, allowing service providers to deliver texts and multimedia contents to all subscribers.1 There is a paucity of studies that have explored the use of these platforms in the dental field to communicate with patients and even fewer studies have been attempted to determine whether such technologies can shorten the treatment time by promoting compliance among orthodontic patients.
Li and colleagues (2016)1 from China reported on a randomized clinical trial that sought to investigate whether mobile intervention using WeChat, vs. usual care, would improve the attendance and oral hygiene of patients, reduce the incidence of bracket debonding, and consequently, shorten the duration of orthodontic treatment (DOT).
MATERIALS AND METHODS
This was a non-blinded, two-arm randomized controlled trial in China conducted among adolescents or adults admitted for orthodontic treatment. Participants were randomized 1:1 to the intervention group or control group after the initial examination. Eligibility of a patient was determined after the treatment plan was finalized. Patients were excluded if they (1) were unable to read Chinese; (2) did not use smartphone that could install WeChat app; (3) preferred the lingual or invisible bracketless technique; (4) were planned for a multiphase treatment, like combined orthodontic-orthognathic treatment; (5) presented a case too complicated to be finished within three years; and (6) disclosed a possibility that they may migrate to another city within the predicted treatment period.
Thus, only those orthodontic patients with fixed appliance and single-phase treatment participated in the trial. Demographics and dental profile concerning the orthodontic treatment were recorded.
At a patient's first visit, a standard examination procedure was performed to make a proper diagnosis, including study casts, panoramic and lateral cephalometric radiographs, extra-oral and intra-oral photograph, etc. Two combinations of bracket systems were used in the treatment: Damon Q self-ligating brackets with Damon Q archwires and HX straight wire brackets (non-self-ligatiing), plus IMD Orthodshape archwires (IMD). All brackets were bonded with light-cured composite and patients were asked to revisit every four weeks. If any brackets accidentally debonded, patients could visit the clinic for the removal of the loose items, but had to wait until the next appointment to have the brackets rebonded. A fee was charged for this repair. If a patient failed to attend or cancelled an appointment, they were rescheduled to two to four weeks later. The end of the treatment was defined as when the treatment goal had been achieved, and all brackets and other appliances were removed.
Participants in WeChat group were instructed to subscribe to the research account of the investigators on WeChat at the first day of treatment. For patients under 18 years, at least one of their parents was also added as a message receiver. The researchers' phones were also added to the receiver lists. There were basically two types of messages: reminder messages with brief texts and educational messages with Rich texts and pictures. Reminder message of attendance was scheduled to be sent twice (one week and one day) prior to the appointment. Patients were asked to reply to the appointment reminders if possible. Other reminders were focused on behaviour change. Educational messages were linked to articles on oral health tips and knowledge. Patients enrolled in the same week were grouped into the same batch, which received the same scheduled educational messages. All contents were written in Chinese. Participants were allowed to browse more contents by clicking the hyperlinks. They could also query the next appointment, or open the Frequently Asked Questions option and source the answers.
The conventional-care-only control group received the same orthodontic strategy and pre-treatment education as in the WeChat group but they were not afforded the opportunity to use the WeChat platform.
The primary outcome measure was the duration of orthodontic treatment (DOT). DOT was defined as the period (weeks) from the initial application of brackets to the completion of treatment. The subsequent period using a retainer was not counted in the duration of orthodontic treatment. The time taken to complete treatment was also calculated. The secondary outcomes included (1) failed attendance, (2) late attendance, and (3) bracket bond failure. The exact time of attendance was recorded. It was counted as a failed attendance if the patient came too late and required rescheduling. It was not counted as a failed attendance if patients requested rescheduling one week or earlier prior to their appointment. The tertiary outcome measure was the oral hygiene condition, graded with orthodontic plaque index (OPI) and modified gingival index (MGI). The OPI and MGI were evaluated at the first visit after the initial bonding (baseline) and just before treatment completion (endpoint).
