










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.71 no.6 Johannesburg Jul. 2016
RESEARCH
Knowledge and beliefs about oral pseudomembranous candidiasis among traditional health practitioners in Limpopo Province, South Africa
M S NemutandaniI; S J H HendricksII; F M MulaudziIII
IChD, MChD, MPH, MSc. PhD (UP). School of Health System and Public Health, University of Pretoria, Pretoria, South Africa
IIB ChD, BTh, DipDPH, MSc, MPH, MPA, DMedSc. Extra-ordinary Professor Health Policy & Management, School of Public Health, University of Pretoria, Pretoria, South Africa
IIIBCur, BCur(Hons) MCur, DLitt et Phil. Associate Professor and Head: Department of Nursing Science, University of Pretoria, Pretoria, South Africa
ABSTRACT
INTRODUCTION: Oral pseudomembranous candidiasis (OPC) is commonly associated with immunosuppression caused by HIV/AIDS and TB infections. The knowledge and beliefs about OPC among traditional health practitioners in South Africa are not well explored.
PURPOSE: To investigate this concern.
METHODS: A cross-sectional descriptive survey was conducted in the rural Vhembe district of the Limpopo Province. Data were collected from 427 traditional health practitioners who were to attend training workshops on HIV/AIDS and TB diseases. An open-ended semi-structured questionnaire with an A4 colour picture of oral pseudomembranous candidiasis was presented to assess their previous exposure to, and their knowledge and beliefs about, the etiology and management of OPC.
FINDINGS AND CONCLUSION: Only thirteen percent correctly identified the lesion. More than 64% were uncertain on etiology, and 24% blamed witchcraft and supernatural powers. Almost two thirds (60%) were confused about the relationship between HIV/AIDS and OPC lesions.
The belief that witchcraft and ancestors could cause OPC could increase the risk of HIV infections and result in delays in seeking treatment. The outcomes of this study should be incorporated in the training of the traditional health practitioners on oral signs and symptoms of HIV/ AIDS diseases.
Keywords: Oral pseudomembranous candidiasis, knowledge and beliefs, traditional health practitioners (THPs)
INTRODUCTION
Oral pseudomembranous candidiasis (OPC), commonly called oral thrush, is an oral infection caused by yeast of the genus Candida and particularly Candida albicans.1 It is characterized by white patches on the surface of the buccal mucosa, tongue, and the soft palate.1 This condition has been observed over the years, and is typically associated with elderly patients, infants and medically compromised individuals.2Candida albicans are among the many organisms which live in the human mouth and gastrointestinal tract.3 Up to 75% of healthy individuals carry the yeast Candida as part of their normal commensal oral microflora.1-3
Since the 1980s there has been a surge of interest and associated research into OPC.4 This has largely been due to an increased incidence of OPC among immunocompro-mised patients and its association in patients infected by the human immunodeficiency virus (HIV).5-7 Oral pseudomembranous candidiasis occurred in up to 90% of HIV positive patients at some point during the course of the disease.7 More recently, with the advent of anti-retro-viral (ARV) therapy, this frequency has become very low. Manifestation is associated with high viral loads, low CD4+ T cell count (< 200 cells/mm3), increased morbidity and has been shown to negatively affect the quality of life of HIV/AIDS patients.7-10 The prolonged course of HIV infection predisposes these patients to recurrent episodes of OPC that can increase in frequency and severity with progressive HIV disease.10,11
In most African countries, including South Africa (SA), traditional health practitioners, formerly referred to as witchdoctors and /or Sangomas,12-14 play a crucial role in providing primary health delivery including taking care of people living with emerging diseases such as HIV/AIDS.15-17 Published reports indicate that between 60-90% of the population in SA consult traditional healers.18-22
Oral pseudomembranous candidiasis was present prior to the discovery of HIV/AIDS.5 It is highly likely that traditional health practitioners were, and still are, treating and taking care of patients presenting with OPC. These patients would be managed according to traditional beliefs and understanding of the source of the disease. The introduction of the Traditional Health Practitioners Act (No 22 of 2007), was aimed at legitimizing their traditional beliefs on supernatural powers and ancestors, and integrating the profession into the main health system in SA.13
In 2013, there were approximately 6.4 million persons infected with HIV/AIDS in SA.23 As the awareness among the traditional health practitioners of the association of OPC with HIV/AIDS is relatively low,21 these practitioners are likely to be managing some of the HIV patients presenting with OPC.
