










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.71 no.6 Johannesburg Jul. 2016
CASE REPORT
Management of an inflamed dentigerous cyst in a patient with an anterior cross-bite, using a modified obturator
D SardanaI; A GoyalII; K GaubaIII
IBDS,MDS. Division of Paediatric Dentistry, Centre for Dental Education & Research, All India Institute of Medical Sciences, New Delhi, India
IIBDS, MDS. Professor,Unit of Paediatric Dentistry, Oral Health Sciences Centre, Post-graduate Institute of Medical Education and Research, Chandigarh, India
IIIBDS, MDS. Professor and Chair, Unit of Paediatric Dentistry, Oral Health Sciences Centre, Post-graduate Institute of Medical Education and Research, Chandigarh, India
ABSTRACT
Dentigerous cysts, amongst the most common odontogenic cysts occurring in children, are caused by the accumulation of fluid between the reduced enamel epithelium and the crown of the tooth. Both developmental and inflammatory aetiologies have been postulated. Enucleation and marsupialisation have remained the mainstay treatment modalities of such cysts although the former is a more radical option- especially in young children with unerupted and developing permanent teeth. A case of an inflammatory dentigerous cyst (IDC) in an 8-year old patient with an anterior dental cross-bite is presented. This was managed by marsupialisation of the cyst and concurrent correction of the anterior cross-bite (within 3 months) using a modified obturator. This treatment modality had the advantage of reducing the treatment time as well as obviating the need for a second appliance. There was no recurrence of either dentigerous cyst or cross-bite at a one-year follow up.
INTRODUCTION
The dentigerous cyst is one of the most common odontogenic cysts and develops due to obstruction of venous drainage by pressure of the erupting tooth on the follicle and consequently an accumulation of fluid between the reduced enamel epithelium and the crown of the tooth.1,2 The cysts are most frequently associated with the mandibular third molar, maxillary canine, mandibular premolars and maxillary third molar teeth, in decreasing order of frequency.3 The mandibular second premolar is the most commonly involved tooth in the 0-9 year old age-group and the permanent maxillary canine has this distinction in the 10-19 year old age-group.4,5 A diagnostic feature is the absence of the affected tooth in the oral cavity.5 The cyst is usually asymptomatic and thus may be diagnosed incidentally on routine radiographs. A cyst may attain a large size, causing resorption of the roots of nearby teeth before it manifests clinically or becomes evident radiographically. Although most dentigerous cysts are considered to be of developmental origin, some seem to have an inflammatory pathogenesis. It is impossible to determine histopathologically whether the inflammatory component is primary or secondary in nature.7 An unusual case of IDC in the right mandibular premolar area, together with an anterior cross-bite involving 12, 21 and 22, is presented in which both cyst and cross-bite were managed conservatively using a simple appliance (modified obturator).7
CASE REPORT
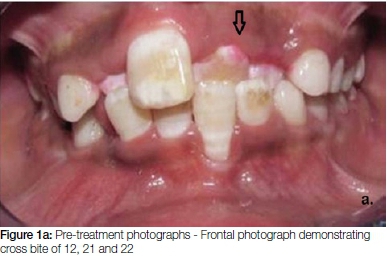
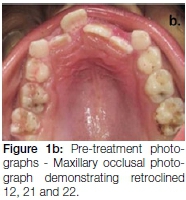
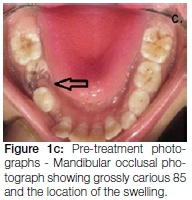
