










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.71 no.4 Johannesburg Mai. 2016
RESEARCH
An audit of root canal treatments completed by students and dentists at an academic hospital
Vanessa C MostertI; Casper H JonkerII
IBChD, PG Dip Dent (Practice Management), MSc (Dent). Department of Dental Management Sciences, School of Dentistry, Faculty of Health Sciences, University of Pretoria, South Africa
IIBChD, PG Dip Dent (Odont), MSc (Endodontology). Division of Endodontics, Department of Operative Dentistry, School of Oral Health Sciences, Sefako Makgatho Health Sciences University, South Africa
INTRODUCTION
The University of Pretoria Oral Health Centre (UPOHC) houses the School of Dentistry where dental, oral hygiene and post graduate students are trained. Dentists employed at the School of Dentistry generally do not complete root canal treatments (RCTs) due to their academic and research commitments but mainly perform emergency dental procedures such as pulpectomies for the relief of acute pain. The pulpectomy procedure includes the extirpation of the necrotic or inflamed pulp, minimal shaping of the canal and irrigating with sodium hypochlorite. This is followed by placing a medicament with an anti-inflammatory action such as Ledermix® or calcium hydroxide and sealing the tooth with a temporary restoration. The patient is then placed on a waiting list (approximately 18 months) for completion of the RCT by students in their fourth and fifth year of study. Dentists complete RCTs mainly in cases where previous attempts made to locate the canals were not successful or where files have fractured in the canals or when retreatment is indicated.
The students complete a limited number of RCTs due to the time-consuming nature of the procedure and their relative lack of skill and experience.1 During the fourth year of study the students are required to complete five RCTs on teeth with one and two canals. The clinical quota for the students in the fifth year of study is five RCTs on teeth that have three or four canals.2
Several studies3-7 have been conducted on the acceptability of root canal obturations with regard to the technical quality as viewed on post-operative radiographs. The studies in question reported an acceptable technical quality of 47.4%, 84.1%, 61.35%, 57% and 44% respectively.3-7 In four of these, the RCTs assessed were completed by undergraduate students. Root fillings between 0.5mm to 2mm from the radiographic apex, consistent density and uniform taper were the criteria used to categorize the RCT as acceptable. Peak et al. also included the absence of apical pathology in the criteria.6
To date no research has been conducted on the technical quality of root canal fillings at tertiary institutions in South Africa.
METHODS
Study design
The design was an observational retrospective record based study.
A random sample of 500 from amongst 1050 teeth that had received an emergency pulpectomy between 1 July 2012 and 30 June 2013 was selected. A total of 224 of these 500 teeth had reached the obturation phase of the RCT by 30 June 2014. The maximum period before root canals were completed was thus 24 months. Four of the cases had no post-operative radiographs, although it was recorded on the file that radiographs had been taken. The clinician had failed to successfully capture the digital x-ray image on the Kodak software program. A sample size of 220 therefore remained.
The electronic and paper records of the 220 teeth on which a RCT had been completed by either a dentist or student were analysed at the UPOHC.
Technical quality assessment
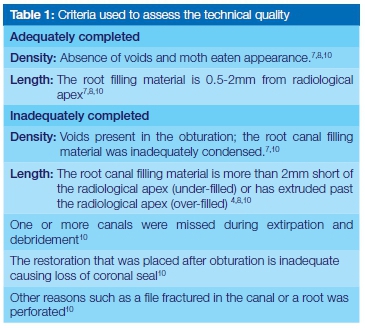
The post-operative intraoral periapical radiographs were accessed on the Kodak software programme (version 6.12). In the cases where the RCT had reached the obturation phase, a decision was made as to whether the RCT was completed adequately or inadequately, based on technical quality as viewed on the post-operative radiographs. The investigator who examined the radiographs is a full-time dentist with 14 years' experience as a clinician. He had supervised dental students at the UPOHC during endodontic clinical sessions for six years and had obtained a Diploma in Endodontology and a Master's degree in Radiology. Where examination of the radiograph resulted in a categorisation of the RCT as inadequate, the reasons for that assessment were recorded. The criteria used were those proposed by Román-Richon et al.7 and others.4, 8-11 These are displayed in Table 1.