The purpose of this study was to determine the knowledge and belief amongst traditional healers, regarding oral pseu-domembranous candidiasis, and its associated with HIV and AIDS. This is particularly important in sub-Saharan Africa, where many people are unaware of their HIV/AIDS status, as the recognition of OPC by traditional health practitioners may result in earlier detection of AIDS and consequent referral to the allopathic health facilities for further management.
METHODS
Study setting
The study was conducted in Vhembe District, one of 52 districts of South Africa. The district is located in the Limpopo Province, and shares its borders with Zimbabwe, Botswana and Mozambique. Vhembe district has four local municipalities categorized as rural. Based on the 2015 mid-year population estimates, the district has approximately 1.6 million inhabitants, with an average life expectancy of 58.2 years.23 More than 85% of the inhabitants in this district live in tribal areas, where traditional practices, beliefs and consultation of traditional health practitioners form part of their culture.23-25
Study design and sample size
A cross-sectional descriptive survey was conducted among traditional health practitioners attending training workshops on the signs and symptoms of HIV/AIDS and TB diseases. Delegates to the training workshops were selected by their respective organisations and recommended by the Vhembe traditional Health Council and traditional leaders. Eight HIV/ AIDS training workshops were conducted between January 20 and August 30, 2014, in four local municipalities under the Vhembe district. A total of 437 traditional health practitioners attended the training workshops.
Data collection tools
The data were collected using a semi-structured questionnaire, prepared first in English and then translated into Tshivenda and Xitsonga. To maintain the consistency of the tool it was back-translated to English by two different public health professionals with a wealth of experience on indigenous knowledge systems. The main researcher administered the questionnaire. The questionnaire was pretested on ten traditional health practitioners who were attending a meeting on ritual killings in Vhembe district. The questionnaire was consequently amended and adjusted to accommodate the desired data for the study.
An open-ended semi-structured questionnaire including an A4 colour picture of OPC [Figure 1] on the palate, was used to assess the pre-training knowledge and beliefs on OPC and the socio-demographic information. Five open ended questions included: 1) What is this condition? 2) What is the cause of it? 3) Have you treated such a condition before? 4) How did/ would you manage the patient? 5) Is it associated with HIV/AIDS? The responses were captured by a research assistant who had attended the necessary training on the objective of the study, data collection techniques, procedures and instruction on how to complete the questionnaires.

Ethical consideration
Ethical clearance was obtained from the Research and Ethics Committee of the University of Pretoria (REC 3992013). Access permissions were granted by the Limpopo Provincial Health Research Council and Traditional Health Practitioners Council. A special permission to enter the traditional health practitioners' "sciences and world" was sought and granted from Wali (Supreme Being) and the holders of traditional sciences, ancestors, during the ritual ceremony (muphaso). Participation by the THP's was voluntary. All participants were informed that they could withdraw from the study at any time. Literate participants gave their consent through signing. Those who were illiterate agreed to participate in front of a representative of the traditional health practitioners.
Statistical analysis
The data were entered into Excel and exported to Stata 11 (Stata Cooperation). The descriptive findings were depicted in tables and graphs. For the response to the five open-ended questions, the "general inductive approach" was used to analyse the qualitative data. A coding scheme was established based on a preliminary analysis of a representative sample of the material, without any references to an existing theory or framework.26 Repetitive reading of the responses to the open ended questions was done, aimed at providing an understanding of the data in context. Twenty percent of the responses were read and coded by the researcher and research assistant together. Emerging responses were determined and coded accordingly. The remaining data was coded using the determined coding.
RESULTS
Demographic characteristics of traditional health practitioners (THP)
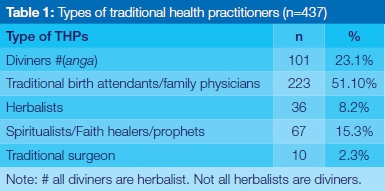
A total of 437 THPs were interviewed. The largest numbers of traditional health practitioners were diviners (23%) and family practitioners (51%). These are traditional healers who perform divination (throwing of bones or ancestral channeling), or who were family protectors (u vhea mui) and birth attendants. There were 36 (8.2%) respondents who used their knowledge of plants, herbs and animal products to cure illnesses. Spiritualists, including the faith healers, prophets and fortune tellers (u femba), accounted for 77 (17.6%) of the sample. There were a few traditional surgeons (2.3%), and all were males, responsible for male circumcisions (Table 1).