An 8-year-old male patient reported to the Unit of Paediatric Dentistry, Oral Health Sciences Centre Post-graduate Institute of Medical Education & Research, Chandigarh, with a chief complaint of a swelling in the mouth on the right side, first noticed two months previously. The patient gave a history of intermittent pain in that area for the past 15 days. The pain was moderate in nature and subsided on the taking of analgesics. Physically, the patient was healthy and there were no signs of any systemic disorder. Extra-orally, no swelling was visible in the right mandibular area; however on palpation a bony hard swelling was felt which was slightly tender and non-fluctuant. The sub-mandibular and sub-mental lymph nodes were not palpable and temporomandibular joint movements were found to be smooth and well coordinated. Intra-orally, the patient was in the early mixed dentition stage of dental development with active caries on 55, 65, 26, 36, 75, 85 and 46 (Figure 1, a-c). The dentition exhibited generalized fluorotic stains. Teeth 84 and 85 were mobile and the bony hard, slightly tender, swelling was felt in the buccal vestibule. There was no sign of a draining sinus associated with the swelling. Teeth 12, 21 and 22 were in a cross-bite relationship with the lowers. The vulnerable labial muco-gingival tissues showed inflammatory enlargement, but there was Class I gingival recession associated with the labial displacement of tooth 31 (Figure 1, a-c). Testing this tooth for fremitus was negative with no mobility. An orthopantomogram was taken which showed a unilocular radiolucency extending from distal surface of 42 to mesial surface of 46. There was displacement of the unerupted 43 and 44 and the roots of 84 and 85 showed premature resorption (Figure 2a). Based on the clinical signs and symptoms, a provisional diagnosis of dentigerous cyst was reached. Considering the age of the patient and the underlying unerupted and displaced 43 and 44, a conservative treatment plan was adopted which consisted of marsupialisation of the lesion by creating a window through the extraction sockets of 84 and 85 and the provision of an acrylic obturator to maintain its patency.


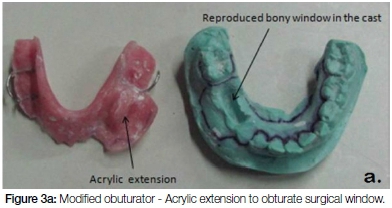
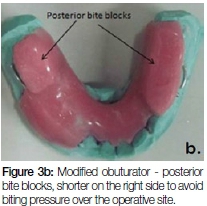
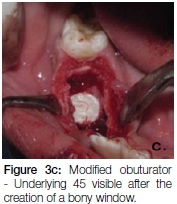
Impressions of the patient's upper and lower arches were taken. The plaster renditions of teeth 84 and 85 were ground off the poured cast. The bony window was reproduced in the cast and an acrylic extension into the cavity was made to serve as the obturator (Figure 3a). It was decided to modify the obturator by incorporating bilateral posterior acrylic bite blocks (Figure 3b) to dis-occlude the anterior teeth, allowing for possible self-correction of the anterior cross-bite. At surgery, the 84 and 85 were extracted, the cyst was marsupialised (Figure 3c) and its lining sent for histopathological examination. The obturator was fitted immediately post-surgery.
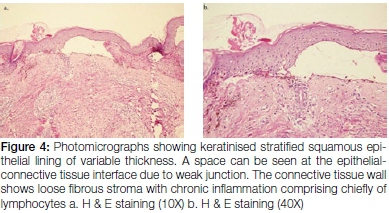
Histopathologic examination (Figure 4) revealed a keratinized stratified squamous epithelial lining of variable thickness. A space could be seen between epithelium and the connective tissue due to a weak junction. The connective tissue wall showed loose fibrous stroma with chronic inflammation comprised chiefly of lymphocytes. Based on the histopathologic findings a definitive diagnosis of IDC was made.
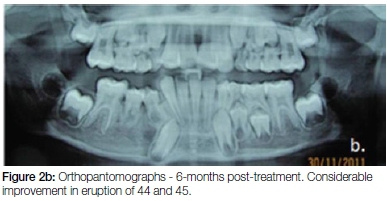
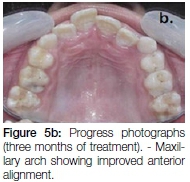
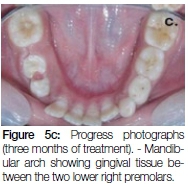
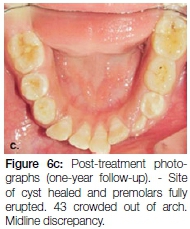
The patient was recalled daily for seven days postopera-tively for irrigation of the socket with betadine and saline. The parents of the patient were taught how to irrigate the socket with these solutions and how to ensure the maintenance of good oral hygiene. Thereafter the patient was recalled fortnightly and periodic trimming of the acrylic extension was done to facilitate eruption of 44 and 45. After three months (Figure 5, a-c), anterior crossbite correction was observed along-with progressive eruption of 44 and 45. The 43 appeared to be improving in its path of eruption. The patient was then advised to discontinue the obturator. Follow-up after one year showed complete eruption of 44 and 45, and no relapse of the crossbites or recurrence of the dentigerous cyst (Figure 2c and Figure 6, a-c).



