










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.71 no.6 Johannesburg Jul. 2016
CLINICAL REVIEW
Oral diseases associated with human herpes viruses: Aetiology, clinical features, diagnosis and management
R BallyramI; NH WoodII; RAG KhammissaIII; J LemmerIV; L FellerV
IBDS, MDS. Department of Periodontology and Oral Medicine, Sefako Makgatho Health Sciences University, Pretoria, South Africa
IIBChD, DipOdont (MFP), MDent(OMP). Department of Periodontology and Oral Medicine, Sefako Makgatho Health Sciences University, Pretoria, South Africa
IIIBChD, PDD, MSc(Dent), MDent (OMP). Department of Periodontology and Oral Medicine, Sefako Makgatho Health Sciences University, Pretoria, South Africa
IVBDS, HDipDent, FCD(SA)OMP, FCMSAae, Hon. FCMSA. Department of Periodontology and Oral Medicine, Sefako Makgatho Health Sciences University, Pretoria, South Africa
VDMD, MDent(OMP). Department of Periodontology and Oral Medicine, Sefako Makgatho Health Sciences University, Pretoria, South Africa
ABSTRACT
Human herpesviruses (HHVs) are very prevalent DNA viruses that can cause a variety of orofacial diseases. Typically they are highly infectious, are contracted early in life, and following primary infection, usually persist in a latent form. Primary oral infections are often subclinical, but may be symptomatic as in the case of herpes simplex virus-induced primary herpetic gingivostomatitis. Reactivation of the latent forms may result in various conditions: herpes simplex virus (HSV) can cause recurrent herpetic orolabial lesions; varicella zoster virus (VZV) can cause herpes zoster; Epstein-Barr virus (EBV) can cause oral hairy leukoplakia; and reactivation of HHV-8 can cause Kaposi sarcoma. In immunocompromised subjects, infections with human herpesviruses are more extensive and severe than in immunocompetent subjects. HSV and VZV infections are treated with nucleoside analogues aciclovir, valaciclovir, famciclovir and penciclovir. These agents have few side effects and are effective when started early in the course of the disease. This article highlights the diagnosis, clinical features and management of HHV-associated oral diseases, particularly of those most likely to be encountered by the general dental practitioner.
Key words: herpes simplex virus, human herpes virus-8, varicella zoster virus, Epstein-Barr virus, recurrent herpes labialis, recurrent intraoral herpetic ulcers, treatment, val-aciclovir, aciclovir, famcicylovir
INTRODUCTION
The human herpesvirus (HHV) family comprises a diverse group of DNA viruses that, following a primary infection, have the capacity to persist life-long in a latent form. The latent HHVs can undergo reactivation, particularly in subjects with immunosuppressive or debilitating conditions, causing subclinical infection with a low-rate of viral replication or causing frank clinical infection.1-3
The HHV family members comprise the herpes simplex virus (HSV) type 1 (HSV-1) also termed human herpes virus type 1 (HHV-1) and the herpes simplex virus type 2 (HSV-2, HHV-2); the varicella-zoster virus also termed human herpes virus type 3 (VZV, HHV-3); the Epstein-Barr virus (EBV, HHV-4); the cytomegalovirus (CMV, HHV-5); the more recently characterized HHV-6, HHV-7; and HHV-8.1,2,4-7