With regard to gender, almost two- thirds were female. Half of the traditional health practitioners were above 60 years of age, 32.9% were between 41 and 60 years old; whilst 10 (2.3%) were minors (below 18 years of age). Almost thirty-five percent (34.8%) of the sample reported that they had no formal education, 178 (40.7%) reported that their highest level of education was primary school. Only 43(9.8%) traditional health practitioners had achieved senior certificate level and 14 (3.2%) had a tertiary qualification.
Their years of experience as traditional health practitioners varied from less than 5 years (18.5%), between 6 -10 years (22.2%), 11-20 years (31.8%) and 21 years and more years (27.5%). Almost all participants (93. 4%) reported that this was their first attendance of a HIV/AIDS and TB training workshop. Almost 90% of traditional health practitioners reported not knowing their HIV status.
The response of the respondents with regard to the questions on OPC is summarised below.
Knowledge on the OPC and the causes of it
Thirteen percent of the participants were able to identify the lesion as OPC. The majority of those who correctly identified the lesions were diviners, followed by herbalists and faith-based healers. Their description of the lesion in indigenous terminology- "mahada' (white snow covering the surface) and "Vhudaadaa" (distress of speech associated with pain), was similar to what an allopathic health practitioner would call an OPC. A larger percentage (71.8%) indicated that they were unsure about this condition.
The knowledge regarding the aetiology of OPC varied. More than 64.3% were not sure about the causes of this lesion. Almost a quarter (24.4%) of the respondents thought that OPC was caused by witchcraft and supernatural powers such as evil spells and ancestors. One THP stated that... "these are diseases caused by ancestors". The majority of those who associated OPC with witchcraft and supernatural powers were diviners and prophets. The diagnoses and treatment process of these categories of THPs involve communication with supernatural powers. Only 5.9% of the total sample of respondents thought that OPC has to do with underlying diseases and infections.
Previous exposure to OPC and its management
Almost half (46%) of the respondents did not recall seeing patients with such lesions. Among those who had seen patients presenting with OPC, a small number had referred their patients (38%) to other THPs, whilst others (57%) managed the patients using herbal medicine.
Association of OPC with HIV/AIDS
The knowledge on the association of OPC with HIV/AIDS infections was assessed. A small percentage of THPs (15.3%) reported that OPC may be as a result of HIV/AIDS infections. Almost double that percent (24.6%) said that there was no relationship with HIV/AIDS whilst sixty percent (60.1%) were unsure about any relationship.
DISCUSSION
Characteristics of traditional health practitioners
The profession of the traditional health practitioner has been practiced for centuries in Africa, long before western medicine became the dominant health system. Their knowledge and practice of the medicinal use of herbs, roots, and other items has been passed down through generations. It is acquired during their ancestral calling to become a traditional health practitioner (thwasana).27-30
A call to become a traditional health practitioner could start at any age and may present in different ways including unexplained illness, constant headaches, dreams and nightmares associated with ancestors and, loss of weight.31,32 Unlike in the Western medical schools, becoming a traditional health practitioner does not follow selection criteria such as grades achieved at high schools, entry level examination, prescribed age limit etc. The majority of THPs were women between 41 and 60 years with no formal education (34.8%). This compared well with Vhembe District Profile, which reported that over 53% of the district's population were female, with little or no formal education.23 In 2002, Bereda found that a much higher percentage (59%) of her participants were not educated.33 This may influence the findings as lower levels of education have been found to correlate with lower level of knowledge of transmission, treatment and prevention of HIV/AIDS and TB.34 It has also been demonstrated that black people generally tend to have poorer HIV/AIDS knowledge due to low literacy levels associated with a lack of exposure to formal education.34
The fact that more than two-thirds of the respondents (75%) had limited basic literacy suggests that extra measures and cautions should be considered in the planning, developing and alignment of the training materials to ensure appropriate relevance.