DISCUSSION
The inflammatory aetiology for dentigerous cysts was first mentioned as early as 1928 by Bloch-Jorgensen8 who suggested that all follicular cysts originated due to the overlying necrotic deciduous teeth. The suggested pathogenesis of such cysts was the spread of periapical inflammation from the roots of the deciduous teeth to involve the follicle of the unerupted permanent successor, producing inflammatory exudates which resulted in the formation of the dentiger-ous cyst. The role of persistent and prolonged inflammation irritating the dental sac of an unerupted tooth thereby causing a dentigerous cyst has also been suggested by other authors.9 Benn and Altini10 indicated that at least two types of dentigerous cysts occur. The first type is purely developmental in origin and occurs in mature teeth usually as result of impaction. The second type is inflammatory in origin and occurs in immature teeth as a result of periapical inflammation from a preceding non-vital deciduous tooth, or other source, spreading to involve the tooth follicle. Benn and Altini10 considered three possible mechanisms in the histogenesis of inflammatory dentigerous cysts:
1. Intra-follicular developmental cysts formed around the crowns of permanent teeth that become secondarily inflamed, as a result of periapical inflammation spreading from non-vital deciduous predecessors.
2. Radicular cysts at apices of nonvital deciduous teeth that fuse with the follicles of unerupted permanent successors. "Eruption" of successor teeth into the cystic cavity results in the formation of the extra-follicular den-tigerous cyst.
3. Periapical inflammation from any source, but usually from nonvital deciduous teeth, spreading to involve follicles of unerupted permanent successors.
Inflammatory dentigerous cysts are only found in the mixed dentition and involve the permanent teeth. Radio-graphically, they may appear as round or ovoid, well demarcated unilocular radiolucencies with a sclerotic border within the mandible. IDCs are usually associated with the roots of a non-vital or necrotic deciduous tooth and the crown of an unerupted permanent tooth.11
Histologically, dentigerous cysts of typical non-inflammatory origin are lined by thin non-keratinized stratified squamous epithelium. However, many variations in the thickness of the lining epithelium may be noted depending on type and severity of any subsequent inflammation present.1,12
The choice of treatment should be based on the size and location of the cyst, age of the patient, affected dentition, and the relationship with surrounding vital structures.13 These factors along-with operator skill and preference, determine whether enucleation or marsupialisation of such cysts may be performed. Enucleation is the process mostly indicated for small cysts in which the cyst is completely removed without rupturing. However, for larger cysts this procedure may result in fracture of the mandible, devitalization of the associated teeth, or the loss of indispensable impacted teeth associated with the lesion. Thus, enucleation should be performed when there is no likelihood of damaging anatomic structures such as the apices of vital teeth, maxillary sinus, neuro-vascular bundles and developing permanent teeth.
The treatment of IDCs includes extraction of the non-vital primary tooth and marsu-pialisation of the cyst, as illustrated in this case. Marsupialisation consists in creating a surgical cavity through the wall of the cyst, emptying its content, and maintaining continuity between the cyst lining and the oral cavity, maxillary sinus, or nasal cavity, whichever is more closely related.14 This technique is indicated for large cysts or cysts associated with unerupted teeth in geriatric and pediatric patients or in patients with systemic diseases.14 This allows healing of the cystic cavity and eruption of the permanent tooth in paediatric patients, provided that these procedures are performed at the normal time of eruption. The main advantage of this procedure over enucleation is its simplicity and a more conservative approach, inflicting less surgical trauma. Since a major disadvantage of marsupialisation is that pathologic tissue is left in situ, a thorough histologic examination is essential.15,16
An obturator is also required to decompress the cystic lesion, maintain patency of the surgical opening and prevent entry of food debris into the cystic cavity.17 Although this technique is found to be quite successful, full compliance with recommended postoperative oral hygiene measures is critical.
