










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.71 n.5 Johannesburg Jun. 2016
RESEARCH
The development of a physiotherapy intervention programme for mandibular condyle fracture patients
Anke van der MerweI; Roline BarnesII
IBSc Physiotherapy (Stell) MSc Physiotherapy (UFS). Lecturer, Department of Physiotherapy, University of the Free State
IIBSc Physiotherapy (UFS) MSc Physiotherapy (UFS). Department Head, Department of Physiotherapy, University of the Free State
ABSTRACT
INTRODUCTION: The need for physiotherapy in the treatment of mandibular condyle fractures has been highlighted, but there has been no agreement regarding an exercise programme for these patients.
AIMS AND OBJECTIVES: The study aimed to develop proposals for an appropriate program for patients who had sustained mandibular condyle fractures.
DESIGN: Quantitative, non-experimental study, by means of a Delphi questionnaire.
METHODS: Data obtained from the literature and a previously conducted needs analysis was used in compiling a Delphi questionnaire dealing with the type and dosage of a suitable physiotherapeutic treatment protocol. The questionnaire was distributed amongst 20 experts (national and international) in the fields of physiotherapy, maxillo-facial surgery and dental surgery. A convenience sampling method was used to select appropriately trained participants for the Delphi review pane.l
RESULTS: The Delphi technique was used in the development of a suitable physiotherapy intervention program for mandibular condyle fracture patients. Inter-reviewer consensus was reached regarding the commencement and dosage of various jaw exercises, as well as what would constitute in-hospital physiotherapy visits.
CONCLUSIONS: The proposed post-surgical intervention program could serve as a baseline for clinical implementation and in further research studies. The advantages of referring these patients to physiotherapy are also highlighted.
Keywords: mandibular condyle fractures; physiotherapy for mandibular condyle fracture rehabilitation for mandibular condyle fractures; temporomandibular joint; trismus
INTRODUCTION
Trauma is regarded as one of the major factors resulting in temporomandibular joint (TMJ) dysfunction, especially as the articulating disc in the joint does not have the ability to repair and remodel.1,2 Following trauma to the mandibular condyles there may be a limitation of mandibular movement to a varying extent due to muscle spasm, oedema and haemarthroses.3 Safe and effective post-surgical exercises according to patient-specific precautionary measures can prevent displacement of fractured bone ends, stimulate remodelling, and have a positive effect on the recovery of normal mandibular function.4,5
A large number of studies have found that an ideal prognosis for mouth function is dependent on a programme of appropriate post-surgical functional exercises.5-9 Active and passive joint movements for increasing the range of motion of the TMJ are regarded as key components in the post-surgical management of patients who underwent surgery in the TMJ region. Long-term follow-up is recommended.10
No standardised criteria or post-operative rehabilitation programmes for patients who have sustained mandibular condyle fractures could be found in the literature.5,11,12 Previous research studies investigating the effects of any such exercise regimes varied in dosage and exercise types, and were all provided by surgeons with no physiotherapy demonstrations or interventions.5,8,13 Only one non-clinical study conducted by Trott (2011) described an empirically based physiotherapy intervention programme. In contrast, a South African research study specifically highlighted the need for physiotherapy intervention in the treatment of mandibular condyle fractures.8 Patients are afraid to exercise into a zone of discomfort for fear of re-fracturing or pain, therefore appropriate active jaw exercises should be commenced as soon as possible.9,14 It was the opinion of the participants in a previously conducted needs analysis that there is a need for physiotherapy intervention for patients who had sustained mandibular condyle fractures treated by ORIF surgery or closed reduction.15 The aim of this study was therefore to use the Delphi technique to compile a proposed physiotherapeutic intervention program for the post-operative rehabilitation of patients following mandibular condyle fractures.
METHODS
Study design
A quantitative, non-experimental Delphi technique study was performed.
Participants
As this study explored a formerly pristine area of physiotherapy research, a convenience sampling method was used to select appropriately trained reviewers for the Delphi review panel. Hence, the panel comprised of experts in the maxillo-facial, dentistry and physiotherapy fields in South Africa and abroad, with a ratio of 2:1 South African: International reviewers. More South African experts were recruited as the study aimed at promoting awareness of a new physiotherapy field in South Africa, and therefore focused on the South African environment and patients.