The wealth of experience and depth of knowledge of traditional medicine and patient management is derived from ancestral spirits incarnated during their initiation process (u wisiswa). The knowledge and practice of herbs, roots, and other medicine has passed down through generations. Compared with allopathic health professionals who are required to attend continuous training and updating on the latest medical developments, the traditional practitioner is expected to comply with the ancestral spirit that called them to become THPs.15,35 In a Western paradigm these fields and practices are considered backwards, unscientific, erroneous and potentially harmful.35 Lack of collaboration and inadequate formal referral between the two health systems could result in patients having drug overdoses, over treatment or drug interactions.
Knowledge and beliefs on the causes of OPC
It was noted that most of the THPs were not able to identify OPC. This was not surprising, as an intra-oral examination on "healthy" patients presenting with no oral health complaints is probably not a common practice among THPs. Having said that, OPC is one of the most common oral lesions associated with HIV/AIDS patients.36,37 Unless the patient has secondary infections such as gingivitis and periodontitis, OPC is generally not painful, and the patients may not be aware that s/he has a lesion. Recent findings by Ramphoma and Naidoo38 revealed that even the oral health care workers working in well-resourced facilities were not vigilant enough in checking for oral lesions. Some of them were unable to correctly identify oral lesions associated with HIV/AIDS as they lacked adequate knowledge of these lesions.
This reported low knowledge level of OPC is comparable to a study conducted by Rudolph et al39 almost 10 years ago. They found that only 22.4% of 63 THPs knew about OPC. Ensuring the ability of THPs to recognise and identify that these lesions are associated with HIV/AIDS infections provides a golden opportunity to engage them in the fight against HIV/AIDS.
A question on "what is the cause of these lesions" revealed their beliefs in supernatural powers and the depth of traditional medicine. These responses were most probably the reflection of the past and present prevailing beliefs among THPs, especially amongst diviners and prophets. A quarter of the respondents (24.4%) believed that OPCs was caused by evil forces and ancestors. The explanation offered on what is thought to be the cause of OPC appeared to link with the indigenous name for it: vhudaadaa, which has been described above as "distress of speech associated with pain". When literally translated this Venda word means that "one is not sure". When one is unsure of the cause- it becomes vhudaadaa. This group of THPs could not explain the cause and origin of the lesion.
The other meaning, "distress of speech associated with pain", could be associated with the fact that OPC was seen among the immunocompromised patients and in infants, who were unable to vocalise at all. The appearance of OPC in a six-month old child may not, however, herald a serious condition. It could be as a result of a transition period wherein the child is developing his/her own immunity and teeth are erupting in the mouth. However, the underlying cause should always be determined to rule out the possibility of a serious commensurate condition such as diabetes or immunosup-pression caused by HIV/AIDS and other serious infections, of which both the patient and THP may not be aware. Any training course on HIV/AIDS should take into account the relevance of linking HIV/AIDS infections and OPC and the importance of contextualising the relevance of indigenous names and their meaning in the past and now.
Management and the relationship of OPC to HIV/ AIDS infections
The management of illness and diseases among THPs has usually been in line with an understanding of the cause of the disease. It was therefore not surprising to note that most of the THPs chose to refer their patients to AHPs (78.3%). This may be a positive result in the sense that THPs understand their role and recognise that some conditions are outside their expertise/ healing methods. It is also positive in that such a referral may address the underlying medical conditions such as HIV/AIDS, diabetes and other immunocompromising diseases.
Only 13.0% preferred to use herbal medicine to manage their patients. If in doubt, patients would be referred to other THPs (8.7%) for treatment or for a second opinion, and possibly to specialist traditional health practitioners. No further questions were posed on the questionnaire to explore why OPC patients were referred to AHPs and how it was being done, whether it was self-referral, or accompanying patients. A referral to an AHP appears to be very significant in that THPs recognise that allopathic and traditional medicine have to coexist. It signals the right approach to collaboration with AHPs. A small gesture of recognition and acknowledgment from AHPs to THPs for referring patients to the clinics could be seen as the beginning of the change in attitudes and mind-set.15,16
A small percentage of THPs knew that patients presenting with OPC (15.3%) may be as a result of HIV/AIDS infections, which suppresses the immune system. More than 60% of the THPs were not sure about the relationship between HIV/AIDS and OPC. It may be expected that their knowledge in this area is poor, considering that more than 90% of respondents had not attended any workshops. Although this study provides the baseline information for future interventions, this should be a matter of great concern for health authorities as OPC has been known to occur in up to 90% of HIV positive patients.7 This has changed in the past few years with the introduction of ARVs.
