










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.71 n.3 Johannesburg Apr. 2016
RESEARCH
The whitening effect of four different commercial denture cleansers on stained acrylic resin
R MaartI; SR GroblerII; HW KruijsseIII; Y OsmanIV; N PatelV; D MoodleyVI
IBChD, PG Dipl. Senior Lecturer, Community Dentistry.Oral and Dental Research Institute, Faculty of Dentistry, Tygerberg Campus, University of the Western Cape, Cape Town, South Africa
IIDSc, PhD. Professor, Dental Materials. Oral and Dental Research Institute, Faculty of Dentistry, Tygerberg Campus, University of the Western Cape, Cape Town, South Africa
IIIPhD. Professor, Statistical Analysis. Oral and Dental Research Institute, Faculty of Dentistry, Tygerberg Campus, University of the Western Cape, Cape Town, South Africa
IVBChD, MChD, BBA (Hons), MBA, PGD HM. Dean. Oral and Dental Research Institute, Faculty of Dentistry, Tygerberg Campus, University of the Western Cape, Cape Town, South Africa
VBDS, MChD, PDD. Specialist, Restorative Dentistry.Oral and Dental Research Institute, Faculty of Dentistry, Tygerberg Campus, University of the Western Cape, Cape Town, South Africa
VIPhD, FLCD, PDD, BDS. Specialist, Restorative Dentistry.Oral and Dental Research Institute, Faculty of Dentistry, Tygerberg Campus, University of the Western Cape, Cape Town, South Africa
ABSTRACT
Denture hygiene and denture cleansers are very important for their antimicrobial effect and also in removing stain from the dentures. The purpose of this study was to determine the effectiveness of Steradent, Corega, Dentalmate and Fitty Dent in improving the colour of stained, polished-and unpolished, acrylic specimens and to determine which colour component should be the visual impression factor. Samples of stained acrylic specimens were severally exposed once to one or other of the denture cleansers. The colour components (L*, a* and b*) of the specimens were measured with a spectrophotometer before and after exposure to one of the four products. In general there was only a slight non-significant improvement (p>0.05) in the yellowness (a*) and redness (b*) of the acrylic samples as a result of a single treatment with any of the four stain removal products. However, the L* value was mainly negatively influenced. The differences (ΔE*ab; ΔL*; Δa* and Δb*) between before and after treatment for any one of the four products were also not statistically significant on a 5% level (Kruskal Wallis non-parametric test).
CONCLUSION: A small improvement of the yellowness and redness could be seen even after a single treatment. This was found for all four commercially available denture cleansers on polished and on non-polished specimens. From the relative magnitudes of L*, a* and b* which contribute to the overall colour value (ΔE*ab) it was statistically confirmed that the brightness/lightness component (L*) should be the visual impression factor.
INTRODUCTION
The hygienic maintenance of dentures by the use of denture cleansers is important for the general oral health of patients and to ensure an odour free appliance. The microporous surface of an acrylic resin denture base material provides an environment that supports microorganisms. Microbial plaque on dentures has the potential to be harmful to both the oral mucosa and to the general health, therefore cleaning and the maintenance of the dentures are essential. Denture cleaning is necessary to remove extrinsic stain and soft and hard deposits from dentures. An ideal denture cleanser should be simple to use, effectively remove organic and inorganic matter from denture surface, have bactericidal and fungicidal properties, be compatible with all denture base materials1,2 and be economical. Cleansers are also expected, importantly, to remove stains from dentures to improve their colour. Dental students at the University of the Western Cape (UWC) provide, on average, some 500 dentures to patients annually. On delivery, oral hygiene instruction and specific details on the care of the prostheses are given to thee patients by the students. An instruction sheet detailing denture hygiene is handed to the patients to reinforce the message and four denture cleansers are recommended. Extrinsic staining of acrylic dentures can be a major problem for many individuals especially those who smoke tobacco products or consume large quantities of tea, coffee, cola or red wine.3 Steradent denture cleanser powder, Corega denture cleaner tablets, Dentalmate denture cleanser tablets and Fitty Dent denture cleanser tablets are the denture cleansers recommended at UWC and are currently commercially available amongst several other competing brands, some claiming to have superior stain-removal properties.