Ethical considerations
All necessary ethical approval to access patient files and digital radiographic material was obtained from the relevant authority at the University of Pretoria, Faculty of Heath Sciences. Complete anonymity of the sample was ensured.
RESULTS
The results of the treatment outcomes as obtained from the patient files and digital records are displayed in Table 2.
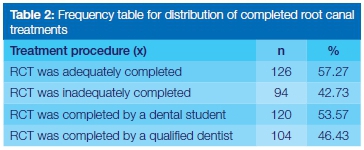
A total of 126 (57.27%) root fillings were adequate and 94 (42.73%) were deemed as inadequate.
In addition, a differentiation was made between RCTs completed by dentists and those completed by students. The calculation of data showed that the fourth and fifth year dental students completed 120 (54%) of the 224 RCTs and the qualified dentists completed 104 (46%) RCTs (Table 2).
Table 3, below, displays the result of the technical quality of the obturation differentiating between clinical provider type (student or dentist).
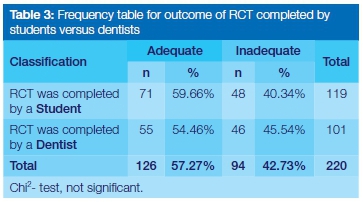
The data showed (Table 3) that the dental students completed 59.66% of their RCTs adequately and 40.34% inadequately. The dentists, on the other hand, completed 54.46% adequately and 45.54% inadequately. These differences were not statistically significant (Chi2- test).
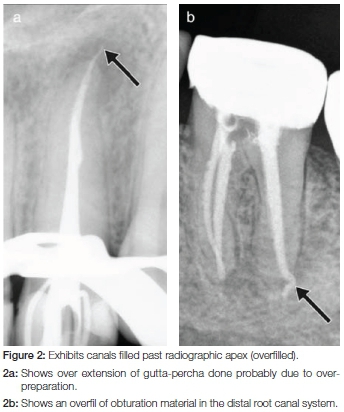
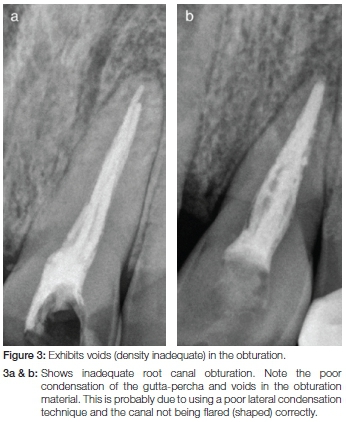
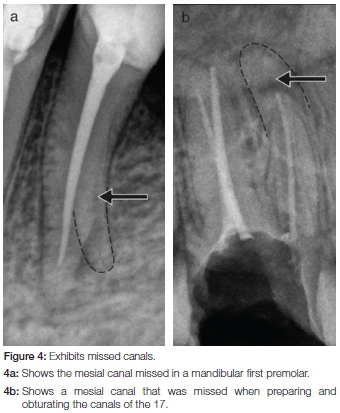
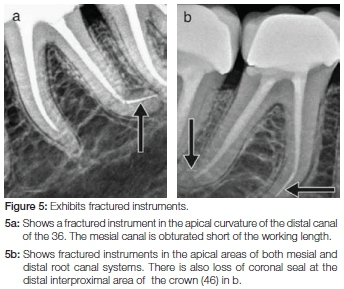
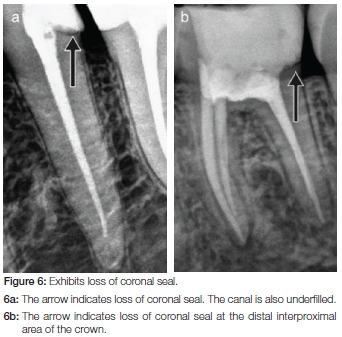
The RCTs that were inadequately completed by either qualified dentists or dental students were classified according to the evaluation of the postoperative radiographs (Table 4). The percentage could not be calculated as some teeth had two or more reasons for inadequacy. The obturated root canals of 57 teeth were under-filled and 11 over-filled. Sixteen teeth had voids in the obturation and in 11 teeth a missed canal was detected. An endodontic instrument was fractured off in five of the obturated teeth and five teeth lacked a proper coronal seal after the obturation. Radiographs revealed that in two teeth the root had been perforated. Figures 1-7 illustrates some digital radiographic examples, of the underfilled and overfilled canals (Figures 1 and 2 respectively), voids in the obturation (Figure 3), missed canals (Figure 4), fractured files (Figure 5), loss of coronal seal (Figure 6) and a root perforation (Figure 7).