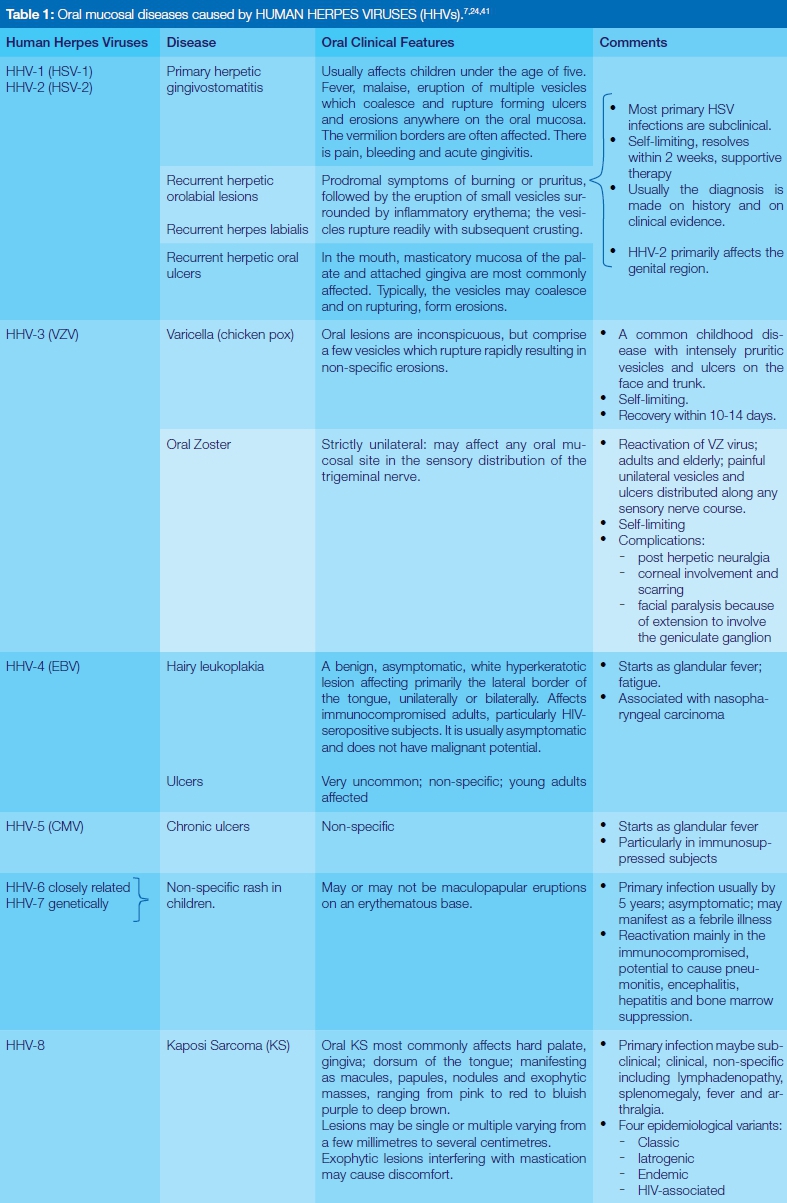
Any HHV can cause asymptomatic subclinical infection, or clinical infection with or without oral manifestations (Table 1). During active productive infection, depending on the site of replication of the virus, viral particles are shed in saliva, genital secretions, urine, tears or respiratory secretions making HHVs readily transmissible and infectious.6,7
Following primary oral infection with HSV or VZV the viruses ascend in sensory neurons from peripheral nerve endings adjacent to the infected epithelium to the trigeminal ganglia where they become latent. Upon reactivation the viruses descend within sensory neurons from the trigeminal ganglia and are released at the nerve endings whence they migrate into the oral epithelium and replicate, causing productive infection that often develops into viral lesions.5,8,9
Epstein-Barr virus (EBV) infects B lymphocytes and oropha-ryngeal epithelial cells where, following primary infection, they persist in latent form.5,10 CMV is believed to infect and establish latent infection in salivary gland cells, endothelial cells, macrophages, lymphocytes, and possibly in haematopoietic progenitor cells.1,3-6 The closely related HHV-6 and HHV-7 infect and establish latency in CD4+T lymphocytes. HHV-8 infects B lymphocytes where subsequently it persists in latent form and upon reactivation replicates in B lymphocytes and endothelial cells.5,11,12
The aim of this paper is to provide the general dental practitioner with a succinct review of the clinical features and diagnosis of the more common HHV-induced oral diseases and to discuss their management and pharmacothera-peutic treatment.
ORAL MUCOSAL DISEASES CAUSED BY HHVs
Herpes simplex viruses cause primary herpetic gingivos-tomatitis, recurrent herpes labialis and, less commonly, recurrent intraoral ulcers, together termed recurrent herpetic orolabial lesions.13 It appears that when primary infection with HSV-1 occurs in childhood, it manifests as herpetic gingivostomatitis; but later it may present as oro-pharyn-gotonsillitis.6 However, most HSV-1 primary infections are subclinical and are acknowledged only when recurrent oro-labial herpetic infection occurs without a history of earlier primary herpetic gingivostomatitis14 (Table 1). Primary her-petic gingivostomatitis should be differentiated from other conditions with oral vesicles or ulcers, including erythema multiforme, herpes zoster, hand foot and mouth disease and herpangina.7
Herpes labialis can be frequently recurrent, painful and persistent and is usually triggered by febrile illness, sunburn, minor trauma, emotional stress or hormonal changes of menstruation (Table 1). Recurrent herpes labialis appears to occur more frequently in white skinned post-adolescent non-smoking females.9,15
Recurrent intra-oral herpetic ulcers need to be differentiated from oral herpes zoster and from aphthous ulcers.7 While intra-oral herpetic ulcers usually affect the kerati-nized masticatory mucosa, aphthous ulcers usually affect the nonkeratinized lining mucosa.
