










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.71 no.7 Johannesburg Ago. 2016
CLINICAL WINDOWS
What's new for the clinician? Summaries of and excerpts from recently published papers
V Yengopal
BChD, MChD (Community Dentistry) Stellenbosch. Department of Community Dentistry, School of Oral Health Sciences, University of the Witwatersrand. E-mail: Veerasamy.Yengopal@wits.ac.za
1. Do adolescents who are night owls have a higher risk of dental caries? - a case-control study
Lundgren A-M, Öhrn K, Jönsson B. Int J Dent Hygiene. 2016; 14: 220-225
Tooth decay is amongst the most common diseases in the world affecting more than 90% of the world population.1
Dental caries in adult, adolescent and child populations thus remains a major public health problem in most communitites around the world despite a significant input of resources in the last few decades.
The risk of developing caries is associated with physical, biological, environmental, behavioural and lifestyle-related factors such as inadequate salivary flow, high number of cariogenic bacteria, frequent intake of food or drinks containing sugar, insufficient fluoride exposure, poor oral hygiene and poverty.1 As dental caries is mainly related to the individual's lifestyle, and to behavioural factors within a person's control, it can be prevented by good dietary habits in combination with tooth brushing with fluoride toothpaste twice daily.1 Many adolescents have neither breakfast nor lunch, and they consume too little fruit and vegetables. Furthermore, the consumption of soft drinks and sweets has increased in the last decades. A frequent intake of soft drinks and candy, and a low consumption of fruit and vegetables, increases the risk of an inadequate intake of nutrients and hence an elevated risk of health problems such as caries.
Circadian rhythm is the internal body clock that regulates biological processes in a 24 hour cycle. This internal clock is controlled by two pin-head sized structures in the brain called the suprachiasmatic nucleus or SCN.
The SCN ensures certain body functions work in harmony with our sleep-wake cycle including body temperature, urine production, and hormone secretion like melatonin which is key to helping us sleep. Those who have a rhythm of 24 hours or more, and so belong to the evening sleep-cycle group, might want to postpone their sleep. These evening people are alert in the evening and tired in the morning. People belonging to the morning group have a short circadian rhythm, close to 24 hours. Morning people are more tired in the evening and more alert in the morning.1
As the morning approaches, the body begins to wake up as certain hormone levels change, body temperature rises and the metabolism starts to use carbohydrates as energy.1 If people are not hungry in the morning, it may be due to eating late the night before or because they have been forced to wake up earlier than is natural for their particular circadian rhythm. For people who have a stable circadian rhythm and regular meal habits, hunger will occur at about the same time every day.
Circadian rhythm changes throughout life, and during puberty, morning tiredness is more common than it is later in life. During the teen years, a substantial shift in circadian rhythms takes place and the proportion categorized as evening types increases.1 Young people who stay up late are seldom in phase with the daily rhythm of the rest of society. When it is time to wake up and go to school, they are often tired and not hungry; and therefore, most of them probably choose to stay in bed as long as possible and skip their breakfasts.
Lundgren and colleagues (2016) in Sweden reported on a case-control study that sought to investigate the correlation between dietary habits, oral hygiene behaviour, circadian rhythm and dental caries among adolescents.1
MATERIALS AND METHODS
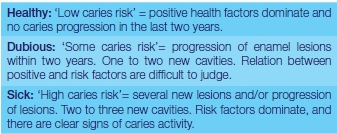
This was a comparative cross-sectional, case-control study. Adolescents, 15 to 16 years old, who were regular patients at the Public Dental Service clinics in Sweden with one dental health examination scheduled for the year ahead, and categorized as healthy (control) or sick (case) at the clinical examination the year before were considered for inclusion in this study. Exclusion criteria were as follows: individuals with a general disease that might influence the development of dental caries, those who were dependent on others for their daily oral hygiene, and individuals who did not understand Swedish. The patient's dental hygienist or dentist assessed the risk category of each individual and after examination and assessment of their history were classified as: healthy, dubious and sick.