DISCUSSION
Most root canal treatment failures develop when initial treatment procedures, mainly technical in nature, have not succeeded to thoroughly eliminate pathogenic factors. Dammaschke et al. concluded that root canal therapy can be a durable way of preserving teeth even when the RCT is carried out by students.13
Assessment of the technical quality of the RCT's in this study showed that 57.27% of completed cases were of acceptable quality (using the criteria described in Table 1). This percentage appears to be lower than those found in other studies which focused on the quality of the root canal fillings done by undergraduate students.4,14 In a study by Lynch et al. in 2006, 70% of the RCTs performed had acceptable root fillings using the same criteria as those used in this research.15 A similar study, conducted by Chakravarthy and Moorthy found that 61.35% of the RCT's completed by undergraduate students in the Department of Conservative Dentistry and Endodontics, Penang International Dental College, Malaysia were adequate.5 This rating is 4% higher than the results for acceptable technical quality achieved by dentists and students in the current study.
Rafeek et al. stated that no curriculum can remain stagnant and that quality control auditing is imperative for ongoing improvement.16 Chakravarthy & Moorthy deduced from their study that auditing the root canal fillings plays a crucial role in quality assurance in dental schools.5 The authors offer valuable insights such as the need for frequent auditing of the endodontic curriculum, to lengthen the time allocated to preclinical and clinical training, to raise the staff-student supervision ratio and to include student self-assessment activities. Similar observations were reported in another study by Hayes et al. where a mere 13% of RCTs were adequately obturated, judged using the same criteria used in the current study.17
This study reported that the poor results mirror the lack of experience of dental students at University of Wales College of Medicine as well as questioning the supervision and assessment methods. These opinions are confirmed by Lynch & Burke who state that teaching of undergraduate students should be conducted by specialist endodontists rather than by academic consultants who have an interest in endodontics.15,17 It is therefore recommended that dentists supervising the endodontic clinical student sessions at the UPOHC should preferably have postgraduate qualifications in the endodontic field of study.3,18 Seminars which increase skills and knowledge should be presented to supervisors who do not have postgraduate qualifications.8 This approach could contribute to the Continuing Professional Development (CPD) points required by the Health Professions Council of South Africa. Increasing the supervisor-student ratio for endodontic sessions should be considered as is also recommended in Chakravarthy and Moorthy's study.5
Endodontics is indeed a difficult skill19,20 and the clinician's competency is the predominant factor determining the success of the outcome of root canal treated teeth.20 Duvivier et al. emphasized the need for purposeful repetition of practical tasks in order to gain the necessary clinical skills. As part of the current curriculum at the UPOHC, the dental students in their third year of study practice RCT on extracted teeth in the laboratory. They are allowed to treat endodontic patients in their fourth year of study only once they have passed the preclinical practical exam. Although these students start at an early stage in their studies to identify the root canal system, more extensive training could be considered for incorporation into the curriculum. Scaffolding is an approach to enhance a student's self-governed learning skills.21 At every level of study the students should have adequate assistance in the initial phases of endodontic training and then be gradually weaned off instruction as they master the endodontic milestones independently.22 This means gradually reducing the support and progressively expanding the student's responsibility.22
In view of the findings of this study it is recommended that an increase in student clinical quotas for endodontics be considered at the UPOHC. Endodontics could be introduced more extensively at an early stage, in the preclinical third year of study. Practical application of modern technology such as the rotary instrumentation and the electronic determination of working lengths should be incorporated in this preclinical year.8,23 The technique for obturation of root canal treated teeth currently being taught to undergraduate dental students at the University of Pretoria is cold lateral condensation. Use is made of gutta-percha which Hammad et al. documented as showing the minimum amount of voids during root section.24 The final year students are however, additionally taught to use the ProTaper Universal (Dentsply Maillefer) system which consists of rotary nickel-titanium files. An earlier introduction of the use of rotary instruments (particularly the use of rotary instruments on extracted teeth in the laboratory) may improve the acceptable outcome of completed RCTs. However, use of rotary instruments in clinical wards must be preceded by thorough practice on extracted teeth.