HSV has also been implicated in the pathogenesis of erythema multiforme which is an acute, immune-mediated mucocutaneous condition. It is estimated that up to 70% of cases of erythema multiforme are associated with HSV, and that in susceptible subjects the periodic reactivation of HSV triggers the recurrence of erythema multiforme.16,17 It was always thought that herpetic infections of the oral, oropharyngeal and ocular mucosa, and of the skin above the waist, were caused by HSV-1; while HSV-2 caused infections of the anogenital mucosa and of the skin below the waist. Transmission of HSV-1 was associated with close non-sexual contact with an infected subject, and HSV-2 with sexual contact. However, owing to the increase in the practice of orogenital sex, there has been a rise in the frequency of oral and oropharyngeal infection caused by HSV-2, and of anogenital infection caused by
HSV-1. Whether caused by HSV-1 or HSV-2, the oral lesions are the same. The prevalence of HSV-1 and HSV-2 is higher in developing than in developed countries.6,8,18,19
VZV causes chicken pox and zoster (shingles); EBV causes oral hairy leukoplakia, non-specific oral ulcers and is associated with nasopharyngeal carcinoma and a subset of lymphomas; and CMV is associated with salivary gland dysfunction and non-specific oral ulcers. The effect of HHV-6 and HHV-7 infections on the oral mucosa is unknown, but HHV-8 is a critical factor in the pathogen-esis of Kaposi sarcoma (Table 1).7,11 As a rule, the extent and severity of primary and recurrent HHV infections are greater in immunocompromised than in immunocompe-tent subjects.13,20
There is some supportive evidence for the role of HHVs in the pathogenesis of periodontal disease as DNA particles and gene products can be detected in lesions of periodontal diseases. It is likely that productive subclinical HHV infection of the periodontium can dysregulate local periodontal immune responses and interfere with normal healing and tissue remodelling.21-23
DIAGNOSIS
Diagnosis of HSV and VZV-induced oral diseases is usually based on the clinical presentation and on the medical history. Histopathological examination of a biopsy specimen, if deemed necessary, would show ballooning degeneration of infected epithelial cells, inclusion bodies, fusion of cells to form syncytia of multinucleated giant epithelial cells, as well as acantholysis with the formation of Tzanck cells. The most common and cost-effective laboratory method of confirming the clinical diagnosis, however, is by microscopic examination for the presence of multinu-cleated giant cells or of large cells with ballooned nuclei in a smear preparation from the base of a lesion.6,7,24 These features are similar in both HSV and VZV induced lesions. If necessary, further differentiation between HSV and VZV can be done by immunofluorescent studies, and typing of the viruses present in the lesion can be determined by immunohistochemistry, in situ hybridization or polymerase chain reaction (PCR).4,6,7,13,24
Diagnosis of EBV-induced oral hairy leukoplakia or of HHV-8-induced oral Kaposi sarcoma is also based largely on the clinical features of the lesions, on the medical history and on microscopic examination of a biopsy specimen.