The case group was made up of adolescents categorized as sick (high caries risk) and with two to three new caries lesions documented in their patient records at their previous examinations. The control group was categorized as healthy (low caries risk) and caries-free, that is, no registered decayed or filled teeth in their patient records (decayed-filled-teeth/surface (DFT/DFS) level = 0). The consecutive inclusion continued until both groups were equally large (n=130 in each group) and evenly distributed with regard to gender.
Participants filled in a 31 item questionnaire regarding self-reported oral health, tiredness, sleeping habits, diet, breakfast habits, tooth brushing behaviour and background and demographic data. The instrument consisted of seven items, which dealt with preferences and habits concerning activities and time. The participants were categorized into three groups based on circadian rhythm: evening types, neutral types and morning types, based on the mean value of the sum of the seven questions. A mean value between 1.0 and 2.0 was categorized as evening type, between 2.01 and 2.99 as neutral type, and between 3.0 and 4.0 as morning type.
In the analysis of each question regarding the circadian rhythm, different response options were distributed into four numbers, where "1" was regarded as extreme evening options, "2" and "3" neutral options, and "4" extreme morning options. The relationship between circadian rhythm, case and control, tooth brushing behaviour and breakfast habits were analysed with chi-square test.
RESULTS
A total of 196 individuals of the 260 invited adolescents completed the questionnaire. Of these, 95 (48.5%) were girls and 101 (51.5%) were boys. Of the sample, 91 (46%) individuals were categorized as case (sick) and 105 (54%) were categorized as control (healthy). No statistically significant correlation could be found between case/control and gender.
The mean circadian rhythm score for evening people was 1.73 (SD 0.04), neutral people, 2.48 (SD 0.02) and morning people, 3.14 (SD 0.03). Neutral types made up the most common category n = 97 (50%) followed by evening types n = 72 (37%) and morning types n = 27 (13%). Many of the evening type respondents (82%) reported that they were tired daily or almost daily at school compared with neutral types (53%) and morning types (35%) (P < 0.001). No statistically significant correlation could be found between circadian rhythm and gender.
In the case group, a significantly higher proportion were evening types (22%) compared with the group of caries-free individuals (14%). More individuals in the control group were neutral types or morning types than in the case group (P = 0.003). Around 13% of the adolescents who were evening types reported that they brushed their teeth less often than twice a day compared with 4% of the morning types. Significantly more adolescents among neutral types and morning types brushed their teeth twice daily (P = 0.01). Breakfast habits differed between the circadian rhythm types; 41% of the adolescents who were neutral types reported that they had breakfast every day compared with 22% of evening types. Significantly more individuals among evening types skipped breakfast than did those among morning types and neutral types (P = 0.003).
A total of 143 (74%) adolescents brushed their teeth twice daily, and 141 (72%) had breakfast regularly. In the control group, 88 (62%) adolescents reported that they brushed their teeth twice a day or more compared with 55 (38%) of the adolescents in the case group (P = 0.001). Breakfast habits differed between the case and control group; 53 (38%) of the adolescents in the case group reported that they had breakfast every day compared with 88 (62%) of the adolescents in the control group (P = 0.001).
When the effects of variables associated with dental caries were analysed simultaneously in a binary logistic regression, being an evening person, not having breakfast regularly and tooth brushing less than twice daily were all factors significantly associated with having a high risk of caries (categorized as sick). Belonging to the evening group was the variable most closely associated with having a high risk of caries. The predicated probability of having a high risk of caries (categorized as sick) was almost four times higher for an evening type person than for a morning type individual (OR 3.8; 95% CI 1.3-10.9).
CONCLUSION
The authors found that adolescents who described themselves as evening types brushed their teeth more seldom, did not have breakfast regularly and had a higher caries risk than morning types. A patient's circadian rhythm ought to be considered when planning oral health education for adolescents with a high risk of caries.