Specialist Maxillo-facial surgeons were included as were qualified physiotherapists who had completed their post-graduate training in Orthopaedic Manipulative Physiotherapy (OMPT), had a special interest in the cranio-mandibular field and / or a minimum of two years work experience in the field. The qualified dentists included in the Delphi review panel had to have a minimum of five years work experience in dental surgery.
The finally constituted Delphi round one review panel consisted of eight physiotherapists, eight maxillo-facial surgeons and four dental surgeons, in a ratio of 2:1:2, to provide for sufficient feedback from all experts routinely treating patients who had sustained mandibular condyle fractures. A larger number of maxillo-facial surgeons and physiotherapists were recruited, as they form the most important part of this rehabilitation team. Twenty review panel members were appointed to generate sufficient input and to provide for reviewer drop-out, while maintaining reliability.16-19
Ethical considerations
The study was approved by the Health Research Ethics Committee of the University of the Free State (ECUFS NR: 05/2012). Informed consent was obtained from each participant before completion of the Delphi questionnaire. Confidentiality of all collected information was ensured as the questionnaire did not require names of the participants or any other identifiable data.
Procedure
Available international literature as well as the results of a previously conducted South African based needs analysis indicated that there is a need for physiotherapy intervention for patients who had sustained mandibular condyle fractures which had been treated by either open reduction or internal fixation (ORIF) surgery or closed reduction.
The Delphi method is based on reviewers reaching a pre-determined level of consensus in the responses to questions. This is achieved by a process of repeated circulation of a questionnaire to an anonymous panel of experts, the questions being modified by feedback for each round.20
The questions on the Delphi questionnaire were formulated using information gained from personal communication with maxillo-facial surgeons, from available literature and from the results of the needs analysis.15 Information gained from that analysis included recommended pre-cautionary measures as well as exercises for possible inclusion in a post-operative exercise regime for mandibular condyle fracture patients.
The questionnaire was divided into two sections: demographical information and the proposed physiotherapeutic management of mandibular condyle fracture patients. Closed questions were posed to participants, with areas for comment following each question.
A pilot study was conducted to increase the face validity of the study and to minimise misinterpretation of questions. Piloting of each Delphi questionnaire round was done by two experts in the field, one physiotherapist and one maxillo-facial surgeon. SurveyMonkey™, an online research tool, was used to electronically send each questionnaire round to members of the review panel.
Consensus for this study was determined as an 80% agreement between participants regarding a question's answer. If consensus was reached, the question was omitted from subsequent rounds. Questions not achieving consensus were identified and information was extracted from questionnaire responses and fed back to the reviewers for consideration and further deliberation during the subsequent round. Any relevant comments or questions logged by reviewers during a round, were also incorporated into the subsequent questionnaire for circulation. The stability of responses for the questions not reaching consensus, was measured when there were no new comments from reviewers indicating that a saturation point had been reached.21
A review panel member was excluded from subsequent Delphi questionnaire rounds if he / she failed to respond within the allocated time frame for completion of the questionnaire round.
Statistical analysis
SurveyMonkey™, the online research tool used to conduct this study, reported all results as a percentage. The data obtained from the three Delphi questionnaire rounds was analysed by the researcher, in conjunction with the research supervisors who were responsible for verifying data analyses.
RESULTS
Demographics and response rate
Of the 20 review panel members included in round one of the questionnaire, 12 completed the third and final questionnaire round, of whom seven were physiotherapists and three, maxillo-facial surgeons. The main reason cited for surgeon drop-out was a lack of time to complete the subsequent questionnaire rounds.
The gender distribution was equitable during all three rounds of the Delphi questionnaire. The majority of reviewers were practising in the private sector.
The ratio of South African versus international members of the review panel was 2:1 during the final questionnaire round, however that ideal was not met for physiotherapists due to international reviewer drop out.