Denture cleansers may be divided into two groups: paste and immersion types. The complex composition of cleaning pastes with their abrasives, humectants, detergents and flavouring provides a variety of potential effects on the denture surface. The roughness of materials might affect plaque formation or inhibit its removal. Immersion type denture cleansers contain no abrasive particles; and the only means of abrading the denture surface would therefore be during the brushing phase before or after soaking.4 Information on the efficacy of the different types of cleansers and the effectiveness of individual additives in removing stain can be difficult to establish because of alterations in formulations of existing products or the introduction of newbrands.3,5
The rate at which deposits accumulate on dentures varies between individuals and can be affected by factors such as dietary intake, saliva composition, surface texture and porosity of the denture base material, the duration for which the dentures are worn and the denture-cleaning regimen adopted by the wearer. Sterilization by immersing dentures leaves the surface roughness of the denture resin unchanged and therefore possibly less susceptible to plaque accumulation. One of the main cleaning chemicals in immersion type cleansers is sodium hypochlorite. These types of cleansers can lead to deterioration of the denture base material, such as bleaching of acrylic resin, corrosion of metal and decomposition of temporary and soft lining material.4
Effervescent tablets are classified as chemical soak-type products and when dissolved in water the sodium perborate readily decomposes to form an alkaline peroxide solution. This peroxide solution subsequently releases oxygen thereby enabling a mechanical cleaning by the oxygen bubbles in addition to the chemical action.6
It is of clinical importance to determine whether denture cleansers alter the properties of acrylic resins. Denture base polymers are susceptible to colour-shifting if the cleaning solutions are not used correctly. The whitening effect may relate to a high temperature of the water used in the solution.6 Whitening of the denture colour has also been correlated with the regular use of chemical denture cleansers.2 Irregularities and porosities present on denture surfaces offer a favourable niche to retain stain and microbial plaque.6
The purpose of this study was to determine the relative effectiveness of Steradent denture cleanser powder, Corega denture cleanser tablets, Dentalmate denture cleanser tablets and Fitty Dent denture cleanser tablets in the colour improvement of stained, polished- and unpolished, acrylic specimens and to determine which colour component should be the visual impression factor.
MATERIALS AND METHODS
Sample discs were prepared using heat cure acrylic resin. Identical rectangular wax discs were constructed from a silicone mould, invested, the wax boiled out, replaced by pink acrylic resin and the sample cured as for denture processing. Some of the discs were finished and polished as is routinely done in denture construction6 and the rest of the acrylic specimens were finished but not polished (as in the fitting surfaces of dentures).
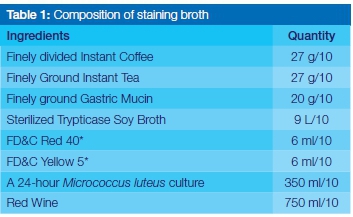
The specimens were washed in distilled water to remove any debris. Specimens in groups of 10 (five polished surface and five specimens not polished, (n=40) were used for each product in the study. A staining broth was prepared as described by the American Dental Association,7 comprising a mixture of coffee, tea, mucin powder, sterilized trypticase soya broth, FD&C Red and Yellow colour along with red wine and a 24-hour culture of Micrococcus luteus (Table 1).
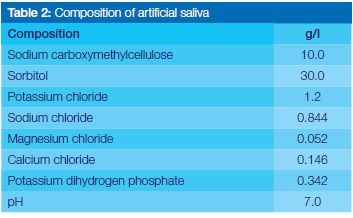
The specimens were first placed in artificial saliva (Table 2; Cipla Medpro, Bellville, RSA) for 2 minutes to form an initial pellicle layer to facilitate the uptake of the stain, and then washed with distilled water.
The specimens were then soaked in the prepared staining solution for 48 hours, after which the uptake of the stain was visible with the naked eye. They were removed from the staining solution, washed in distilled water and allowed to air dry.
The colour components (L*, a* and b*) of each specimen were measured before soaking and after being soaked in the cleansers (Table 3). This was done with a spectropho-tometer (Konica Minolta, CM-2600d) and the data were recorded.