The characteristic microscopic features of hairy leukopla-kia are epithelial hyperplasia, acanthosis, hyperkeratosis, presence of koilocyte-like cells, but with little or no inflammatory cell infiltrate in the underlying lamina propia.10
Kaposi sarcoma exhibits atypical vascular channels, sheets and fascicles of spindle cells forming nodular tumour like masses, extravasated red blood cells and an inflammatory cell infiltrate. HHV-8 DNA can be demonstrated in oral Kaposi sarcoma cells by PCR or by immunohistochemical methods.11,20,25
TREATMENT
Most HHV diseases are self-limiting and resolve within 7-10 days; but in order to alleviate the symptoms of primary herpetic gingivostomatitis, recurrent orolabial HSV infection, primary oral VZV infection, and oral herpes zoster, all are generally treated non-specifically and supportively with antimicrobial mouthwashes (chlorhexidine by choice), analgesic, soft diet and adequate intake of fluids.6,7,24
In immunocompromised or debilitated subjects, or in immunocompetent subjects with persistent, unusually painful, or frequently recurrent HHV infections, systemic antivirals are necessary (Tables 2 and 3).6,7,24,26,27 Drug treatment will not only shorten the course of the disease, but will also reduce the duration of virus shedding and will promote healing.1 In these subjects, recurrent orola-bial herpetic lesions are usually larger and run a more severe clinical course than in immunocompetent subjects. In subjects with AIDS, the larger herpetic ulcers mimic major aphthous ulcers or necrotizing stomatitis so histopatho-logical or cytological examination may be necessary for diagnosis and PCR or in-situ hybridization may reveal the presence of several different HHVs.6
The most commonly used antiviral agents in the treatment of oral HSV or VZV infections are the nucleoside analogues, aciclovir, valaciclovir, famciclovir and penciclovir (Table 3). These agents inhibit viral DNA polymerization and disrupt the viral DNA synthesis and replication, while having only a minimal effect on the host-cellular DNA synthesis.2,14,18,24,28 Long-term use of antivirals does not seem to cause the emergence of drug resistant viruses. Valaciclovir and famciclovir have a greater bioavailabil-ity when taken orally and consequently are administered less frequently per day than aciclovir. However, as the effectiveness of these drugs when taken according to the prescribed dosing schedule is similar, and as aciclovir is substantially less expensive, it is the most frequently prescribed first-line antiviral agent.29-32
As a rule, treatment with systemic or topical antiviral agents should be started as early as possible in the course of symptomatic HSV and VZV infections, as this may minimize or prevent the development of new lesions, accelerate resolution and significantly shorten the period of viral shedding.6,7,15
Factors to be considered in deciding whether or not to use antiviral agents for the treatment of symptomatic HSV and VZV oral infections, which are usually self-limiting, include the severity and extent of the disease, the duration of the condition since the onset (according to the patient), the age of the patient, the fitness of the immune system as deduced from the history and the potential side effects of the drugs.15,33 Those who will benefit most from the use of antiviral agents are immunocompromised subjects, or im-munocompetent subjects with a history of frequent, painful and persistent episodes of recurrent orolabial HSV infection or of VZV infections. In such cases, systemic agents are more effective than topical agents in reducing the duration of signs and symptoms and in promoting healing.15
Antiviral drugs are best started in the prodromal or early stage of viral infection, so any patient with a history of frequent recurrent orolabial herpes infection should be provided with a small stock of the selected antiviral drug so that treatment can be started promptly at the onset of recurrence, avoiding the delay of professional consultation and prescription. However, self-diagnosis, and the potential adverse effects of self-medication are issues of some concern.15
PRIMARY HERPETIC GINGIVOSTOMATITIS
Active herpetic lesions are highly infectious so anyone with primary herpetic gingivostomatitis should avoid close contact with others to prevent transmission and spread of the virus; and should be aware of the hazards of auto-inoculation.6
In those cases of primary herpetic gingivostomatitis when pharmacotherapeutic agents are necessary, the recommended drug regimens are as in Tables 2 and 3. Treatment is best if started within the first three days of onset of the disease.1,6,7,34
RECURRENT HERPETIC OROLABIAL LESIONS
Recurrent herpes labialis, also termed 'cold sore' or 'fever blister', affects the vermilion border and the immediately surrounding skin and is the most common clinical manifestation of recurrent HSV-1 infection. Up to 50% of subjects will experience at least one episode of recurrent herpes labialis.1,18
Aciclovir 5% cream or penciclovir 1% cream when applied topically, if possible eight times a day from the start of the prodrome reduces morbidity and promotes healing.6-8,35 For management of severe recurrent herpes labialis, see Tables 2 and 3.8,36
When recurrent herpes labialis is triggered by exposure to sunlight during skiing or sunbathing, prophylactic use of aciclovir 400mg twice per day, valaciclovir 1g per day or famciclovir 250mg twice per day, together with the use of sunscreen for the duration of the vacation is generally effective.6,8 When episodes of apparently spontaneous recurrent infection are frequent and debilitating, occurring more than six times a year, long-term prophylactic treatment with antiviral agents, such as aciclovir 400mg twice per day or valaciclovir 500mg once daily for 4-12 months should be considered. Side-effects of long-term use of these agents are minimal33 (Table 2).
