










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.71 no.4 Johannesburg Mai. 2016
RADIOLOGY CASE
Maxillo-facial radiology case 140
CJ Nortjé
BChD, PhD, ABOMR, DSc. Faculty of Dentistry, University of the Western Cape. E-mail: cnortje@uwc.ac.za
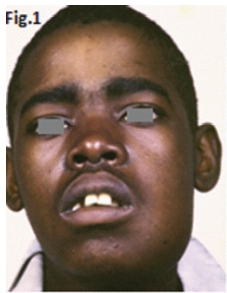
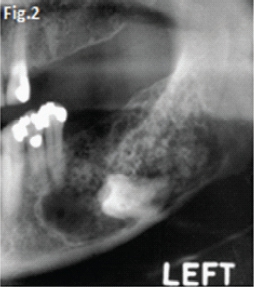
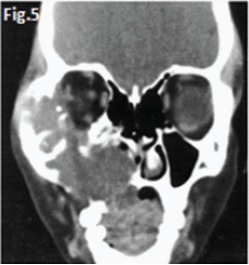
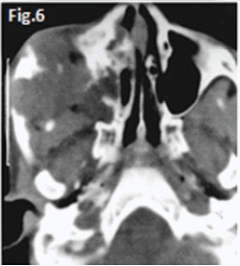
This 22 year old male patient (Figs.1 & 2) presented with a slow growing swelling in the left mandibular molar region. Figures 3, 4, 5 & 6 are images of three other patients with the same condition. Discuss the radiological features and what is your diagnosis?
INTERPRETATION
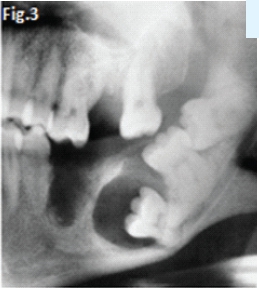
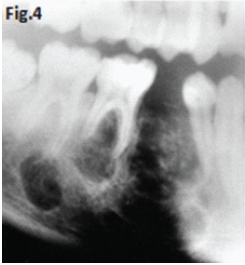
Fig 1 & 2: the large lesion of left mandible shows a honeycomb-like distribution of calcifications. The borders are corticated. The tumour has displaced the mandibular molar tooth. A histological diagnosis of calcifying epithelial odontogenic tumour (Pindborg Tumour) was made. Fig.3 shows a Pindborg tumour distal to left second premolar associated with displacement of the first molar tooth. Fig.4 shows a similar tumour with mixed lucency-opacity between right premolar and molar teeth. Figs 5 & 6 show coronal and axial CT views of a large Pindborg tumour affecting the right maxilla. Note the marked expansion and cortical destruction. Calcifying epithelial odontogenic tumour is a rare benign neoplasm, accounting for less than 1% of all odontogenic tumours. The average age at diagnosis is 40 years; however, the tumour can occur at any age. It occurs equally in males and females. Approximately two thirds of cases are reported to occur in the mandible. Most cases occur in the premolar-molar area and are commonly associated with an unerupted tooth. The tumour is a painless, slowly enlarging mass. Histologically the tumour has a very characteristic appearance. Sheets of polyhedral cells with well-defined eosinophilic cytoplasm and hyperchromatic nuclei are featured. Amyloid and ringlike calcification may also be present. The tumour may be irregular or, in some cases, the cystic lesions may be well defined and corticated, whereas others appear ill defined. Small unilocular lesions may have a completely radiolucent centre (Fig.3). Others may have variable amounts of small flecks of calcifications scattered throughout. Larger lesions have a multilocular or honeycomb appearance. The tumour can displace and often prevent the eruption of teeth. Radiologically the tumour may be very similar to the calcifying odontogenic cyst, adenomatoid odontogenic tumour and ameloblastic fibro-odontoma.
Reference
1.Farman AG, Nortje CJ & Wood R E: Oral and Maxillofacial Imaging, 1st Ed, Mosby. St. Louis, Missouri 1993 pp. 244-246. [ Links ]