IMPLICATIONS FOR PRACTICE
Different circadian rhythms have been found to affect young people's general health. Information on circadian rhythms should be included in oral health education programmes for adolescents as there is evidence that the internal clock of adolescents and their habits and lifestyle is a risk marker for caries.
ACRONYM
SCN: suprachiasmatic nucleus
Reference
1. Lundgren A-M, Öhrn K, Jönsson B. Do adolescents who are night owls have a higher risk of dental caries? - a case-control study. Int J Dent Hygiene. 2016; 14: 220-225 [ Links ]
2. The effect of water on morning bad breath: a randomized clinical trial
Van der Sluijs E, Slot DE, Bakker EWP, Van der Weijden GA. Int J Dent Hygiene 2016; 14: 124-34.
Halitosis is a general term used to describe an unpleasant or offensive odour emanating from the oral cavity. It is well accepted that the pathogenesis of oral malodour is associated with the bacterial degradation of sulphur-containing amino acids (methionine, cysteine and cystine) into volatile sulphur compounds (VSCs), the principal components of which are hydrogen sulphide (H2S), methyl mercaptan (CH3SH) and, to a lesser extent, dimethyl sulphide ((CH3)2S).1
Increased public awareness and demand for remedies for oral malodour have resulted in a substantial growth of the breath industry and a saturation of the market with breath-improving products such as mints, chewing gum, breath sprays and pills. Although some of these products provide modest breath improvement, the majority have only a short-term 'masking' effect on bad breath and are essentially ineffective.1
A malodourous breath upon awakening is a common condition known as 'morning bad breath' (MBB). This problem tends to be transient in nature, in contrast to persistent halitosis. Low salivary flow, particularly during the night, creates a favourable environment for bacterial proliferation and putrefaction and results in physiological 'morning breath', which is the most common breath complaint.1
To reduce MBB, several consumer websites suggest that rinsing with or drinking water upon awakening is effective because MBB can be caused by a dry mouth.1 The hypothesis is that drinking water helps to stimulate the production of saliva and to saturate the whole mouth.1 This home remedy is, however, not supported by any scientific evidence.
Van der Sluijs and colleagues (2016) reported on a randomized clinical trial (RCT) that sought to evaluate the effects of the use of water on MBB parameters in periodontally and systemically healthy participants.1 The secondary aim was to compare the effects of rinsing with water with those of drinking a glass of water.
MATERIALS AND METHODS
Non-dental students from different universities and colleges in and around Amsterdam who had indicated in a database that they were potentially interested in participating in clinical research were notified by email and flyer about applying for a screening appointment. Participants with self-reported MBB at least five times a week were potentially eligible for inclusion. The participants were assessed for the following eligibility criteria: age ≥18 years old; classified as systemically healthy, as assessed by the medical questionnaire, and periodontally healthy, as assessed by a Dutch Periodontal Screening Index DPSI score ≤3 and the presence of at least five teeth per quadrant. Respondents who presented with an orthodontic appliance or a removable (partial) denture or who were smokers were excluded. Additional exclusion criteria were the following: caries, any pathological alterations of the oral mucosa, pregnancy, acute sinusitis or severe oral-pharyngeal infections; any medications that can cause malodour; and a reduced salivary flow due to pathological reasons. In addition, respondents who had participated in a clinical study within the previous 30 days were not allowed to participate.
Prior to the experiment, the participants were instructed to adhere to specific lifestyle rules to avoid factors that may have influenced the oral malodour odour examination. For example, they were told not to eat spicy food or consume alcohol for a period of 48 hours before assessment.
Assessments were carried out during a single visit in the same room where pre- and post-scores were obtained before and after the allocated intervention, which was performed in another room to ensure that the examiner was blinded to the intervention. The clinical assessments were taken between 7:00am and 12:00pm for each participant during the study. Lifestyle rules requested participants to avoid spicy foods, alcohol and the use of any kinds of perfume.