Sometimes, for unknown reasons, herpetic lesions occur following a local anaesthetic injection in the hard palate. When there is a history of this having occurred, then 2g valaciclovir taken twice on the day of the anticipated injection in the palate, and 1g taken twice on the next day has been reported to prevent or limit the herpetic eruption6,18,37 (Table 2).
HSV-ASSOCIATED AND IDIOPATHIC ORAL ERYTHEMA MULTIFORME
HSV-associated recurrent erythema multiforme (EM) is indirectly induced by an immune response to subclinical or clinical HSV infection, and some cases, putatively idiopathic EM may also be provoked by HSV, as might be demonstrated by appropriate molecular investigations. In general, prophylactic treatment against HSV infection for 6-12 months may be beneficial for subjects who have experienced several episodes of recurrent HSV-associated or idiopathic EM per year. Suppression of HSV replication by aciclovir 400mg, or valaciclovir 500mg or famciclovir 250mg twice daily will prevent or reduce the frequency of the EM. However, treatment with antiviral agents has no effect on the clinical course of overt EM.
ORAL HERPES ZOSTER
Antiviral agents started within 72 hours of the development of the first oral zoster vesicles may reduce both the severity and the duration of the infection and minimise the risk of post herpetic neuralgia.1,7,37 Recommended drug regimens are as in Table 2.
THE RISK OF HSV TRANSMISSION AND ITS IMPLICATIONS FOR ORAL HEALTH-CARE PERSONNEL
As discussed earlier, reactivation of latent HSV in the trigeminal sensory ganglion with consequent replication of the virus in the oral or perioral epithelium may manifest clinically as recurrent orolabial herpetic lesions; but HSV infection usually occurs asymptomatically and subclinically. In both clinical and subclinical infections there is shedding of the virus from the oral epithelium into the oral fluids.6-8,38
Clinical and virological research have shown that about 6% of subjects free of clinical oral HSV infection nevertheless shed HSV-1 into their oral fluids on any given day and that about 70% shed the virus at least once a month.38 In healthy immunocompetent subjects each episode of HSV-1 shedding lasts for one to three days and is increased by local trauma or inflammation. In immunocompromised subjects the frequency, duration and quantity of oral shedding of HSV is increased. The load of HSV-1 in the infected oral fluids, even in the case of subclinical infections is sufficient to make the saliva a vehicle of potential viral transmission.38 The viruses in oral fluids may be dispersed in aerosols generated by normal breathing, coughing or spitting and by kissing or food sharing.3 However, although HSV is highly transmissible, most recipients of the transmitted virus will not develop HSV disease.6,7
Recurrent orolabial herpetic infection is a potential occupational hazard for oral health care workers. Their risk of infection is particularly high when aerosols are generated by high-speed rotatory and ultrasonic instruments even if the patient has subclinical HSV infection.39 Therefore, the importance of universal infection control measures cannot be overemphasized, and elective dental and oral treatment of patients with overt clinical orolabial herpetic disease should be deferred.40
Herpetic whitlow, that is a primary or recurrent HSV infection of the finger, may result from self-inoculation in subjects with primary or recurrent orolabial or genital HSV infection; or in the case of oral health care workers from treating patients with active herpetic infection. Indeed, before the introduction of universal precautions against infection, dentists had a higher frequency of herpetic whitlow than the general population.6,40
CONCLUDING REMARKS
HSV and VZV infections of oral and perioral tissues are usually self-limiting requiring only supportive treatment.
However, susceptible subjects can have frequent, persistent and disabling episodes of these oral infections, and prophylactic treatment with systemic antiviral agents are usually helpful.
Conflict of interest: None declared.
