










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.71 n.3 Johannesburg Apr. 2016
CASE REPORT
Adolescent caries management: An interdisciplinary approach
K PradeepI; S KariappaII; KC ChethanaIII; MA KuttappaIV
IAssociate Professor, Department of Conservative Dentistry & Endodontics, Manipal College of Dental Sciences, Manipal, Karnataka, India
IISenior Lecturer, Department of Conservative Dentistry & Endodontics, Coorg institute of Dental Sciences, Virajpet, Coorg. Karnataka, India
IIIReader, Department of Periodontics, Shravathi Dental College and Hospital, Shimoga,Karnataka, India
IVFormer Professor and Head, Department of Conservative Dentistry & Endodontics,Coorg Institute of Dental Sciences, Virajpet, Coorg. Karnataka, India
ABSTRACT
Adolescent caries is a new and growing challenge in restorative dentistry. Dental aesthetics has become a popular topic in all the disciplines in dentistry. When a makeover is planned to enhance the aesthetic appearance of the teeth of a patient, the clinician must have a logical diagnostic approach that results in the appropriate treatment plan. With some patients, the restorative dentist cannot accomplish the correction alone, but may require the assistance of colleagues in other dental disciplines. This case describes a unique approach to interdisciplinary dental diagnosis, beginning with aesthetics but encompassing structure, function and biology to achieve an optimal result. Providing education about risk factors for dental caries, such as consumption of sugars and poor oral hygiene, together with the introduction of preventive strategies, not only assists in meeting the special oral needs of the adolescent population, but also helps in the establishment of lifelong healthy habits.
Key words: Adolescent caries, interdisciplinary approach, interdisciplinary management
INTRODUCTION
Globally the prevalence of dental caries in permanent teeth is approximately 50% in 12- to 15-year-olds and 78% in 17-year-olds.1 Adolescence marks a period of significant caries activity for many individuals. Current research suggests that the overall caries rate is declining, yet remains highest during adolescence.2 The same factors that influence caries risk in children still exist throughout ado-lescence.3 Health care providers should be mindful of the following risk factors for caries: a) Inadequate access to fluoride b) Poor oral hygiene c) Frequent access to sugars d) Previous caries experience e) Reduced salivary flow f) Infrequent professional dental care.3
Changes in the frequency, distribution, and rate of progression of dental caries demand a re-evaluation of the treatment paradigm. Treatment of the adolescent patient can be multifaceted and complex.4 This case report explains the successful management of adolescent caries in a 17 year old patient, based on an interdisciplinary approach. Coordinated endodontic, periodontal and pros-thodontic treatments, with careful consideration of patient expectations, requests and financial status, were critical for a successful outcome and patient satisfaction.
CASE REPORT
A 17 year old male patient reported to the Department of Conservative Dentistry and Endodontics with the main complaint of decayed teeth. On intra-oral examination, deep carious lesions were seen in the maxillary anterior, premolars, first molar and mandibular first molar teeth (Figure 1a and b). In addition, a gingival polyp in relation to 24, 26 and a pulp polyp in relation to 46 were observed (Figure 3 a and b). No other significant changes were seen in soft tissue. The patient's medical history was non-contributory.



The patient had the habit of frequent intake of chocolates (sucrose) and of taking milk and biscuits just before going to sleep. He used to brush once a day in the morning and practised no other form of oral hygiene measures. Orthopantomograph examination revealed carious lesions involving the pulp in relation to 16, 24, 46 and carious lesions approaching the pulp with respect to 15, 12, 11, 21, 23, 26 and 36 (Figure 2). Vitality tests (electric and thermal tests) gave a negative response in relation to all above-mentioned teeth.
The clinical and special investigation findings were collated and, following discussion with other specialties (Periodontics and Prosthodontics), the following treatment was planned:
- Oral prophylaxis
- Excision of gingival and pulp polyps.
- Root canal therapy
- Crown lengthening procedure
- Post Endodontics restorations
The treatment procedures were explained to the patient and informed consent was obtained. Oral prophylaxis followed by excision of gingival and pulp polyps was carried out in Department of Periodontics. Multiple visit root canal treatment was carried out, per quadrant under rubber dam isolation. Calcium hydroxide was used as an intra-canal medicament (Figure 4).The access cavities were restored with composite resins.

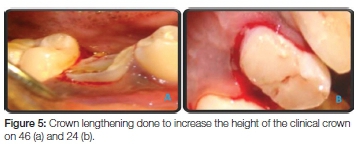
Crown lengthening is a surgical procedure which removes periodontal tissue to increase the clinical crown height and re-establish the biological width. In this case, the procedure contributed to meeting both restorative objectives and the aesthetic demands of the patient. Whenever crown lengthening is planned, the biological width must be considered, for if it is encroached upon, periodontal destruction may follow, leading to gingival recession.10 Crown lengthening procedures were carried out on teeth 24 and 46 in the Department of Periodontics (Figure 5a and b). A prefabricated threaded metal post was placed in both 24 and 46 to increase crown structure for crown placement.
The diagnostic casts were made from impressions taken in alginate. Orientation relation was recorded using face bow transfer, whilst centric relation was recorded with putty bite registration paste (Figure 6). Since the patient was missing the 22, the crown of the 23 was modified to mimic the shape of the lateral incisor. Crown preparations were done with shoulder finish lines on 11, 12, 15, 16,21 23 24, 26, 46 and36. Gingival foam cord was used for tissue retraction. Poly vinyl siloxane putty wash impressions were taken.

