










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.70 no.10 Johannesburg nov. 2015
RESEARCH: REPRINT
Patient satisfaction during and following procedural sedation for ambulatory surgery
C LapereI; J RoelofseII; Y OmarIII; A du PlessisIII; A von BackstromIV; W BothaIV; C CookIV; G BoschIV
IUniversity of the Western Cape, Cape Town, South Africa
IIUniversity of the Western Cape, Cape Town, South Africa, University College, London, UK
IIIEastman Dental Institute, Sedation Solutions, London, UK
IVSedation Solutions, London, UK
ABSTRACT
BACKGROUND: Patient satisfaction is multidimensional. The clinician's perspective of a good outcome and the patient's experience of a satisfactory service are often two different end-points. The primary aim of our study was to assess the perioperative experience of patients undergoing procedural sedation. A secondary aim was to create a postoperative questionnaire which could be used as a measurement tool. The questions could also be used as an audit to assist with adherence to quality assurance and clinical governance.
METHOD: A questionnaire was compiled to attempt to assess the perioperative aspects of procedural sedation. Five hundred consecutive patients undergoing procedural sedation for dental-related outpatient procedures were asked to complete a questionnaire. Patients who didn't complete it were excluded. Ninety-eight per cent of the patients returned the questionnaire and 489 questionnaires were evaluated.
RESULTS: A total of 489 patients were included. Ninety-three per cent of the patients expressed a good (7+/10) overall experience of procedural sedation, and 92.6% indicated that they would recommend it to others.
CONCLUSION: Our study population showed a high level of satisfaction with their sedation experience. It is suggested that the devised questionnaire could be used successfully in future as an assessment tool or audit of patient satisfaction following procedural sedation for ambulatory surgery.
Keywords: patient satisfaction, postoperative questionnaire, procedural sedation
INTRODUCTION
The concept of procedural sedation is widely accepted for managing pain and anxiety for procedures outside the operating theatre. Defining patient satisfaction involves a multidimensional approach which includes clinical aspects of care, safety, and patients' perception of a satisfactory outcome.
Procedural sedation is a rapidly expanding field. It is an alternative to general anaesthesia within the scope of widening ambulatory surgery. Patients are often poorly informed of what procedural sedation entails, and want reassurance that even though they are not unconscious, as in the case of general anaesthesia, they will still be comfortable, and without pain and anxiety while in the chair.
Measuring clinical outcomes is limited by a lack of validating instruments. Mortality and length of hospital stay are commonly used variables. However, neither is applicable in the case of elective ambulatory surgery.1
Patients expect more from an anaesthetic than merely being able to wake up afterwards.2 For example, post-operative nausea and vomiting (PONV) after general anaesthesia can increase the cost of the total health care by increasing recovery room time and potential hospital admission. It is equally important that patients are dissatisfied and uncomfortable with PONV.3 Patients report that avoiding PONV is of greater importance than preventing postoperative pain.4
Patients are viewed as customers who expect a certain standard of care in a service delivery-driven world.4 Patient autonomy gives patients the right to partake in a number of available treatment options.
According to local sedation guidelines,5 an annual audit needs to be conducted of the performance of every practice for clinical governance and quality assurance. The primary aim of our study was to assess the peri-operative experience of patients undergoing procedural sedation for ambulatory dental procedures. A secondary aim was to create a postoperative questionnaire which could be used as a measurement tool. The questions can also be used as an audit to assist with adherence to quality assurance and clinical governance within a practice setting.