Assessing the knowledge and management of these lesions by THPs could assist HIV/AIDS and TB trainers to understand traditional beliefs and practices related to OPC. As both the diagnosed and un-diagnosed HIV patients consult THPs at various stages of the diseases, the training of the THPs on OPC could alert them to refer their patients for confirming laboratory tests. Greater awareness may also encourage patients to check their HIV status and to take the necessary precautions to prevent spreading the disease.
The training and the involvement of THPs in the management of HIV/AIDS patients has been a thorny issue.15-17 Flint and Payne argued that the training of THPs in SA on HIV/ AIDS will assist in the fight against HIV/AIDS infections.15 Homsy and others suggested that trained THPs are key to scaling up comprehensive care for HIV/AIDS.17
Despite the calls made by WHO33 for integration, the facts that AHP are university trained and use evidence as determined by Western medicine whilst THP are selected on a calling and practice traditional healing, may make it a challenge for these healers to co-exist.32,35 However, taking into account that the THPs may be the first contact for patients seeking care, it is incumbent on the AHP to understand THP, their knowledge, practices and beliefs. This understanding should inform the development of the relevant educational interventions that, combined, would promote the health of the population which is a responsibility of the health (and other) sectors.13,33
Certain traditional practices could increase THPs risk of contracting HIV. It is common practice for THPs to use bare hands (ungloved) to apply topical medicine on open wounds and sores such as Herpes Zoster, thought to be caused by ancestors. Many also utilize their mouths to suck blood from their patient's body as part of disease management.34 Lack of knowledge of infection control and no access to hand gloves may result in THPs handling HIV/AIDS-related lesions directly.
The researchers believe that engagement with THPs on best alternative practices and the sharing of knowledge through collaboration could help prevent further spread of HIV and TB infections. Collaboration with THPs may require a change of attitudes and mind sets of the AHPs, and a recognition that THPs also have a role to play in the delivery of health care in SA. It is through exposure and sharing of information that attitudes may change.
CONCLUSION AND RECOMMENDATIONS
This study has shown that despite the low knowledge level and etiology of OPC amongst THP's, they are nevertheless managing OPC without knowing that it may be as a result of HIV/AIDS.
Noting that the majority of patients consult THPs on a daily basis, and the fact that South Africa is experiencing an HIV/AIDS and TB pandemic, urgent focus should be given to conducting further training workshops for THPs on the signs and symptoms of HIV/AIDS and TB diseases.
The existing beliefs that witchcraft and ancestors were the causes of OPC, could well delay patients from seeking allopathic treatment early.
Some patients were referred to AHPs, clearly demonstrating the need for constructive engagement and training workshops to exchange knowledge and information in both directions.
The researchers recommend that HIV/AIDS and TB training workshops be initiated to target the beliefs of THPs on the cause of OPC and to instruct on management practices. AHPs also need exposure to traditional medicine. The starting point may be the inclusion of a traditional medicine module in the curriculum of AHP students and engaging with THPs during training.
LIMITATIONS
Traditional medicine is mostly based on an acceptance of supernatural powers of the ancestors. The diagnosis and treatment modalities are directed and inspired by ancestors in the consulting rooms inhabited by ancestors. Traditional health practitioners are secretive, ancestor-respecting people and could be providing data designed to simply please the interviewer, as they were not within their normal environment to consult ancestors for diagnosis and treatment. However, they could also have been advantaged to hear whispering answers from ancestors, having been in a spiritual and subjective state during the interview. This could result in information bias, unfair advantage and selection bias. The sample size was also relatively small due to limited resources.
Conflict of interests: None declared
ACRONYMS
AHP: Allopathic Health Practitioner
ARV: anti-retro-viral
OPC: oral pseudomembranous candidiasis
THPs: Traditional Health Practitioners
Acknowledgements
The South African Medical Research Council (SAMRC) and National Health Scholarship Programme (NHSP) are gratefully acknowledged for financial support. The authors would like to thank the following people: the respondents and the general community in Vhembe district, Maine M. Vhengani, Maine T. Ramatshimbila and Dr E Klu.