Each denture cleanser solution was mixed as per manufacturers' directions. Corega denture cleanser tablets (Glaxo SmithKline South Africa (Pty) Ltd), Fitty Dent denture cleanser tablets (Fitty Dent International GMBH) and Dental Mate denture cleanser tablets (Dis-Chem Pharmacies, RSA) were separately dropped into 250ml warm water to dilute. Steradent powder (1/4 capful) (Reckit Benckiser, RSA) was put in 250ml of warm water. Specimens were soaked in the various denture cleanser solutions for periods according to the directions supplied by the respective manufacturers. Hence in the Corega denture cleanser tablet solution, specimens were soaked for 3 minutes, those in the Fitty Dent denture cleanser tablet solution were soaked for 5 minutes, and those in the Dental mate denture cleanser solution were soaked until the effervescing solution changed from blue to clear. Specimens in the Steradent denture cleanser powder solution were soaked for 10 minutes. As the intent of the tests was to evaluate the change in colour, if any, effected by the different treatments, no control group, such as water, was used. Each of the specimens was then rinsed thoroughly for one minute with distilled water and air-dried. The colour change as a result of the removal of the stain was measured using the above mentioned spectrophotometer.
The composition of the dental cleansers is given in Table 3.
The spectral distributions of the acrylic samples were compared by determining the three dimensions of their L*a*b* colour space. In the three dimensional space, ΔL* represents the brightness/whiteness dimension, Δa* the dimension of the opponent colours green/red and Δb* the dimension of opponent colours blue/yellow.
The L*a*b* space consists of coordinates that vary in a finite range. For example, brightness/whiteness could range between zero and 100 where zero would be pitch dark and 100 maximum white/bright. Figure 1 demonstrates the colour space of the L*a*b* system.8

To gain insight as to which of the three different components (ΔL*, Δa* and Δb*) would determine the visual impressions of the total colour change (ΔE*ab) the inter-relationships between the three deltas was further investigated using a two dimensional principal component analysis (CATPCA).
RESULTS
Delta E (total colour difference) values for all four products were calculated using the following formula8:
ΔE*ab = [ ( ΔL*)2 + (Δa* )2 + ( Δb* )2 ]1/2
Where: L* indicates (-)darkness/lightness(+), a* (-)green/ red(+) and b* (blue/yellow(+). These are the chromaticity coordinates.
In general, there was only a small and insignificant improvement (p>0.05) in the overall colour (ΔE*ab) of stained specimens as a result of a single treatment with any one of the four stain removal products. Since the sample sizes were small (n=10) the Kruskal Wallis non-parametric Test was used. The differences between the three colour components (ΔL*; Δa* or Δ b*) before and after treatment of the stained samples for any one of the four products were also small and not statistically significant on a 5% level. There was also no significant difference between non-polished (stained) and polished (stained) in ΔE*ab ; ΔL*; Δa* or Δb* Kruskal Wallis non-parametric test).
The overall mean ΔE*ab (colour improvement) for the four different products on the polished specimens was 2.46 (sd=2.11). For the non-polished specimens the overall mean ΔE*ab was 2.58 (sd=3.0) and the performance of the four products also did not differ significantly (p<0.05).
The results of a two dimensional principal component analysis (CATPCA) with ΔL*, Δa*,Δb* revealed that it was not the difference between Δa* and Δb* but the difference between one of these components and ΔL* that is crucial to the visual impression.
This is apparent from Figure 2 which shows that AL* largely contributes to dimension 2 whereas Δa* and Δb* dominate dimension 1. This and the high correlation between Aa* and Δb* suggest that changes in ΔL* will be prominent in the spectral distribution of the cleansers used in this study whereas the relative differences between Δa* and Δb* will have only a marginal effect.
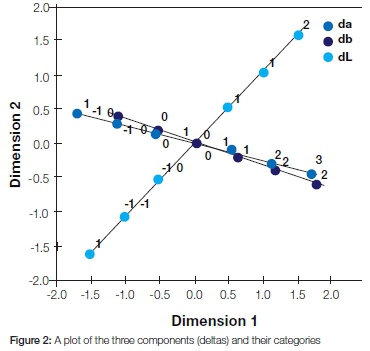
Category values of the deltas are in decimals but for readability purposes are presented here as integers. The two-dimensional solution with eigen-values d1=2.16, d2=0.673 explained 94.4% of the total variance.
DISCUSSION
There are a number of factors which could influence the determination of the whitening capability of a denture cleanser i.e.: the type of stain initially used, the stained product, the number and time of treatment with denture cleansers and the way the effect of stain removal was measured.