METHOD
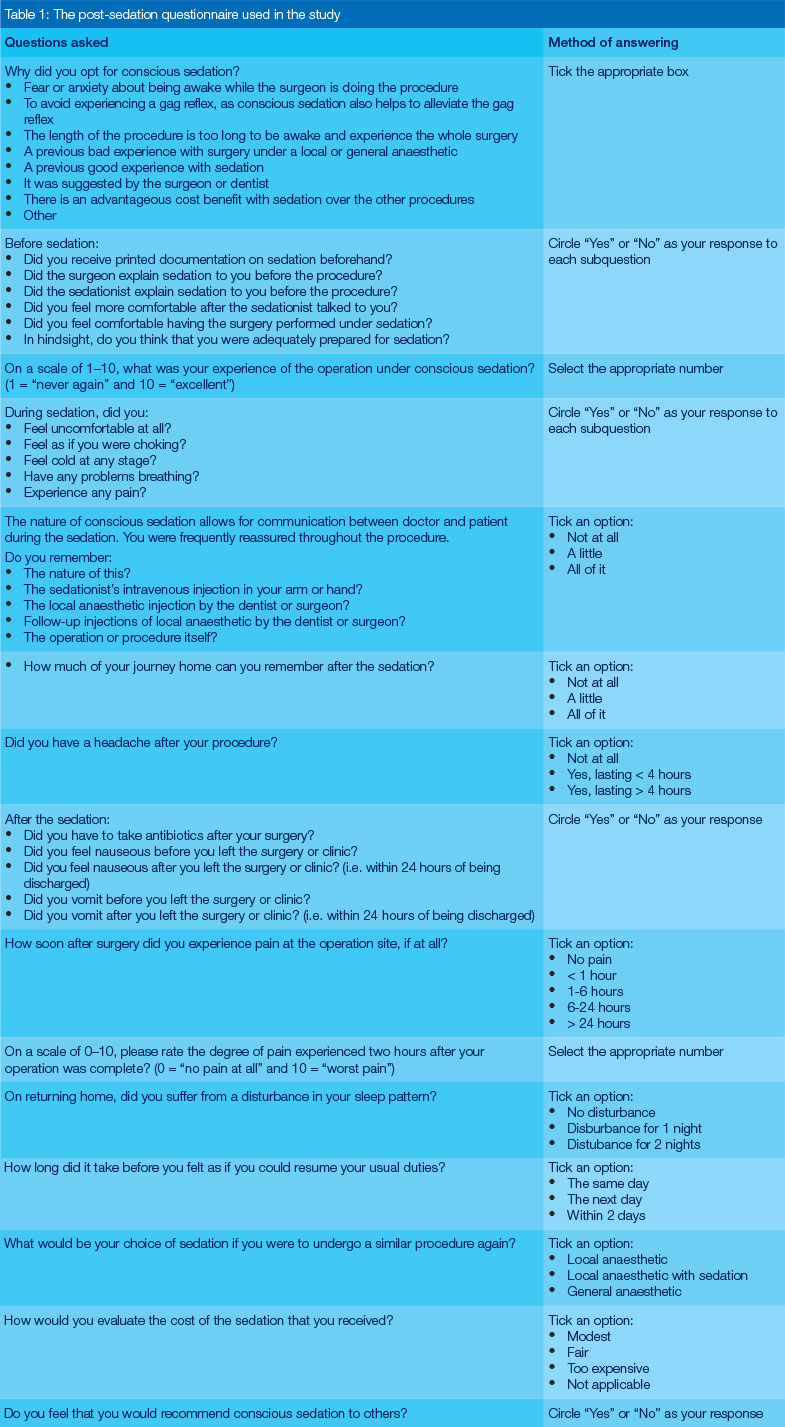
The questions were designed based on the entire peri-operative experience, starting with the indications and preoperative information given. Questions on the procedure itself, immediate postoperative time and the following 48 hours, based on common side-effects experienced, were also included. The questions were based on existing questionnaires that have been in use at our facility. A total of 28 questions was listed. The questionnaire is included in Table 1 in its entirety.
During August 2014, 500 adult patients who received procedural sedation for dental-related procedures were included in this study. They were asked to complete the questionnaire. A total of 490 patients (98%) returned it. The patients received it in a stamped envelope at the time of their procedure, and were asked to return it via mail or at their first follow-up visit. Patients who failed to complete the questionnaire were excluded. Patients' responses remained confidential and anonymous.
Four hundred and eighty-nine questionnaires remained for analysis. All questions in the remaining eligible questionnaires were assessed separately and a record was kept of unanswered questions. We expressed each unanswered answer as a percentage of the total assessed (489).
Patients underwent procedural sedation, in which advanced techniques were utilised. Advanced sedation techniques are defined as the use of a combination of sedative and/or analgesic drugs administered via any route, or by using intravenous sedation, with the exception of titrated dosages of midazolam, or by target-controlled infusion.5 Patients received a combination of titrated midazolam, propofol and a small dose of ketamine immediately before the local anaesthetic injection.
Moderate sedation and analgesia levels were targeted and achieved for patients. This is defined as the drug-induced depression of consciousness, during which the patient responds purposefully to verbal commands, either alone or accompanied by light and tactile stimulation. Intervention is not required to maintain a patent airway. Spontaneous ventilation is adequate. Cardiovascular function is usually maintained.