Possible physiotherapy intervention for mandibular condyle fracture patients
Currently the majority of in-hospital patients treated for mandibular condyle fractures are seen only by maxillo-facial surgeons. Two physiotherapists and one dentist indicated that they are involved in the treatment and rehabilitation of mandibular condyle fracture patients in an out-patient setting. One international reviewer indicated that mandibular condyle fracture patients abroad are already receiving routine physiotherapeutic management.
The majority of review panel members were of the opionion that a physiotherapist should evaluate mandibular condyle fracture patients who had been treated by either ORIF surgery or closed reduction, as well as manage and progress the post-surgery exercise program. Stability amongst reviewers was reached regarding physiotherapy evaluation and treatment commencing day one after either ORIF surgery or closed reduction. The panel tended toward agreement, and stability was reached, regarding whether mandibular condyle fracture patients should receive physiotherapy treatment until hospital discharge.
Forty-two percent of review panel members reported that 11-49% of mandibular condyle fracture patients, treated by closed reduction tend to demonstrate in-hospital functional loss. More than 70% of review panel members reported that up to 0-49% of mandibular condyle fracture patients treated by ORIF surgery, and between 11-49% of patients treated by closed reduction, reported functional loss at follow-up.
Results regarding pre-cautionary measures to be considered when treating mandibular condyle fracture patients varied between rounds. However, it was found that at six weeks postoperatively there was a relatively consistent high response rate regarding adherence to pre-cautionary measures for mandibular condyle fracture patients, who had been treated by either treatment method. Although stability was reached indicating the safety of posterior-anterior / anterior-posterior mandibular condyle movements, it is the opinion of reviewers that the treating maxillo-facial surgeon should be contacted before commencing mandibular protrusion movements following a mandibular condyle fracture.
As shown in Table 1, stability was reached with reviewers indicating that jaw muscle stretches and passive TMJ movements should only be commenced during out-patient follow-up, whereas all other physiotherapeutic interventions can be commenced in-hospital.
There was an increased tendency in reviewer responses towards agreement that all exercises should be executed in front of a mirror, with stability reached in the recommendation that all jaw exercises should be done with light guided hand pressure to prevent incorrect mandibular deviation.
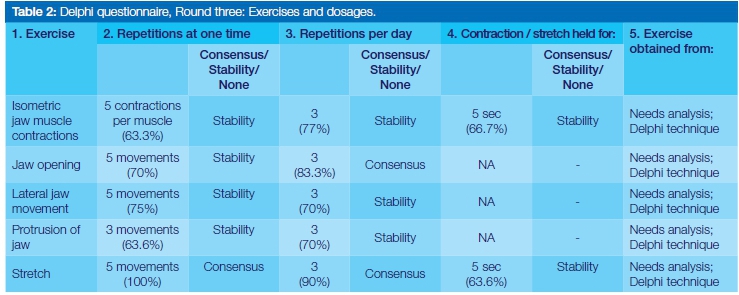
In accord with reviewer comments, questions relating to exercise dosage were simplified and grouped together. The exercise related questions were also, as per reviewer comments, grouped to be either answered by the maxillo-facial surgeons and dentists or physiotherapists, separately. As mentioned by reviewers, physiotherapists should have more experience with exercise prescription, and hence directing these questions to those panellists should ensure more reliable interpretations on the enquiry.
Data analyses indicated that the majority of exercise dosage related questions reached consensus between physiotherapists, with the maxillo-facial surgeons and dentists achieving consensus on only 50% of those questions, possibly due to their lack of practical experience in prescribing exercises. Physiotherapists achieved consensus on nearly 70% of exercise dosage questions, with the remaining 30% of questions recording between 70% and 76% inter-reviewer agreement (Table 2).
DISCUSSION
As facial trauma is one of the major causes of TMJ cartilage degeneration and intra-articular pathology, it is necessary to recognise that impact and to provide adequate treatment for this patient population.12 The study aimed to determine the proposed content of a post-operative physiotherapeutic intervention program for patients who had sustained mandibular condyle fractures, using the Delphi technique. The study results confirmed, according to expert opinion, that post-operative physiotherapeutic intervention for patients who had sustained mandibular condyle fractures is of the utmost importance.