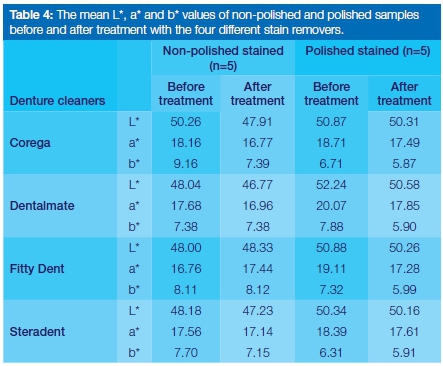
A small improvement in the colour of the stained resin (Table 4) was found as a result of only one treatment, whether polished or not polished. In general, the L* values indicated a deterioration but there was a small improvement in the a* values (less positive) (Table 4) for the non-polished as well as polished samples indicated an improvement in the colour (less reddish), as did also the b* values (less yellowish). No significant differences in the whitening abilities of these denture cleansers were found when the specimens were soaked once in a denture cleanser (short periods as mentioned). However, it could be expected that multiple treatments (longer treatment periods) may result in a significant colour improvement as a consequence of repeated or prolongued exposures (Table 4). It was recently stated that discolouration of three different denture resins did occur when subjected to different staining agents (coffee, cola, grape juice) but also that the colour of the resins was subsequently improved by the denture cleansers.9 However, in contrast to our study the specimens were soaked for 12 hours in denture cleansers after staining. In another study10 where acrylic denture teeth (shades A1, B1, C1) were exposed for 10 hours daily over 48 weeks to various denture cleansers, clinically acceptable colour changes (delta E* of 3.5) were reported. Imirzalioglu et al11reported a clinically observable colour shift (delta E < 3.7) as a result of exposure to tea, coffee and nicotine for days. Unlu et al2, also reported the whitening effect of four different types of agents on six different types of acrylic resins. However, none reported any of the components (L*, a*, b*) separately but considered only the total colour change.
If it is assumed that the degree of stain removal could also give an indication of the whitening improvement, it is valid to compare the present results with the findings of previous studies. In a recent article12 the stain removal ability of eight denture cleansers on acrylic resin was determined. In agreement with our results on whitening the authors concluded that all denture cleansers had a capacity to remove stain. However, they measured the optical density change of the stain remover and not the direct colour change on the specimen as we did. In agreement with our results, they found a change for most cleansers (except one) after only one cycle process of 1 minute and also an increase in improvement with increasing numbers of cycles (up to 5 times). Furthermore, they stained the acrylic resin with chlorhexidine and tea whereas we used the staining broth recommended by the American Dental Association7 which included many different products namely: a mixture of coffee, tea, mucin powder, sterilized trypticase soya broth, FD&C Red and Yellow colour along with red wine and 24hour culture of Micrococcus luteus. Thus, it could be expected that our staining should be more intense and difficult to remove but it does simulate the in vivo situation more closely. Also in agreement with our results, another study3 concluded that all the commercial denture cleansers removed stain. However, in that instance the tests were done on polystyrene plates and not acrylate and the investgators used chlorhexidine and tea as staining solution.
Our specimens were placed in artificial saliva to build up an initial pellicle layer to more closely mimic the clinical scenario. All four denture cleansers are readily available in South African shops and pharmacies. All the denture cleansers contain various ingredients with the most common being sodium bicarbonate, which acts as a buffer and provides an alkaline environment. The alkaline substances most frequently employed in denture cleansers are the phosphates, carbonates and silicates.13 All four denture cleansers in our study contain some of these alkaline substances (Table 3). The pH values of all our products were measured: Corega 7.9, Fitty Dent 9.1, Dental Mate 8.5 and Steradent 6.4. Steradent has the lowest and slightly acidic pH and the three other products have alkaline values, with Fitty Dent the highest. Differences in the pH values of cleansing solutions were reported to play a role in the whitening effect of acrylic resins.2 Alam et al3concluded that a denture cleanser containing sodium percarbonate (sodium carbonate peroxide) and sodium lauryl sulphate was particularly effective in stain removal via a chemical action. Corega, Dental Mate (Dischem) and Steradent all contain sodium lauryl sulphate (soap) (Table 3), Corega and Fitty Dent contain sodium perborate. Steradent, Dentalmate and Corega all contain citric acid and sodium bicarbonate (Table 3); citric acid may assist with stain removal and sodium bicarbonate is recognized as a whitening agent.3
In this study, some of the specimens were smoothed and polished, but in a previous study5 it was suggested that the texture and amount of porosity of the denture surface play a major role in retaining stain and microbial plaque. These surface defects may favour the initial formation of plaque by protecting the organisms from dislodgement and could make complete removal of plaque and stain by physical means difficult.5 However, the current study did not show a statistically significant difference, although it is accepted that there was only one short treatment.