Productive use of students' clinical time is another factor to be investigated. At the UPOHC, much time is spent by students preparing/disinfecting the surgery (cubicle) for their patients as well as on collecting materials needed for the clinical session. The output of these students could certainly be increased if they could be provided with dental assistants. Possible solutions may include the training of junior dental students to assist during clinical teaching and learning. Greater collaboration between tertiary institutions is necessary for dental assistant (dental nursing) students to be placed in the wards during the student clinical sessions so that productivity can be enhanced. If more qualified chair side assistants could be employed then these personnel could help the dental students to prepare their surgeries before and after treatments. Dental assistants could help ensure that infection control protocols are in place, gather and prepare dental materials to be used during the session, and process instruments once the treatment has been carried out. Such measures will not only increase the productivity of the students, but may even provide both the dental and dental assistant students with improved teamwork skills and competencies, which may have an additional educational benefit. A similar recommendation was made in the United Kingdom where the General Dental Council recommended that for all dental procedures students work with a dental nurse.25 Installation of additional periapical x-ray machines in the endodontic clinical wards could decrease the time students spend waiting to take radiographs. There are currently only two machines per group (varying between 10 and 20 students) during one endodontic clinical session. Another option is to utilize other wards with more periapical x-ray machines for endodontic sessions.
The results from Table 3 indicate that the outcomes of RCT's completed by qualified dentists and by undergraduate students differ by only five percent, whether judged adequate or inadequate. It may be expected that qualified dentists should have a higher success rate compared with students. However, the staff at the UPOHC, working under severe time constraints, do the retreatments and difficult cases students could not manage, which may challenge and influence the quality of the clinical work.26, 27 In a study at a German dental school, Stoll et al. attributed the 74% survival rate of endodontically treated teeth to the fact that at a training hospital the difficult root canal treatment cases are delegated to the dentists.28 Certain root canal failures such as broken file segments are sometimes impossible to reverse and as Souter & Messer suggested, should not be attempted routinely.18,29 A valuable insight by Hayes et al. stated that focus should be on the quality of treatment rather than quantity.17 Dentists at the UPOHC ideally should allocate more time to properly complete RCTs rather than perhaps aiming for quantity and compromising on quality. Proper selection of teeth for RCT, especially teeth that require retreatment, should be considered. A good coronal restoration can diminish the risk of failure of root canal treated teeth.30 The traditional method of restoring endodontically-treated teeth is the placement of full crown coverage. Nagasiri and Chitmongkolsuk investigated the survival of endodontically-treated teeth which had no coronal coverage.31 A mere 54% of teeth survived after 5 years, showing that a proper coronal restoration like a crown is essential for root canal treated teeth.31 However, according to latest research which is based on laboratory studies, root canal treated premolars and molars with limited destruction of hard tissue can be restored with composite without the use of posts.32 Post placement is beneficial however, when there is no cusp protection particularly left in premolars.32 Mannocci & Cowie stated that the conservation of tooth structure is crucial to the longevity of a root canal treated tooth.30 The preservation rather than removal of dentine is made possible with composite restorations using adhesive techniques rather than expanded mechanical retentions.30
Limitations
Two-dimensional radiographs (conventional digital intra oral) were used to assess the technical quality of the completed root treatment. Three-dimensional radiography (a CBCT scan/cone beam) may have yielded more precise assessments. A single clinician retrospectively examined the radiographs with no repeatability assessment. It is financially costly to perform a CBCT scan on every endodontic patient and the high radiation dosage produced with the CBCT imaging makes it unethical to perform routine scans.33
As with most retrospective studies, the quality of the data depended largely on the quality of the documentation of existing records34 including the legibility of handwriting on the hospital files. Sometimes students or dentists failed to record the entire treatment visit or omitted the tooth number on which the treatment procedure was carried out.
CONCLUSION
The assessment of 42.73% of a random sample of RCT's as inadequate raises a number of concerns.