The primary MBB outcome variable was the organoleptic score, which was determined by one blinded examiner who was a trained and calibrated judge. As a refresher, the judge tested the ability to distinguish odours using the Smell Identification Test®; in addition, the judge tested the ability to detect odours at low concentrations using a series of dilutions of the following substances: skatole, putrescine, isovaleric acid and dimethyl disulphide. Each participant was instructed to close his/her mouth for two minutes and then to slowly open his/her mouth at the request of the examiner. Immediately upon the mouth opening, the judge sniffed the dorsum of the tongue of the participant at a distance of approximately 3-5cm.
Participants were instructed to breathe through the nose throughout this procedure. The judge performed two consecutive organoleptic assessments, and the mean of both scores was used as the individual organoleptic score. The organoleptic scale was defined as follows: 0 = absence of odour, 1 = barely noticeable odour, 2 = slight odour, 3 = moderate odour, 4 = strong odour and 5 = extremely strong odour.
In addition, Volatile Sulphur Compound (VSC) assessments were performed using the Halimeter® RH-17 and the OralChroma™ CHM-1 using the data management software: ABIMEDICAL for Windows version 3.5.0. Prior to the study, a calibration of the apparatuses was performed according to the manufacturer's recommendations. The OralChroma™ and Halimeter® were switched on 24 hours before each visit to enable their acclimatization to the ambient air. Before the assessments, each apparatus was calibrated to approximately zero. A second examiner was responsible for operating this equipment in the absence of the organoleptic judge to avoid introducing any feedback bias to the organoleptic assessment based on the outcomes of the oral malodour equipment. Before the VSC examinations, each participant was instructed to keep his/her mouth and lips closed, to breathe through the nose for two minutes and not to swallow, which facilitated the build-up of VSCs in the oral cavity.
Upon the request of the examiner, the mouth was slightly opened. A sterile disposable syringe was inserted through this opening into the oral cavity and placed between the front teeth. The participant was instructed to avoid touching the tip of the syringe with the tongue. The piston was subsequently pulled to the very end of the syringe to fill the syringe with a breath sample from the oral cavity. The syringe was then removed from the oral cavity. Any adherent saliva was wiped off the syringe with tissue paper. A gas injection needle was connected to the tip of the syringe, and 0.5ml of the breath sample was discarded. The remaining 0.5ml of the breath sample was injected into the OralChroma™ with a single push. The VSC reading of the OralChroma™ provided the concentration values of H2S, CH3SH and (CH3)2S in (parts per billion) ppb and ng ml−1. These values were recorded separately, and chromatograms were printed for analysis.
The VSCs were also scored using a portable industrial sulphide monitor (Halimeter®). The unit was zeroed to ambient air before each measurement. A disposable straw was placed between the participant's front teeth. The participant placed his/her teeth around the straw and held his/her breath as the instrument drew air from the mouth to the sensing chamber. The operator recorded the peak concentration of VSCs, displayed in ppb. The values were recorded, and the mean of these values was determined in ppb of sulphide equivalents.
The tongue coating (thickness and colour) was examined to assess tongue coating. The tongue was assessed from the vallate papillae to the tip, that is the back third, the middle third and the front third as well as from the left to the right, that is the left third, the middle third and the right third. For each of the nine sections, discolouration and coating were visually assessed. The discolouration was scored on a scale from 0 to 4 (0=pink, 1=white, 2=yellow/light brown, 3=brown and 4 = black), and coating was scored according to thickness on a scale from 0 to 2 (i.e. 0 = no coating, 1 = light-thin coating and 2 = heavy-thick coating). Light-thin coating was scored when the pink colour underneath remained visible through the coating. Heavy-thick coating was scored if no pink colour could be observed under the coating. For each section of the tongue, more than 1/3 had to be covered to obtain a score other than 0. As a potential source of oral bacteria, the presence or absence of fissures on the tongue surface was also recorded.