RESULTS
Two hundred and twenty four patients (n=224) were included in this trial; and112 were randomly allocated to each group. All 224 patients completed their treatment and were included in the analysis. There were more females in the study (156, 69.6 %). The mean age of participants was 17.6 ± 5.7 years, and nearly half were adults (105, 46.9 %). Extractions were performed in nearly half of the cases (103, 46.0 %). Self-ligating brackets were applied in 139 (62.1 %) subjects. All the demographics and baseline characteristics were balanced between the two groups.
The duration of orthodontic treatment (DOT) in WeChat group was significantly shorter, compared with the control group (median 80.5 vs. 84.5 weeks, range 66-93 vs. 75-103, P = 0.007). The mean difference between the two groups was 7.3 weeks (95 % CI 3.7 to 11.6). The Kaplan-Meier curve showed that individuals in WeChat group were likely to complete treatment earlier than control (HR = 1.49, 95 % CI 1.14 to 1.95; p = 0.003).
There were 2161 and 2360 appointments altogether in WeChat and control group. The total number of failed and late attendance in WeChat groups were 68 (3.1 %) and 435 (20.1 %) respectively compared to 256 (10.9 %) and 706 (29.9 %) in the control group. Patients in the WeChat group had significantly fewer failed attendance than the control group (35, 31.3 % vs. 83, 74.1 %; RR = 0.42, 95 % CI 0.31 to 0.57).
In terms of bracket bond failure, there were 666 (16.3 % of 4104 bonded) brackets bond failures during the treatment period. A lower rate of bond failure was observed in WeChat group versus the control group (11.8 vs. 16.1 %, P < 0.001). The number of individuals who had at least one bracket debonded showed no significant difference between the two groups (56.2 vs. 68.8 %, P = 0.053). However, subgroup analysis found fewer adults with bond failure after WeChat intervention (24.5 vs. 48.1 %, P = 0.024).
There were no significant differences between the two groups as regards the orthodontic plaque index (OPI) and modified gingival index (MGI) at either baseline or endpoint evaluation.
Five compliance-related factors concerning attendance, bracket bond failure, and oral hygiene were screened using a univariate approach. Failed attendance was identified as the only independent factor affecting the time to finish treatment. This implied that the greater the number of missed appointments, the more likely it was that the treatment completion was delayed (P = 0.004, HR = 0.89, 95 % CI 0.84 to 0.95). No adverse effect of the intervention was reported throughout the research.
CONCLUSION
This trial showed that the intervention using a mobile messaging app effectively reduced the duration of orthodontic treatment. It also improved the attendance of the patients and decreased the bracket bond failure rate when compared with patients who did not use the mobile app.
IMPLICATIONS FOR PRACTICE
This trial has showed improvements in treatment management among patients who were linked to a mobile message system. This study has highlighted the potential for the expanded use of social media in health in our setting where cellphones are used by the majority of the population.
ACRONYMS
OPI: orthodontic plaque index
DOT: duration of orthodontic treatment
MGI: modified gingival index
Reference
1. Li, X., Xu, Z., Tang, N. et al. Effect of intervention using a messaging app on compliance and duration of treatment in orthodontic patients. Clin Oral Invest (2016) 20: 1849 [ Links ]
2. Assessment of postoperative pain after reciprocating or rotary NiTi instrumentation of root canals: a randomized, controlled clinical trial
Relvas, J.B.F., Bastos, M.M.B., Marques, A.A.F. et al. Clin Oral Invest 2016:20: 1987
Endodontic postoperative discomfort is defined as any degree of pain that occurs after endodontic treatment.1 This phenomenon is known in literature as flare-up, which is characterized by the development of pain, swelling or both, beginning within a few hours or days after the surgical procedures.1
The recent introduction of rotary and reciprocating endodontic systems has resulted in reduced treatment times, less patient discomfort and less pain during the procedure when compared with the traditional mechanical way of cleaning and obturating root canals.1 Recent studies have shown that the treatment protocols of new reciprocating systems can also produce extrusion of debris in the apical region, which could be related to postoperative pain when compared with other traditional instrumentation techniques.1
Thus, on the premise that an innovative reciprocating system can cause different levels of pain after endodontic treatment, Relvas and colleagues (2016)1 reported on a study that sought to assess postoperative pain in a prospective randomized clinical trial comparing two groups, using the Reciproc® system in one group and the ProTaper® rotary system in the other. The primary outcome measure of the study was to assess whether different instrumentation techniques influence the occurrence of postoperative pain.