Disclaimer: Any opinion, findings and conclusions or recommendations expressed in this material are those of the authors and therefore, the SAMRC and NHSP do not accept any liability in this regard.
References
1. Giannini PJ, Shetty KV. Diagnosis and management of oral candidiasis. Otolaryngol Clin North Am. 2011; 44(1):231-40. [ Links ]
2. Muzyka BC. Oral fungal infections. Dent Clin North Am. 2005; 49(1):49-65. [ Links ]
3. Ng S. Managing patients with oral candidiasis. J Can Dent Assoc 2013; 79: d122. [ Links ]
4. Bodey G P. Fungal infection and fever of unknown origin in neutropenic patients. Am J Med. 1986; 80:112-9. [ Links ]
5. Gold J W M. Opportunistic fungal infections in patients with neoplastic disease. Am J Med. 1984; 76:458-63. [ Links ]
6. Horn R, Wong B, Kiehn T E. Fungemia in a cancer hospital: changing frequency, earlier onset, and results of therapy. Rev Infect Dis. 1985; 7:646-55. [ Links ]
7. Egusa H, Soysa NS, Ellepola AN, Yatani H, Samaranayake LP. Review of oral candidosis in HIV-infected patients. Curr HIV Res. 2008 Nov; 6(6):485-99. [ Links ]
8. Samaranayake LP, Fidel PL, Naglik JR. Fungal infections associated with HIV infection. Oral Dis. 2002; 23(Suppl 2):151-60. [ Links ]
9. Diro E, Feleke Y, Guteta S, Fekade D, Neway M. Assessment of risk behaviours and factors associated with oral and peri-oral lesions in adult HIV patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. Ethiop J Health Dev. 2008; 22:180-6. [ Links ]
10. Campo J, Del Romero J, Castilla J, Garcia S, Rodriguez C, Bascones A. Oral candidiasis as a clinical marker related to viral load, CD4 lymphocyte count and CD4 lymphocyte percentage in HIV-infected patients. J Oral Pathol Med. 2002; 31:5-10. [ Links ]
11. Badiee P, Alborzi A, Davarpanah MA, Shakiba E. Distributions and antifungal susceptibility of Candida species from mucosal sites in HIV positive patients. Arch Iran Med. 2010 Jul; 13(4):282-7. [ Links ]
12. Parrinder G. Witchcraft: European and African. Faber and Faber; London, UK: 1963. [ Links ]
13. The Traditional Health Practitioners Act, Act 22 of 2007. Pretoria: Government printers. Republic of South Africa, 2007. [ Links ]
14. Witchcraft Suppression Act, No. 3 of 1957, Government Printers, Pretoria, Republic of South Africa. 1957. [ Links ]
15. Flint AG, Payne JR. Reconciling the irreconcilable? HIV/AIDS and the potential for middle ground between the traditional and biomedical healthcare sectors in South Africa. Forum Develop. Stud. 2013; 40:47-68. [ Links ]
16. Audet CM, Hamilton E, Hughart L, Salato J. Engagement of traditional healers and birth attendants as a controversial proposal to extend the HIV health workforce. Curr Opin HIV/AIDS Rep. 2015; 12(2):238-45. [ Links ]
17. Homsy J, King R, Balaba D, Kabatesi D. Traditional health practitioners are key to scaling up comprehensive care for HIV/AIDS in sub-Saharan Africa, Editorial Comment AIDS. 2004; 18:1723-5. [ Links ]
18. Babb DA, Pemba L, Seatlanyane P, Charalambous S, Churchyard GJ, Grant AD. Use of traditional medicine by HIV- infected individuals in South Africa in the era of antiretroviral therapy. Psychol Health Med. 2007; 12(3):314-20. [ Links ]
19. Peltzer K, Preez NF, Ramlagan S, Fomundam H. Use of traditional complementary and alternative medicine for HIV patients in KwaZulu-Natal, South Africa. BMC Public Health. 2008; 8:255-7. [ Links ]
20. Peltzer K, Mngqunaniso N. Patients consulting traditional health practitioners in the context of HIV/AIDS in urban areas in KwaZulu-Natal, South Africa. Complement. Alter. Med. 2008; 5:370-9. [ Links ]