ACRONYMS
EM: erythema multiforme
HHV: human herpes virus
PCR: polymerase chain reaction
HSV, HHV-1: herpes simplex virus
VZV, HHV-3: varicella-zoster virus
EBV, HHV-4: Epstein-Barr virus
CMV, HHV-5: cytomegalovirus
References
1. Evans CM, Kudesia G, McKendrick M. Management of herpesvirus infections. Int J Antimicrob Agents 2013;42:119-28. [ Links ]
2. Weller SK, Kuchta RD. The DNA helicase-primase complex as a target for herpes viral infection. Expert Opin Ther Targets 2013;17:1119-32. [ Links ]
3. Grinde B. Herpesviruses: latency and reactivation - viral strategies and host response. J Oral Microbiol 2013;5 doi 10,3402/jom,v510.22766. [ Links ]
4. Balasubramaniam R, Kuperstein AS, Stoopler ET. Update on oral herpes virus infections. Dent Clin North Am 2014;58:265-80. [ Links ]
5. Feller L, Lemmer J, Meyerov R. The association between human herpesviruses and periodontal disease: Part 1. Herpesviruses immune evasion. A review. SADJ 2007;62: 8-9. [ Links ]
6. Neville BW, Damm DD, Allen AM, Chi AC. Viral infections. In: Falk K, editor. Oral and Maxillofacial Pathology. St Louis, Missouri, USA: Elsevier; 2016. 218-58. [ Links ]
7. Scully C. Herpesvirus infection. In: Taylor A, Watt L, editors. Oral and Maxillofacial Medicine,The Basis of Diagnosis and Treatment. London, United Kingdom: Elsevier; 2013. 277-85. [ Links ]
8. Woo SB, Challacombe SJ. Management of recurrent oral herpes simplex infections. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103 Suppl:S12 e1-8. [ Links ]
9. Raborn GW, Grace MG. Recurrent herpes simplex labialis: selected therapeutic options. J Can Dent Assoc 2003;69:498-503. [ Links ]
10. Khammissa R, Fourie J, Chandran R, Lemmer J, Feller L. Epstein-Barr Virus and its association with oral hairy leukoplakia: A short review. Int J Dent 2016:Article ID 4941783. [ Links ]
11. Feller L, Wood NH, Lemmer J. Herpes zoster infection as an immune reconstitution inflammatory syndrome in HIV-seropositive subjects: a review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:455-60. [ Links ]
12. Feller L, Wood NH, Khammissa RA, Chikte UM, Meyerov R, Lemmer J. HPV modulation of host immune responses. SADJ 2010;65:266-8. [ Links ]
13. Arduino PG, Porter SR. Herpes Simplex Virus Type 1 infection: overview on relevant clinico-pathological features. J Oral Pathol Med 2008;37:107-21. [ Links ]
14. Simpson D, Lyseng-Williamson KA. Famciclovir: a review of its use in herpes zoster and genital and orolabial herpes. Drugs 2006;66:2397-416. [ Links ]
15. Cunningham A, Griffiths P, Leone P, Mindel A, Patel R, Stanberry L, et al. Current management and recommendations for access to antiviral therapy of herpes labialis. J Clin Virol 2012;53:6-11. [ Links ]
16. Staikuniene J, Staneviciute J. Long-term valacyclovir treatment and immune modulation for herpes-associated erythema multiforme. Cent Eur J Immunol 2015;40:387-90. [ Links ]
17. Sokumbi O, Wetter DA. Clinical features, diagnosis, and treatment of erythema multiforme: a review for the practicing dermatologist. Int J Dermatol 2012;51:889-902. [ Links ]
18. Rahimi H, Mara T, Costella J, Speechley M, Bohay R. Effectiveness of antiviral agents for the prevention of recurrent herpes labialis: a systematic review and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;113:618-27. [ Links ]
19. Wald A, Ericsson M, Krantz E, Selke S, Corey L. Oral shedding of herpes simplex virus type 2. Sex Transm Infect 2004;80:272-6. [ Links ]
20. Feller L, Lemmer J, Wood NH, Jadwat Y, Raubenheimer EJ. HIV-associated oral Kaposi sarcoma and HHV-8: a review. J Int Acad Periodontol 2007;9:129-36. [ Links ]
21. Slots J, Contreras A. Herpesviruses: a unifying causative factor in periodontitis? Oral Microbiol Immunol 2000;15:277-80. [ Links ]
22. Contreras A, Zadeh HH, Nowzari H, Slots J. Herpesvirus infection of inflammatory cells in human periodontitis. Oral Microbiol Immunol 1999;14:206-12. [ Links ]
23. Feller L, Meyerov R, Lemmer J. The association between human herpes viruses and periodontal disease, Part 2. SADJ 2007;62:170, 2, 4. [ Links ]