1. Auditing of root canal fillings is an important contributing factor for this provides the basis of long term survival of teeth treated endodontically by undergraduate students.5 Members of staff involved in clinical supervision of endodontics should be equipped with sufficient knowledge and clinical experience to evaluate and sign off RCTs which display adequately filled canals to proper working length. Shortcomings in the proper evaluation of obturated RCTs will almost certainly result in failure of the treatment.
2. Th ere may be a need to:
2.1 Increase student-supervisor ratio;
2.2 Allocate more time to clinical and preclinical endodontic training in order to raise student clinical quotas
2.3 Re-organise the dental treatment facilities to enhance efficiency in endodontic clinical sessions;
2.4 Ensure dentists dedicate more time to complete the more difficult RCTs and properly select the cases that can be successfully treated by students.
2.5 Recall patients with unsatisfactory RCTs for retreatment by experienced dentists. This can be used as a teaching tool during student endodontic tutorials.
2.6. Properly plan clinical time during student endodontic sessions to allow sufficient time to complete lengthy procedures and avoid unnecessary mistakes due to a rushed effort.
3. This study was undertaken at a particular Dental School. It may be instructive to repeat the study at other Schools.
ACRONYMS
RCTs: root canal treatments
UPOHC: University of Pretoria Oral Health Centre
References
1. Bender I. Reversible and irreversible painful pulpitides: diagnosis and treatment. Australian Endodontic Journal. 2000;26:10-4. [ Links ]
2. University of Pretoria. Study Guide: Endodontic Module. [Study Guide]. In press 2014. [ Links ]
3. Barrieshi-Nusair K, Al-Omari M, Al-Hiyasat A. Radiographic technical quality of root canal treatment performed by dental students at the Dental Teaching Centre in Jordan. Journal of Dentistry. 2004;32:301-7. [ Links ]
4. Kelbauskas E, Andriukaitiene L, Nedzelskiene I. Quality of root canal filling performed by undergraduate students of odontology at Kaunas University of Medicine in Lithuania. Stomatologija. 2009;11:92-6. [ Links ]
5. Chakravarthy P, Moorthy J. Radiographic assessment of quality of root fillings performed by undergraduate students in a Malaysian Dental School. Saudi Endodontic Journal. 2013;3:77. [ Links ]
6. Peak J, Hayes S, Bryant S, Dummer P. Endodontics: The outcome of root canal treatment. A retrospective study within the armed forces (Royal Air Force). British Dental Journal. 2001;190:140-4. [ Links ]
7. Román-Richon S, Faus-Matoses V, Alegre-Domingo T, Faus-Llácer VJ. Radiographic technical quality of root canal treatment performed ex vivo by dental students at Valencia University Medical and Dental School, Spain. Medicina Oral, Patologia Oral y Cirugia Bucal. 2014;19:e93. [ Links ]
8. Khabbaz M, Protogerou E, Douka E. Radiographic quality of root fillings performed by undergraduate students. International Endodontic Journal. 2010;43:499-508. [ Links ]
9. Schaeffer MA, White RR, Walton RE. Determining the optimal obturation length: a meta-analysis of literature. Journal of Endodontics. 2005;31:271-4. [ Links ]
10. Walton RE, Torabinejad M. Endodontics : Principles and Practice. 4 ed. St. Louis, Mo.: Saunders/Elsevier; 2009. [ Links ]
11. Saunders W, Saunders E, Sadiq J, Cruickshank E. Technical standard of root canal treatment in an adult Scottish sub-population. British Dental Journal. 1997;182:382-6. [ Links ]
12. Nair P. Pathogenesis of apical periodontitis and the causes of endodontic failures. Critical Reviews in Oral Biology & Medicine. 2004;15:348-81. [ Links ]
13. Dammaschke T, Steven D, Kaup M, Ott KHR. Long-term survival of root-canal-treated teeth: A retrospective study over 10 years. Journal of Endodontics. 2003;29:638-43. [ Links ]