Temporisation was effected using self cure acrylic resin and cemented using non-eugenol cement. Definitive metal ceramic crowns were cemented using Type I Glass ionomer cement (Figure 7a and b). The appearance of the patient was markedly improved. He was instructed to reduce his sugar consumption, and to intensify his oral hygiene practices, i.e. brushing twice daily with fluoridated toothpaste. The need to brush before going to bed was emphasized and the use of 0.2% Chlorhexidine mouthwash twice a day for one month was prescribed.

DISCUSSION
Dental caries is one of the most prevalent oral diseases of public health concern affecting adolescents.1 Untreated caries can result in pain and adversely affect quality of life.2,6 Present studies suggest that dental caries is a mul-tifactorial disease, involving micro-organisms, substrate, host, and factors related to the teeth and time.7-9 The World Health Organisation (WHO) defines "adolescents" as individuals between the age of 10 and 19 years.2,8 This age group constitutes 20% of the world's population.10 Adolescents are considered as an important target group for oral health promotional activities as behaviour and attitudes formed during adolescence may last into adult life.11 Most adolescents attend schools, therefore, it might be easy to organise and target preventative care for this age group.
Good communication with the patient and effective interdisciplinary treatment planning was critical to patient satisfaction in this example of aesthetic dentistry. Three specialties of Dentistry, namely, Endodontics, Periodontics and Prosthodontics were involved. Crown lengthening was done without osteoplasty because of the availability of sufficient biological width, allowing a consistent 3mm gain. The face-bow transfer recorded the relationship of the maxilla to the transverse horizontal hinge axis of mandible. Endodontic treatment was chosen over implants because of cost factors and the inherent limitations of implants.12 Dentists, dental hygienists, and related health professionals should be aware of the unique aspects of treating adolescents, and be willing and able to spend time on prevention and diet counseling. Preventive measures such as prescription-strength fluoride gels for home use, fluoride varnishes, and other interventions may need additional emphasis for those individuals exhibiting increased caries susceptibility.13
CONCLUSION
This article illustrates the importance of proper and logical treatment planning as well as clear communication between the dental team and the patient regarding the outcomes of the planned dental treatment. Favourable aesthetics and a functional result can only be achieved if the clinician is communicating well with the patient, and plans a logical treatment sequence. The complexity of a case can be reduced if management is broken down into separate phases of treatment that can be addressed sensibly. For this patient, the treatment outcome exceeded his expectation. Certainly, his quality of life has greatly improved.
References
1. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ 2005; 83 : 661-9. [ Links ]
2. Slade GD. Epidemiology of dental pain and dental caries among children and adolescents. Community Dent Health 2001; 18: 219-27. [ Links ]
3. CDC/NCHS, National Health and Nutrition Examination Survey (NHANES) collected between 2005-2006. [ Links ]
4. Guidelines on Adolescence Health Care: Reference manual, American Academy of Pediatric Dentistry.151-8. [ Links ]
5. Shepherd MA, Nadanovsky P, Sheiham A. The prevalence and impact of dental pain in 8-year-old school children in Harrow, England. Br Dent J 1999; 187 : 38-41. [ Links ]
6. Okullo I, Astrom AN, Haugejorden O. Social inequalities in oral health and use of oral health care services among adolescents in Uganda. Int J Paediatr Dent 2004; 14: 326-35. [ Links ]
7. Eriksen HM, Dimitrov V. Ecology of oral health: a complexity perspective. Eur J Oral Sci 2003; 111: 285-90. [ Links ]
8. Kidd EAM, Mejare I, Nyvad B. Clinical and radiographic diagnosis. In: Fejerskov O, Kidd EAM, editors. Dental Caries: The Disease and its Clinical Management. Oxford: Blackwell Munksgaard; 2003;111-28. [ Links ]
9. Fejerskov O. Changing paradigms in concepts of dental caries: Consequences for oral health care. Caries Res 2004; 38: 182-91. [ Links ]
10. Petersen PE. The World Oral Health Report 2003: Continuous Improvement of Oral Health in the 21st Century--the Approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol 2003; 31 : 3-24. [ Links ]
11. Barton J, Parry-Jones W. Adolescence. In: Detels R, McEven J, Beaglehole R, Tanka H, editors. Oxford Textbook of Public Health: The Practice of Public Health. 4th Ed. Oxford: Oxford University Press; 2000; 1623-38. [ Links ]
12. Majewski RF. Adolescent caries: a discussion on diet and other factors, including soft drink consumption. J Mich Dent Assoc. 2001;83(2):32-4 [ Links ]
13. Mahmoud Torabinejad, Charles J. Goodacre. Endodontic ordental implant therapy: the factors affecting treatment planning. JADA. 2006;137:973-7. [ Links ]
 Correspondence:
Correspondence:
Kabbinale Pradeep
Associate Professor, Department of Conservative Dentistry & Endodontics
Manipal College of Dental Sciences, Manipal University, Manipal
576104, Karnataka, India
Cell: +91 973 944 2258, Fax: 0820 257 1966
E-mail: endopradeep@gmail.com