The participants were also asked to provide details about their daily use of oral hygiene tools and products. In addition, their own perception of their MBB before and after the intervention was assessed using a visual analogue scale (VAS). On a 10-cm-long uncalibrated line, 0 corresponded to 'stale' and 10 corresponded to 'fresh'. The participants indicated their perception by placing a vertical mark along this line.
Due to the nature of the interventions, the participants were aware of the intervention to which they were assigned, but they were requested not to reveal this information to the examiners. The participants received and read the detailed written and illustrated instructions in a room shielded from the examiners. Based on the randomization sequence, participants were assigned to the drink or rinse group. The drink group drank 200ml water and were instructed to drink the 200ml of water calmly and gradually within the time frame that was given. The other group rinsed with 15ml water with moderate power on the cheeks, for 30 seconds. A stopwatch was used to keep track of the time of either rinsing or drinking.
RESULTS
A total of 63 participants were screened for this clinical trial; 13 were excluded and 50 participants completed the single visit.
A mean score for each of the nine sections of the tongue surface was calculated. The analysis showed no significant difference in total tongue surface discolouration scores (P=0.264) or tongue coating thickness scores (P = 0.158) between the groups.
With both regimens, tongue discolouration most frequently received a score of 2 (yellow/light brown) in the posterior- and mid-dorsal regions of the tongue. Tongue coating thickness most frequently received a score of 2 (heavy-thick) in the posterior dorsal sections of the tongue. Both tongue discolouration and tongue coating mostly received scores of 0 in the anterior sections (pink and no coating, respectively). The prevalence of tongue fissures was low in both groups (4-6%).
Both regimens yielded a significant decrease in the organoleptic score. The score reduction was 0.46 (0.51; P=0.01) in the drinking group and 0.33 (0.48; P = 0.05) in the rinsing group. There was no significant difference between the regimens at any time point, nor was the incremental change following the regimen different between the groups (P = 0.360). The correlation coefficients between tongue discolouration and organoleptic scores (P = 0.248, P = 0.083), as well as between tongue coating thickness and organoleptic scores (P = 0.175, P = 0.224), were small and not significant.
Most of the VSC outcome data measured by the Halimeter® and OralChroma™ showed a non-normal distribution. Following the two regimens, the Halimeter® outcome showed a reduction between the pre- and post-intervention results of 11.12 in the drinking group and 14.17 in the rinsing group, neither of which was significant (P = 0.884). Regarding the VSC levels as assessed by the OralChroma™ apparatus, there was a significant decrease in the levels of the two different gases, H2S and CH3SH, in both regimens. (CH3)2S showed a reverse trend, namely a non-significant increase of 10.77 in the drinking group and 23.14 in the rinsing group was found. None of the OralChroma™ outcomes related to the three gases showed a significant difference between the groups with respect to the incremental changes between pre- and post-assessments.
The mean scores and standard deviations of the subjective perception of the participants related to their MBB before and after the assigned regimen were not significantly different between the two groups. The change in the VAS score in the drinking group was 0.59 (2.00), which was not significant (P=0.146). The rinsing group perceived a change of 1.00 on the VAS scale, which proved to be statistically significant (P=0.001).
CONCLUSION
The researchers concluded that rinsing with 15 ml water or drinking a glass of 200 ml water had a statistically significant effect on the morning bad breath (MBB) parameters. No significant difference was obtained between the two regimens.
IMPLICATIONS FOR PRACTICE
This trial provided scientific efficacy for two common home "remedies" for the treatment of morning bad breath (MBB). Both drinking and rinsing with water had significant effects on the MBB outcome, with no significant difference found between the two interventions.
ACRONYMS
MBB: morning bad breath
VSCs: volatile sulphur compounds
Reference
1. Van der Sluijs E, Slot DE, Bakker EWP, Van der Weijden GA. The effect of water on morning bad breath: a randomized clinical trial. Int J Dent Hygiene 2016; 14: 124-134. [ Links ]