MATERIALS AND METHODS
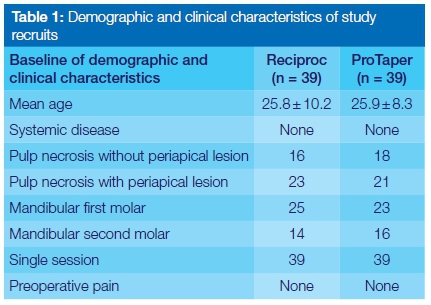
This was a randomized, controlled, double-blinded parallel-group trial with an equal allocation rate between groups. The study sample consisted of men over the age of 18, who had had previous indication for endodontic treatment in permanent mandibular molar teeth and had been diagnosed with asymptomatic pulp necrosis. The pulpal status was confirmed by a negative response to cold and electric pulp tests and was confirmed later by the absence of bleeding on opening of the pulp chamber. Immunocompromised patients who were on antibiotics, analgesics, or corticosteroids preoperatively or during treatment were excluded. Additionally, during the root canal procedure, teeth that could not be treated in a single-session or patients who interrupted treatment were excluded. Table 1 provides information of the study participants.
Randomization was done through a table generated by the Sealed Envelope™ software by a third investigator not involved in the research protocol. A list of 80 numbers was prepared, divided into four blocks, 40 in each group. Each number from the list with the sequence of the experimental and control groups was individually placed in a numbered, opaque, sealed envelope. Once the patient was considered eligible for the procedure, and prior to the endodontic treatment, the envelope was opened by the researcher-operator to identify which individual belonged to which group. Both the patient and researcher-evaluator were blinded to the treatment protocol until the access to the root canal system was performed.
Of the 138 patients considered for the study, 50 were excluded because they did not meet the inclusion criteria. Thus, only 78 individuals were selected for allocation to groups and the individuals were randomly assigned to two groups, that is, 39 patients in the Group Reciproc® (RP) and 39 in ProTaper® group (PT).
Endodontic treatment followed a treatment protocol according to the two techniques used in the study. The cold test was performed by spraying a cotton swab, which was then placed on the occlusal surface of the tooth. If there was no response after five seconds, the test result was considered negative.
A glide path was established using PathFiles 0.13, 0.16, and 0.19 for both groups (Dentsply Maillifer). The working length was confirmed with an electronic apex locator and radiography. Instrumentation of the root canals was performed in accordance with the manufacturer's recommendations and began with the canal negotiation using size 10 K-file and the PathFile instruments #0.13, 0.16, and 0.19. For the Reciproc® system, the instruments were driven by the VDW Silver® motor, specifically programmed for reciprocating instrumentation.
The instrumentation of the root canals with the ProTaper® system began with the canal negotiation with the size 10 K-file and the PathFile instruments #0.13, 0.16, and 0.19. Canal shaping was achieved with ProTaper rotary instruments following the manufacturer's instructions. The instruments were also driven by the VDW Silver® motor.
The root canals were abundantly irrigated with 2.0mL of 2.5% sodium hypochlorite after each instrument exchange, and the irrigating solution remained in the root canal during the procedure. For both groups, sodium hypochlorite was applied with the aid of the 30-G Max-i-Probe needle(Dentsply Maillefer) up to 4mm short of the working length. The amount of irrigating solution did not exceed 40mL. For all the root canals, patency was performed with a size 10 K-file.