RESULTS
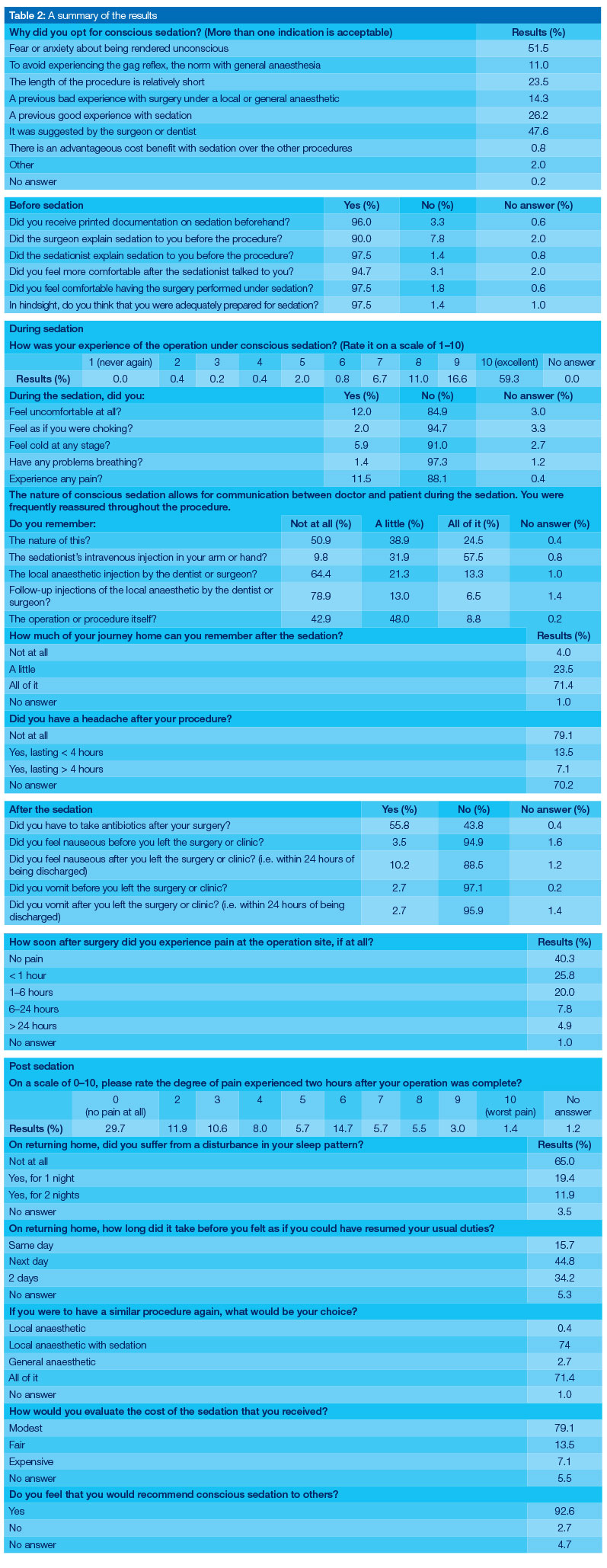
In studies done that utilizes mail to communicate information to and from patients, a response rate of 50% for mailing methods was considered to be adequate for analysis.6 Of the 500 patients in this study, 98% returned their questionnaire. The results are summarised in Table 2.
Preoperative experience
Two hundred and fifty-two patients (51.5%) opted for procedural sedation due to fear or anxiety of being awake during the procedure, while 233 patients (47.6%) had been recommended sedation. Four hundred and sixty-three patients (94.7%) felt more comfortable after discussing the procedure with the sedationist.
During sedation
Four hundred and fifteen patients (84.9%) reported that they never felt uncomfortable during the procedure, and 431 (88.1%) that they didn't experience any pain. Of the 489 patients, 315 (64.4%) couldn't remember the local anaesthetic injection.
After the procedure
Fifty patients (10.2%) felt nauseous after they left the clinic, and only 13 patients (2.7%) vomited. Four hundred and fifty-four (93%) patients expressed a good (7+/10) overall experience of procedural sedation. Four hundred and fifty-three (92.6%) patients would recommend it to others.
DISCUSSION
Overall, the patients were very satisfied with their experience of procedural sedation. They were well-informed about the procedure and sedation, as demonstrated by our study results. Patients recovered quickly, with minimal post-sedation sideeffects, which facilitated a speedy return to work and normal duties.
The response rate achieved using a mailed questionnaire is usually less than that obtained using an interviewing method. However, an extremely high response rate was accomplished in our study. This could possibly be explained by our chosen method of collecting the questionnaire. Patients could either mail the envelope back (the envelope was already addressed and stamped), or bring it with them to the first follow-up consultation. Patients had to return for a follow-up, making it easier to track their response to the questionnaire.
Chanthong et al.7 who reviewed 379 abstracts on patient satisfaction and ambulatory surgery, mostly performed under general anaesthetic, reported on a suggestion to create and develop a standard questionnaire to evaluate outcome. It was also proffered that further studies should be conducted and should utilise a rigorous methodological psychometric questionnaire to establish a standardised one to be used as the gold standard.7 Such a questionnaire has not yet been devised. Sparse literature is available on assessments of the perioperative experience of patients undergoing procedural sedation. We believe that our questionnaire covers the most important patient concerns. However, ideally, a validated assessment tool, which is comparable with the Iowa Satisfaction with Anesthesia Scale, is needed;8 the difference being that the Iowa Satisfaction scale was developed to assess patient satisfaction during Monitored Anaestesia Care, and not the perioperative period of sedation as in our case.