14. Yavari H, Samiei M, Shahi S, Borna Z, Abdollahi AA, Ghiasvand N, et al. Radiographic evaluation of root canal fillings accomplished by undergraduate dental students. Iranian Endodontic Journal. 2015;10:127. [ Links ]
15. Lynch C, Burke F. Quality of root canal fillings performed by undergraduate dental students on single rooted teeth*. European Journal of Dental Education. 2006;10:67-72. [ Links ]
16. Rafeek RN, Marchan SM, Naidu RS, Carrotte PV. Perceived competency at graduation among dental alumni of the University of the West Indies. Journal of Dental Education. 2004;68:81-8. [ Links ]
17. Hayes S, Gibson M, Hammond M, Bryant S, Dummer P. An audit of root canal treatment performed by undergraduate students. International Endodontic Journal. 2001;34:501-5. [ Links ]
18. Ruddle CJ. Nonsurgical retreatment. Journal of Endodontics. 2004;30:827-45. [ Links ]
19. Ashkenaz P. One-visit endodontics. Dental Clinics of North America. 1984;28:853-63. [ Links ]
20. Duvivier RJ, van Dalen J, Muijtjens AM, Moulaert VR, van der Vleuten CP, Scherpbier AJ. The role of deliberate practice in the acquisition of clinical skills. BMC Medical Education. 2011;11:101. [ Links ]
21. Kicken W, Brand-Gruwel S, van Merriënboer JJ. Scaffolding advice on task selection: A safe path toward self directed learning in on demand education. Journal of Vocational Education and Training. 2008;60:223-39. [ Links ]
22. Larkin MJ. Providing support for student independence through scaffolded instruction. Teaching Exceptional Children. 2001;34:30-4. [ Links ]
23. Dummer P. Comparison of undergraduate endodontic teaching programmes in the United Kingdom and in some dental schools in Europe and the United States. International Endodontic Journal. 1991;24:169-77. [ Links ]
24. Hammad M, Qualtrough A, Silikas N. Evaluation of root canal obturation: a three-dimensional in vitro study. Journal of Endodontics. 2009;35:541-4. [ Links ]
25. Stewardson D, Palenik C, McHugh E, Burke F. Occupational exposures occurring in students in a UK dental school1. European Journal of Dental Education. 2002;6:104-13. [ Links ]
26. Carrotte P. Endodontics: part 8 Filling the root canal system. British Dental Journal. 2004;197:667-72. [ Links ]
27. Elemam RF, Pretty I. Comparison of the success rate of endodontic treatment and implant treatment. International Scholarly Research Network Dentistry. 2011. [ Links ]
28. Stoll R, Betke K, Stachniss V. The influence of different factors on the survival of root canal fillings: a 10-year retrospective study. Journal of Endodontics. 2005;31:783-90. [ Links ]
29. Souter NJ, Messer HH. Complications associated with fractured file removal using an ultrasonic technique. Journal of Endodontics. 2005;31:450-2. [ Links ]
30. Mannocci F, Cowie J. Restoration of endodontically treated teeth. British Dental Journal. 2014;216:341-6. [ Links ]
31. Nagasiri R, Chitmongkolsuk S. Long-term survival of endodontically treated molars without crown coverage: a retrospective cohort study. The Journal of Prosthetic Dentistry. 2005;93:164-70. [ Links ]
32. Aurèlio IL, Fraga S, Rippe MP, Valandro LF. Are posts necessary for the restoration of root filled teeth with limited tissue loss? A structured review of laboratory and clinical studies. International Endodontic Journal. 2015:Sept. doi.10.1111/iej 12538 . [ Links ]
33.Low KM, Dula K, Bürgin W, von Arx T. Comparison of periapical radiography and limited cone-beam tomography in posterior maxillary teeth referred for apical surgery. Journal of Endodontics. 2008;34:557-62. [ Links ]
34. Caplan DJ, White BA. Clinical factors related to non-completion of root canal therapy. Journal of Public Health Dentistry. 2001;61:6-13. [ Links ]
 Correspondence:
Correspondence:
Vanessa C Mostert
Department of Dental Management Sciences
School of Dentistry, University of Pretoria
P.O. Box 1266, Pretoria, 0001, South Africa
Tel: +27 12 319 2370
Cell: +27 84 654 2322
Fax: +27 12 319 2146
E-mail: vanessa.mostert@up.ac.za