Previous research studies investigating the effects of post-mandibular fracture exercise regimes varied in quality, dosage, exercise types and were all provided by surgeons with no physiotherapy demonstrations or interventions.5,8,13
As discussed in the studies conducted by Bevilaqua-Grosso et al (2002), Yun and Kim (2005) and Feng et al (2009) there are currently no unifying criteria regarding the physiotherapeutic management of mandibular condyle fractures.5,11,12 However, the need for adequate and prompt physiotherapy treatment in mandibular condyle fracture patients has been emphasised by a South African study conducted by Rikhotso and Ferretti (2008), and highlighted again in this Delphi study.8
The fact that stability was reached regarding only those questions relating to functional loss and the amount of treatment sessions provided, may be due to the fact that each patient presents differently after surgery, require different methods of treatment or may present with other complications resulting from their injury. Clear communication between the surgeon and physiotherapist is therefore important to ascertain fracture stability, the treatment required and those pre-cautionary measures for adherence.
As each patient differs clinically, it is advised that patient-specific pre-cautionary measures and their duration be discussed with the treating maxillo-facial surgeon.
Even though it was those questions pertaining to exercise dosages which achieved stability, the results regarding exercises which should be included in a post-operative physiotherapeutic intervention provided substantial information, enabling the compilation of a comprehensive exercise program, together with proposed exercise dosages. The exercise dosages suggested by the Delphi review panel showed concurrence when compared with the general exercise prescription guidelines proposed in the literature. Thse advocate a low number of repetitions, performed at low intensity, to be repeated several times per day.22
When analysing the results, it should be taken into account that only 50% of review panel members had clinical experience in the physiotherapeutic treatment of patients who had sustained mandibular condyle fractures. As this regime is still a fairly unexplored area in South Africa, this lack of experience is to be expected.
The results of the Delphi study was used to compile and to propose a post-operative intervention protocol for mandibular condyle fracture patients which could be implemented in clinical trials as part of further research to assess the viability and efficacy of the programme.
CONCLUSION
The need for adequate and prompt physiotherapy treatment for mandibular condyle fracture patients has been emphasised by the previously conducted needs analysis, as well as previous research.5-9,15 The results of the study provide a platform for expanding the evidence-base for physiotherapy intervention for the treatment of maxillo-facial conditions. Whilst an evidence-based method was utilised during the development of the proposed post-operative physiotherapy intervention program, this in no way guarantees efficacy in the prevention of complications in patients who underwent maxillo-facial surgery following a mandibular condyle fracture. Further research is warranted into the implementation of this proposed physiotherapeutic intervention to determine the efficacy of the programme.
LIMITATIONS
As the study investigated an area where in which very few South African physiotherapists are currently actively practicing, reviewers showed a certain amount of hesitation to participate in due to a lack of specific clinical knowledge. This reluctance resulted in difficulties in increasing the original sample size.
There is a strong possibility that recall bias may have been present in the questions relating to patient-reported functional loss in-hospital and at follow-up after ORIF surgery or closed reduction for mandibular condyle fractures.
As the majority of respondents were physiotherapists, bias could have been present, in that there would a natural tendency for physiotherapists to believe that physiotherapy is invaluable in the treatment of mandibular condyle fracture patients.
Inter-reviewer consensus could not be reached on all questions posed to reviewers, possibly due to the differing nature of the specialisation fields of the participants. This dilemma was addressed by separating out those questions pertaining to exercise prescription.
Acknowledgements
The researcher would like to extend a heartfelt thank-you to all reviewers who participated in the study, for offering their precious time and valuable input.