An interesting question which now emerged is which of the three different colour components (ΔL*, Δa* and Δb*) would determine differences in the visual impressions of the total colour change (ΔE*ab).
The fact that the two-dimensional solution (Figure 2) explained 94.4% of the total variance would imply that the differences between Aa* and Ab* of the materials in this study would be difficult to detect when presented to subjects (the human eye) and that it is rather the brightness/lightness which would determine the differences of the visual impressions of E*ab's.
CONCLUSION
A small improvement in the yellowness and redness could be seen even after a single treatment. This was found for all four different commercially available denture cleansers on polished or non-polished specimens. From the relative magnitudes of L*, a* and b* which contribute to the overall colour value (ΔE*ab) it was shown that the brightness/lightness component (L*) should be the visual impression factor.
CLINICAL RELEVANCE
A slight improvement on the yellowness and redness could be seen after even a single treatment with any of the four different commercially available denture cleansers.
ACRONYM
UWC: University of the Western Cape
FD&C: Food, Drug and Cosmetic
References
1. Sato S, Cavalcante M, Orsi I, Paranhos H, Zaniquelli O. Assessment of flexural strength and color alteration of heat-polymerized acrylic resins after simulated use of denture cleansers. Brazilian Dental Journal 2005; 16: 124-8. [ Links ]
2. Unlu A, Tugrul Altay O, Sahmali S. The role of denture cleansers on the whitening of acrylic resins. International Journal of Prosthodontics 2006; 9(3): 266-70. [ Links ]
3. Alam M, Jagger R, Vowles R, Moran J. Comparative stain removal properties of four commercially available denture cleaning products: an in vitro study. International Journal of Dental Hygiene 2010; 9: 37-42. [ Links ]
4. Harrison Z, Johnson A, Douglas W. An in vitro study into the effect of a limited range of denture cleansers on surface roughness and removal of Candida albicans from conventional heat-cured acrylic resin denture base material. Journal of Oral Rehabilitation 2004; 31: 460-7. [ Links ]
5. Jagger D, Al-Akhazami L, Harrison A, Rees J. The effectiveness of seven denture cleansers on tea stain removal from PMMA acrylic resin. The International Journal of Prosthodontics 2002; 15(6): 549-52. [ Links ]
6. Peracini A, Davi L, Ribiera N, de Souza R, da Silva C, Paranhos H. Effect of denture cleansers on physical properties of heat-polymerized acrylic resin. Journal of Prosthodontic Research 2010; 54: 78-83. [ Links ]
7. American Dental Association (2008) In-office whitening agents: laboratory testing methods. ADA Professional Product Review,3:http://www.ada.org/sections/scienceAndResearch/pdfs/0804_whitening _testmethods.pdf (retrieved on Feb, 2013). [ Links ]
8. Minolta, Precise color communication, Minolta, Co., Ltd., Osaka, Japan, 1994; 9242-4830-92 IHCAJ. [ Links ]
9. Hollis S, Eisenbeisz Ε, Versluis A. Color stability of denture resins after staining and exposure to cleansing agents. J Prosthet Dent 2015; doi: 10,1016/j.prosdent.2015.06.001. [ Links ]
10. Moon A, Powers JM, Kiat-Amnuay S. Color stability of denture teeth and acrylic base resin subjected daily to various consumer cleansers. J Esthet Dent 2014; 26: 247-55. [ Links ]
11. Imirzalioglu P, Karacaer O, Yilmaz B, Ozmen Ml. Color stability of denture acrylic resins and softlining material against tea, coffee and nicotine. J Prosthodont 2010; 19: 118-24. [ Links ]
12. Al-Huraishi H, Moran L, Jagger R, MacDonald E. Evaluation of stain removal and inhibition properties of eight denture cleansers: an in vivo study. Gerodontology 2013; 30: 10-7. [ Links ]
13. Anthony D, Gibbons P. The nature and behaviour of denture cleansers. J Prosthet Dent 1958; 8: 796-810. [ Links ]
 Correspondence:
Correspondence:
Sias R Grobler:
Oral and Dental Research Institute, Faculty of Dentistry, Tygerberg Campus
Private Bag X01, Tygerberg 7505.
Tel: +27 21 937 3023/24
E-mail: srgrobler@uwc.ac.za

{kind=link}