24. Regezi JA, Sciubba JJ. Vesiculo-Bullous Diseases. In: Dyson J, editor. Oral Pathology Clinical-pathological Correlations. Philadelphia, USA: W.B. Saunders Company; 1989. 1-28. [ Links ]
25. Feller L, Lemmer J. Oral Kaposi sarcoma. In: Pantanowitz L, Stebbing J, Dezube BJ, editors. Kaposi Sarcoma: A Model of Carcinogenesis. India: Research Signpost; 2010. 295-303. [ Links ]
26. Durso SC. Oral manifestations of disease. In: Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson LJ, et al., editors. Harrisons Principles of Internal Medicine: McGraw Hill Medical; 2008. 214-20. [ Links ]
27. Marques ER, Cohen JI. Herpes Simplex. In: Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff K, editors. Fitzpatricks's Dermatology in General Medicine. USA: Mc Graw-Hill; 2012. 2367-82. [ Links ]
28. Antonelli G, Turriziani O. Antiviral therapy: old and current issues. Int J Antimicrob Agents 2012;40:95-102. [ Links ]
29. Bhalekar MR, Upadhaya PG, Reddy S, Kshirsagar SJ, Madgulkar AR. Formulation and evaluation of acyclovir nanosuspension for enhancement of oral bioavailibility. Asian J Pharm 2014;8:110-8. [ Links ]
30. Granero GE, Amidon GL. Stability of valacyclovir: implications for its oral bioavailability. Int J Pharm 2006;317:14-8. [ Links ]
31. Hoglund M, Ljungman P, Weller S. Comparable aciclovir exposures produced by oral valaciclovir and intravenous aciclovir in immunocompromised cancer patients. J Antimicrob Chemother 2001;47:855-61. [ Links ]
32. Danve-Szatanek C, Aymard M, Thouvenot D, Morfin F, Agius G, Bertin I, et al. Surveillance network for herpes simplex virus resistance to antiviral drugs: three-year follow-up. J Clin Microbiol 2004;42:242-9. [ Links ]
33. Szenborn L, Kraszewska-Glomba B, Jackowska T, Duszczyk E, Majda-Stanislawska E, Marczynska M, et al. Polish consensus guidelines on the use of acyclovir in the treatment and prevention of VZV and HSV infections. J Infect Chemother 2016;22(2):65-71. [ Links ]
34. Amir J, Harel L, Smetana Z, Varsano I. Treatment of herpes simplex gingivostomatitis with aciclovir in children: a randomised double blind placebo controlled study. BMJ 1997;314:1800-3. [ Links ]
35. Spruance SL, Nett R, Marbury T, Wolff R, Johnson J, Spaulding T. Acyclovir cream for treatment of herpes simplex labialis: results of two randomized, double-blind, vehicle-controlled, multicenter clinical trials. Antimicrob Agents Chemother 2002;46:2238-43. [ Links ]
36. Cernik C, Gallina K, Brodell RT. The treatment of herpes simplex infections: an evidence-based review. Arch Intern Med 2008;168:1137-44. [ Links ]
37. Arduino PG, Porter SR. Oral and perioral herpes simplex virus type 1 (HSV-1) infection: review of its management. Oral Dis 2006;12:254-70. [ Links ]
38. Miller CS, Danaher RJ. Asymptomatic shedding of herpes simplex virus (HSV) in the oral cavity. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:43-50. [ Links ]
39. Ramalho KM, Rocha RG, Correa-Aranha AC, Cunha SR, Simoes A, Campos L, et al. Treatment of herpes simplex labialis in macule and vesicle phases with photodynamic therapy. Report of two cases. Photodiagnosis Photodyn Ther 2015;12:321-3. [ Links ]
40. Browning WD, McCarthy JP. A case series: herpes simplex virus as an occupational hazard. J Esthet Restor Dent 2012;24:61-6. [ Links ]
41. McCarthy FP, Shklar G. Virus diseases of the oral cavity. In: McCarthy FP, Shklar G, editors. Diseases of the Oral Mucosa. New York: McGraw-Hill; 1964. 77-88. [ Links ]
42. Corey L, Whitley RJ, Cohen JI. Infections due to DNA viruses. In: Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson LJ, Loscalzo J, editors. Harrison's Principles of Internal Medicine. USA: McGraw Hill; 2015. 1175-89. [ Links ]
 Correspondence:
Correspondence:
Liviu Feller
Head:Department of Periodontology and Oral Medicine Sefako Makgatho
Health Sciences University, Pretoria, South Africa, 0204
Tel: 012 5214834, Fax: 012 5214833
E-mail: liviu.feller@smu.ac.za

{kind=link}
{kind=link}
{kind=link}