ACRONYMS
OMPT: Orthopaedic Manipulative Physiotherapy
ORIF: open reduction and internal fixation
TMJ: temporomandibular joint
References
1. Levangie PK, Norkin CC. Joint Structure and Function: A Comprehensive Analysis. 3rd ed. Philadelphia: F. A. Davis Company, 2002: 186-92. [ Links ]
2. Görgü M, Deren O, Sakman B, Ciliz D, Erdoğan B.. Prospective comparative study of the range of movement of temporomandibular joints after mandibular fractures: rigid or non-rigid fixation. Scand J Plast Recons. 2002;36(6):356-61. [ Links ]
3. Zachariades N, Mezitis M, Mourouzis C, Papadakis D, Spanou A. Fractures of the mandibular condyle: a review of 466 cases. Literature review, reflections on treatment proposals. J. Cranio-Maxillofac. Surg .2006;34:421-32. [ Links ]
4. Tanaka E, Koolstra JH. Biomechanics of the temporomandibular joint. J Dent Res. 2008;87(11):989- 91. [ Links ]
5. Feng Z, Chen R, Zhang Y, Yang M, Lin Y, Tian W, Liu L. Outcome of postsurgical sequential functional exercise of jaw fracture. J Craniofac Surg. 2009;20:46-8. [ Links ]
6. Thiele RB, Marcoot RM. Functional therapy for fractures of the condyloid process in adults. J Maxillofac Surg. 1985;43:226-8. [ Links ]
7. Hwang K, Park JH, Lee, HJ. Miniplate fixation of high condylar fracture and postoperative exercise regimen. J Craniofac Surg. 2005;16(1):113-6. [ Links ]
8. Rikhotso E, Ferretti C. A prospective audit over a six month period of condylar fractures at Chris Hani Baragwanath Hospital. SADA 2008;63(4): 222-5;228-9. [ Links ]
9. Trott PH. The management of TMJ patients: Part 1. Available from: 2011.http://www.clinicalsolutions.co.za. [ Links ][Accessed on 7 September 2011].
10. McCarty WL Jr, Darnell MW. Rehabilitation of the temporomandibular joint through the application of motion. Cranio. 1993;11(4):298-307. [ Links ]
11. Bevilaqua-Grosso D, Monteiro-Pedro V, De Jesus Guirro RR, Bérzin F. A physiotherapeutic approach to craniomandibular disorders: a case report.J Oral Rehabil. 2002;29:268-73. [ Links ]
12. Yun PY, Kim YK. The role of facial trauma as a possible etiologic factor in temporomandibular joint disorder. J Oral Maxillofac Surg. 2005;63:1576-83. [ Links ]
13. Hwang K, Han JY, Kil MS, Lee S. Treatment of condyle fracture caused by mandibular angle osteotomy. J Craniofac Surg. 2002;13(5):709-12. [ Links ]
14. Brukner P, Khan K. Clinical Sports Medicine, Revised 2nd ed. Australia: McGraw-Hill, 2002;128:145-72,214. [ Links ]
15. Van der Merwe A, Barnes, RY. The need for physiotherapy intervention for mandibular condyle fracture patients: A needs analysis. 2015. SADJ 2015;70(5):196-9. [ Links ]
16. Dorey G. Physiotherapy for the relief of male lower urinary tract symptoms: A Delphi study. Physiotherapy. 2000;86(8):413-26. [ Links ]
17. Barker K, Burns M. Using consensus techniques to produce clinical guidelines for patients treated with the Ilizarov fixator. Physiotherapy. 2001;87(6):289-300. [ Links ]
18. Opie J, Taylor MC. An exploratory Delphi study on the integration of disabled students into physiotherapy education. Physiotherapy. 2008;94(4):292-9. [ Links ]
19. Carnes D, Mullinger B, Underwood M. Defining adverse events in manual therapies: A modified Delphi consensus study. Manual Therapy. 2010;15(11):2-6. [ Links ]
20. Skulmoski GJ, Hartman FT, Krahn J. The Delphi Method for graduate research. JITE-Research. 2007;6:1-21. [ Links ]
21. Hsu C, Sandford BA. The Delphi Technique: Making sense of consensus. Practical Assessment. Research and Evaluation. 2007;12(10):1-8. [ Links ]
22. Kisner C, Colby, LA. Therapeutic Exercise: Foundations and Techniques. 5th ed. Philadelphia: F. A. Davis Company, 2007;163-9. [ Links ]
 Correspondence:
Correspondence:
Anke van der Merwe
Department of Physiotherapy, University of the Free State
Christiaan de Wet Building, Rektor Avenue, Bloemfontein, 9301.
Tel: 27 51 401 3289. Cell: 27 82 446 4923.
E-mail address: gonzalesa@ufs.ac.za

{kind=link}
{kind=link}