21. Gail H, Tarryn B, Oluwaseyi A, Denver D, Oluchi M, Charlotte VK, Joop de J, Diana G. An ethnobotanical survey of medicinal plants used by traditional health practitioners to manage HIV and its related opportunistic infections in Mpoza, Eastern Cape Province, South Africa. J Ethnop-harmacol. 2015; 171:109-15. [ Links ]
22. Malangu N. Self-reported use of traditional, complementary and over-the-counter medicines by HIV-infected patients on antiretroviral therapy in Pretoria, South Africa. Afr J Trad CAM. 2007; 4:273-8. [ Links ]
23. Statistics South Africa. 2015 Mid-Year Population Estimates. South African. [ Links ]
24. Matshidze PE. The role of Makhadzi in traditional leadership among the Venda. Unpublished Ph.D thesis, University of Zululand, KwaDh-langezwa, KwaZulu-Natal. 2013. [ Links ]
25. Mafukata MA. Mandevu. Journal of Arts and Humanity. 2015; 4(1):14-26. [ Links ]
26. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. American Journal of Evaluation, 2006; 27(2):237-46. [ Links ]
27. Conley RJ. Cherokee Medicine Man: The Life and Work of a Modern-Day Healer. University of Oklahoma Press; Norman, OK, USA: 2005. [ Links ]
28. Brownlee F. Some experiences of native superstition and witchcraft. Afr. Affairs. 1940; 39:54-60. [ Links ]
29. Lett J. "Science, religion, and anthropology." Anthropology of Religion: A handbook (1997): 103-20. [ Links ]
30. Semenya SS, Potgieter MJ. Bapedi traditional healers in the Limpopo Province, South Africa: their socio-cultural profile and traditional healing practice. J Ethnobiol Ethnomed. 2014.10:4-9. [ Links ]
31. Stuttaford M, Al Makhamreh S, Coomans F, Harrington J, Himonga C, Hundt GL. The right to traditional, complementary, and alternative health care. Global Health Action. 2014; 7:10-8. [ Links ]
32. Struthers S, Eschiti V.S, Patchell B. Traditional indigenous healing: Part I. Complement. Ther. Nurs. Midwifery. 2004; 10:141-9. [ Links ]
33. Bereda JE. Traditional healing as a health care delivery system in a transcultural society. M.A. Dissertation. Pretoria: University of South Africa. 2002. [ Links ]
34. Shisana O, Zungu-Dirwayi N, Toefy Y, Simbayi LC, Malik S, Zuma K. Marital status and risk of HIV infection in South Africa. S Afr Med J. 2004; 94(7):537-43. [ Links ]
35. Flint AG. Traditional healing, biomedicine and the treatment of HIV/AIDS: contrasting South African and Native American experiences. J Environ Res Public Health. 2015; 12(4): 4321-39. [ Links ]
36. Obileye MF, Agbelusi GA, Orenuga OO, Temiye EO. Immune suppression and oral manifestations of HIV in a group of Nigerian children. West Afr J Med. 2014; 33(4):270-5. [ Links ]
37. Muller K, Kazimiroff J, Fatahzadeh M, Smith RV, Wiltz M, Polanco J, Grossberg RM, Belbin TJ, Strickler HD, Burk RD, Schlecht NF. Oral human papillomavirus infection and oral lesions in HIV-positive and HIV-negative dental patients. J Infect Dis. 2015; 212(5):760-8. [ Links ]
38. Ramphoma KJ, Naidoo S. Knowledge, attitudes and practices of oral health care workers in Lesotho regarding the management of patients with oral manifestations of HIV/AIDS. SADJ. 2014; 69(10):446, 448-53. [ Links ]
39. Rudolph MJ, Ogunbodede EO, Mistry M. Management of the oral manifestations of HIV/AIDS by traditional healers and care givers. Curationis. 2007; 30(1):56-61. [ Links ]
 Correspondence:
Correspondence:
M Simon Nemutandani
Department of Community Dentistry, University of Limpopo, Limpopo Province, South Africa
Tel: +27 15 287 5473, Cell: +27 83 301 5505
E-mail: ve2si@yahoo.com or ve22si@gmail.com