All teeth received the same amount of irrigating solution and the root canals were also irrigated with 17% EDTA prior to obturation. First, the root canals were completely dried using sterile absorbent paper points compatible with the root canal diameters. The gutta-percha master cone, compatible with the root canal instrumentation (ProTaper F1-F4, Dentsply Maillefer or R25-R50, VDW), was then inserted into the root canal and the first 5mm were coated with AH Plus sealer (Dentsply Maillefer). Obturation was then completed and temporary sealing with glass ionomer cement, occlusal adjustment (completely taken out of occlusion), and final radiography were performed. Patients were referred to their clinic of origin for tooth rehabilitation.
After endodontic treatment, all patients were asked to fill out a verbal description scale according to the operator's instructions (primary outcome). The questionnaires were assessed by the researcher-evaluator who did not have access to the data regarding the type of treatment performed by the operator. To assess postoperative pain, a scale of pain intensity was applied 24 h, 72 h, and 7 days after endodontic treatment. Pain was recorded on a verbal rating scale (VRS) as follows: 0: no pain or discomfort; 1: mild pain: feeling pain, but no oral medication (analgesics) required; 2: moderate pain: feeling pain, but no oral medication (analgesics) required; 3: Severe pain: feeling pain and is no longer able to perform any type of activity, feeling the need to lie down and rest (analgesics have little or no effect on pain relief).
Seven days after the procedure, a postoperative clinical assessment was conducted to assess the condition of the periapical region using palpation and percussion routine tests. The vertical percussion test was recorded as yes or no, depending on the patient's response to the stimulus. On the second recall visit, all patients returned and pain assessment forms were reviewed.
RESULTS
In the ProTaper® group, 32(82.0%) patients reported no pain after the first 24 h, 5(12.8%) experienced mild pain, and 2(5.1 %) reported moderate pain, but none reported severe pain; 37(94.8%) patients did not present any kind of pain and 2(5.1 %) individuals reported mild pain after 72 h. Seven days after the endodontic treatment, 38 (97.4 %) individuals reported no pain and only 1 (2.5 %) reported mild pain. The percussion test was performed on the endodontically treated tooth 7 days after the clinical intervention. Only two individuals responded positively to this test, corresponding to 5.1 % of the total sample.
In the Reciproc group, 33 (84.6 %) individuals reported no pain after the first 24 h, 3 (7.7 %) experienced mild pain, and 3 (7.7 %) reported moderate pain, but none reported severe pain; 38 (97.4 %) individuals reported no pain and only one (2.5 %) reported moderate pain after 72 h; no patients reported any kind of pain 7 days after the endodontic treatment. No patients responded positively to the percussion test 7 days after treatment.
The intensity of pain experienced by patients after endodontic treatment in the Reciproc group was similar to those in the ProTaper group (p > 0.05). In both groups, the highest levels of postoperative pain were recorded 24 h after each procedure, but these levels decreased after 72 h and 7 days after endodontic therapy, although differences were not significant (p = 0.55).
CONCLUSION
No significant difference (p > 0.05) in postoperative pain was found between patients who had been treated using either the ProTaper® or the Reciproc® instrumentation technique during endodontic treatment in this study.
IMPLICATIONS FOR PRACTICE
The occurrence of postoperative pain was low and similar between the reciprocating and rotary techniques during the time intervals assessed in this RCT. These results are different from basic laboratory studies that affirm that the reciprocating techniques tend to promote more postoperative pain since extrusion of debris is greater.
ACRONYMS
VRS: verbal rating scale
Reference
1. Relvas, J.B.F., Bastos, M.M.B., Marques, A.A.F. et al. Assessment of postoperative pain after reciprocating or rotary NiTi instrumentation of root canals: a randomized, controlled clinical trial. Clin Oral Invest 2016:20: 1987. [ Links ]