In this case, posterior bite blocks were incorporated in the obturator bilaterally to dis-occlude the anterior teeth and assist in self-correction of cross bite of the lin-gually locked maxillary incisors. The main advantage of this modification is that it obviated the need for a second appliance to correct the cross bite. The appliance was also easily constructed although speech and mastication difficulties were of concern to the patient for the first few days, after which he became accustomed to manipulating the device. The results of the modified obturator were encouraging and the one year follow-up did not show any sign of recurrence of the cyst or relapse of the cross bite. The lower right first molar has drifted mesially and further orthodontic treatment remains a requirement to deal with crowding, overjet, midline discrepancy and impaction of the lower right canine.
Conflict of interests: None declared
ACRONYMS
IDC: inflammatory dentigerous cyst
References
1. Browne RM. The pathogenesis of odontogenic cysts: A review. J Oral Pathol. 1975;4:31-46. [ Links ]
2. Freitas DQ, Tempest LM, Sicoli E, Lopes-Neto FC. Bilateral dentigerous cysts: review of the literature and report of an unusual case. Dentomaxillofac Radiol 2006;35:464-8. [ Links ]
3. Jones AV, Craig GT, Franklin CD. Range and demographics of odontogenic cysts diagnosed in a UK population over a 30-year period. J Oral Pathol Med 2006, 35: 500-7. [ Links ]
4. Bernick S. Dentigerous cysts of the jaw. Oral Surg Oral Med Oral Pathol 1949;2:914-21. [ Links ]
5. Ericson S, Bjerklin K, Falahat B. Does the canine dental follicle cause resorption of permanent incisor roots? A computed tomographic study of erupting maxillary canines. Angle Orthod 2002;72:95-104. [ Links ]
6. Johnson LM, Sapp JP, McIntire DN. Squamous cell carcinoma arising in a dentigerous cyst. J Oral & Maxillofac Surg1994;52:987-90. [ Links ]
7. Neville BW, Damm DD, Allen CM, Bouquot J. Oral and Maxillofacial Pathology (2nd ed). Saunders 2002;590-93. [ Links ]
8. Bloch-Jorgensen K. Follicular cysts. Dent Cosmos 1928;70:708-11. [ Links ]
9. Azaz B, Shteyer A. Dentigerous cysts associated with second mandibular bicuspids in children: Report of five cases. ASDC J Dent Child 1973;40:29-31. [ Links ]
10. Benn A, Altini M. Dentigerous cysts of inflammatory origin. A clinic-pathologic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;81:203-9. [ Links ]
11. Kozelj V, Sotosek B. Inflammatory dentigerous cysts of children treated by tooth extraction and decompression--report of four cases. Br Dent J 1999;187:587-90. [ Links ]
12. Shafer WG, Hine MK, Levy BM. A Textbook of Oral Pathology. Philadelphia: WB Saunders Company; 1993. p. 154-8. [ Links ]
13. Motamedi MH, Talesh KT. Management of extensive dentigerous cysts. Br Dent J 2005;198: 203-6. [ Links ]
14. Nishide N, Hitomi G, Miyoshi N. Irrigational therapy of a dentigerous cyst in a geriatric patient: A case report. Spec Care Dentist 2003;23:70-2. [ Links ]
15. Takagi S, Koyama S. Guided eruption of an impacted second premolar associated with a dentigerous cyst in the maxillary sinus of a 6-year-old child. J Oral Maxillofac Surg 1998;56:237-9. [ Links ]
16. Ellis E. Surgical management of oral pathologic lesions. In: Peterson LJ, Ellis E, Hupp JR, Tucker MR, eds. Contemporary Oral and Maxillofacial Surgery. 4th ed. St Louis: Mosby; 2002:479-502. [ Links ]
17. Delbem AC, Cunha RF, Vieira AE, Pugliesi DM. Conservative treatment of a radicular cyst in a 5- year-old child: A case report. Int J Paediatr Dent 2003;13:447-50. [ Links ]
 Correspondence:
Correspondence:
Divesh Sardana
Division of Paediatric Dentistry, Centre for Dental Education & Research
All India Institute of Medical Sciences, New Delhi, India
E-mail: doc_divesh@yahoo.co.in