Chantong et al.7 noted that certain dimensions should be included in a questionnaire when assessing ambulatory anesthesia, including information on postoperative pain and home care management. The measuring instrument should also include questions on information provision, physical discomfort and emotional support, i.e. relaxed, reassuring and attentive.9 Our postoperative questionnaire contains all of these elements.
Eberhart et al.10 considered patient preference by interviewing patients after a preoperative visit where general information and the side-effects of anaesthesia were explained. Avoidance of PONV was a major concern of patients, followed by the desire to experience no or mild pain. The restoration of postoperative vigilance was of minor importance.10 It was clearly shown in our study that patients experienced a very low rate of nausea (10.2%) or vomiting (2.7%) following sedation. Four hundred and fifteen patients (84.9%) reported that they never felt uncomfortable during the procedure, and 431 (88.3%) that they didn't experience any pain.
Few studies, if any, are available in which patient satisfaction and the side-effect profile after procedural sedation is compared.
It is noteworthy that numerous patients in our study did not complete the last few questions, while those on the last page were often overlooked. It could be concluded that the questionnaire contained too many questions. It was evident from our responses given that 361 (74%) patients would opt for the option of local anaesthetic and procedural sedation in a future procedure. However, 107 (22%) of patients didn't answer this question.
A weakness of our study was that the focus was mainly on dental related procedures. It cannot be assumed that the expressed satisfaction would extend to other procedures. Also, the study population only consisted of adult patients.
CONCLUSION
A high level of satisfaction was demonstrated by our study population with their sedation experience. The postoperative sedation questionnaire is a useful tool with which to determine the perioperative experience of patients undergoing procedural sedation.
However, a validated assessment tool which can be used to audit the quality of sedation, train clinicians and establish protocolspecific guidelines for satisfactory procedural sedation is required. A possible suggestion is the identification of 8-10 core questions to be taken from this pilot study and included in a validated assessment tool.
Acknowledgements: Gratitude is extended to Sedation Solutions, London, UK, for use of the organisation's patient information. The contributions of administrative support and guidance, given by Daniel St John-Hore and Katie Heffer of Sedation Solutions, are also acknowledged.
Source acknowledgement: This article is reprinted with permission from the South African Journal of Anaesthesia and Analgesia 2015; 1(1): 1-6.
References
1. Grocott MPW, Browne JP, Van der Meulen J, et aí. The postoperative morbidity survey was validated and used to describe morbidity after major surgery. J Clin Epidemiol. 2007;60(9):919-28. doi: 10.1016/j. jclinepi.2006.12.003. [ Links ]
2. Smalhout B, Van Wijk M. Anaesthesia. Oct. 1990;45:679-82. [ Links ]
3. Gan TJ, Meyer T, Apfel CC, et aí. Consensus guidelines for managing postoperative nausea and vomiting. Anesth Analg. 2003;62-71. doi: 10.1213/01.ANE.0000068580.00245.95. [ Links ]
4. Macario A, Weinger M, Carney S, et aí. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg. 1999;89(3):652-8. doi: 10.1097/00000539-199909000-00022. [ Links ]
5. Analg A. Guidelines for the safe use of procedural sedation and analgesia for diagnostic and therapeutic procedures in adults. S Afr J Anaesthesiol Analg. 2010;16(4 Suppl 1):S1-24. [ Links ]
6. Babbie E. Chapter 3 survey. 2nd ed. Belmont, CA: Wadsworth Publishing; 1990. p. 257-318 [ Links ]
7. Chanthong P, Abrishami A, Wong J, et aí. Systematic review of questionnaires measuring patient satisfaction in ambulatory anesthesia. Anesthesiology. 2009;110(5):1061-7. doi: 10.1097/ ALN.0b013e31819db079. [ Links ]
8. Dexter F, Aker J. Development of a measure of patient satisfaction with monitored anesthesia care. Anesthesiology. 1997;87(4):865-73. [ Links ]
9. Rhodes L, Miles G. Patient subjective experience and satisfaction during the perioperative period in the day surgery setting: a systematic review. Int J Nurs Pract. 2006;12(4): 178-92. [ Links ]
10. Eberhart LHJ, Morin AM, Wulf H, et aí. Patient preferences for immediate postoperative recovery. Br J Anaesth. 2002;89:760-1. doi: 10.1093/bja/aef261. [ Links ]
This paper is reprinted with the kind permission of Ms Ina du Toit, Managing Head of Academic Publishing Services, MedPharm Publications (Pty) LTD and of the authors, represented by Professor James Roelofse. Our sincere appreciation is extended for this courtesy.

{kind=link}
{kind=link}