










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.70 n.8 Johannesburg 2015
CASE REPORT
Squamous Cell Carcinoma of the upper lip in an 8 year old child - a case report
K RajkumarI; CJ PerumalII; As SinghIII; M HainsworthIV
IBChD, Dip Odont (Oral Surgery). Division of Maxillofacial and Oral Surgery, Grey's Hospital, Pietermaritzburg, KwaZulu-Natal, South Africa
IIBDS. Specialist, Division of Maxillofacial and Oral Surgery, Grey's Hospital, Pietermaritzburg, KwaZulu-Natal, South Africa
IIIBDS, MDent (MFOS), MSc, MDS. Head Division of Maxillofacial and Oral Surgery Grey's Hospital, Pietermaritzburg, KwaZulu-Natal, South Africa
IVMBCHB, MMed (Anat Path). Division of Maxillofacial and Oral Surgery, Grey's Hospital, Pietermaritzburg, KwaZulu-Natal, South Africa
ABSTRACT
Squamous cell carcinoma (SCC) frequently occurs between the 5th and 7th decades of life. Its occurrence in adolescence is uncommon, and it is less common in children.1-4 South Africa has a kaleidoscope of social and ethnic belief systems which may influence the management of these patients. This case report presents a rare occurrence of a squamous cell carcinoma involving the upper lip in an eight-year-old child.
INTRODUCTION
Cancer of the lip may originate from the labial mucosa, the epithelium of the vermilion border of the lip, or from the accessory glands present at the vermilion-cutaneous and the vermilion-oral mucosal junctions respectively.5,6 Squamous cell carcinoma is the most common malignancy of the lip, but it rarely occurs in subjects under 20 years of age.1 The aetiological and predisposing factors of lip cancer include, excessive exposure to sunlight, tobacco usage, viral infections, racial factors, a genetic predisposition, immunosuppression, immunodeficiency, certain occupations and familial factors.5,6 We present an unusual case of an eight-year-old black female patient with a SCC of the left side of the upper lip.
CASE REPORT
An eight year old black female patient attended the Maxillofacial and Oral Surgery department of Grey's Hospital, Pietermaritzburg, KwaZulu-Natal, South Africa with a non-healing ulcer of the upper lip of seven months duration. There was no significant medical history. The lesion had started as a small ulcer which appeared spontaneously, and gradually increased to a size of approximately 10x15mm, with a central area of crusting (Figure 1). There were no palpable regional lymph nodes. A differential diagnosis of tuberculous (TB) ulcer, traumatic ulcer, syphilitic ulcer, human papilloma virus (HPV) related ulcer and pseu-doepitheliomatous hyperplasia was made. A biopsy of the lesion was performed under general anaesthesia.

HISTOLOGY REPORT
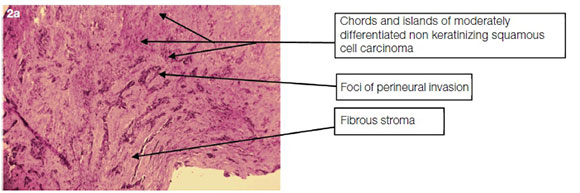
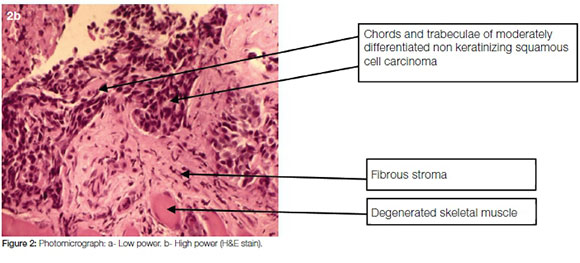
Histology showed extensive ulceration and the presence of an infiltrating tumour involving the subepithelial connective tissue and superficial orbicularis oris muscle. In the muscle, a focus of perineural invasion was observed. In one small focus, there was residual dysplastic squamous epithelium from which the tumour appeared to arise. The tumour was comprised of small dysplastic squamous cells staining positively with immunohistochemical stains CK5/6, P63 and P16. The overall histomorphological appearances and immunohistochemical staining characteristics were indicative of a moderate to poorly differentiated non-keratinising squamous cell carcinoma (Figure 2a and b). Polymerase chain reaction (PCR) for HPV infection was negative, though the expression of P16 by oropharyngeal squamous cell carcinomas is often indicative of HPV infection. However, Larque et al reported that the correlation is not absolute with 80% of such lesions testing negative for HPV by PCR,7 as was the case in this instance.
PLANNED TREATMENT
The patient was discussed with the Department of Plastic and Reconstructive surgery. An urgent surgical excision of the lesion was suggested. The patient and her mother were referred for pre-surgical counselling. During counselling, the mother expressed her family's cultural beliefs and stated that the child's father believed that the lesion had arisen because the spirits of their ancestors were displeased with something. He therefore believed that intervention by a traditional healer was the method of choice in the management of this malady. The mother on the other hand, expressed concern about her child not receiving surgical treatment. The father remained adamant about his beliefs. The patient subsequently failed to arrive for treatment and was lost to follow-up.
DISCUSSION
Squamous cell carcinoma is the most common head and neck neoplasm in the adult population above 60 years of age but is uncommon in adolescents and in children.8 Cancer of the lip may originate from either the labial mucosa, the epithelium of the vermilion border, or rarely (adenocarcinoma) from the sebaceous or minor salivary glands present at the vermilion-cutaneous or the vermilion-oral mucosal junctions respective-ly.5,6 Repeated exposure to ultraviolet light B (UVB, wavelength 290 - 320nm) causes lower lip actinic cheilitis. Ultraviolet light irradiates the deoxyribonucleic acid (DNA) within the nuclei of the non-keratinising epithelial cells of the vermilion border, inducing alterations in the p53 tumour suppressor gene,6 which is important in regulating cell division. Alterations in this gene renders it ineffective in limiting the proliferation of cells with altered DNA, thus promoting neoplasia.6
Tobacco usage has long been established as a causative agent for cancer of the lip and tongue with the most important carcinogen being nitrosamines.6 Conflicting reports have been published as to whether there is a direct link between lip cancer and tobacco use. However, it is believed that there is a synergistic effect between sunlight induced actinic cheilitis and tobacco usage, with sunlight reducing the permeability of the more superficial epithelial cells of the vermilion border, thus exposing the deeper cells to the carcinogens in tobacco.4-6 Viral infections may be a contributing factor in oral squamous cell carcinoma.6 Herpes simplex virus (HSV1) has the potential to transform cells in vitro. The potential for transformed cells to become malignant is increased by tobacco usage. The Human Papilloma Virus, most notably HPV-16 has been associated with oral SCC.6 Persons with light hair, eyes and skin are at a significantly higher risk of sunlight-related squamous cell carcinoma in general, and of the lip in particular. Lip cancer is 30 times more common in white men than in black men.6 The difference can be accounted for by the shielding effect of the pigment melanin.6,10 Cancers have been reported to arise in immunosuppressed patients, particularly those who have received organ transplants. The development of lip cancer in renal transplant patients who are on immunosuppressants has been reported.6 Although acquired immune deficiency syndrome (AIDS) patients are known to be susceptible to oral neoplasia, by 1998 only three AIDS patients with lower lip cancer had been reported.6 The use and abuse of tobacco and alcohol is uncommon in children. Short-term exposure is insufficient to induce neoplastic change.8 Stolk-Liefferink reported 65 cases of oral SCC in children, 22 cases in males and 15 in females, while the genders of 28 patients were unreported. The ages ranged from 2 to 20 years. In six of the 65 cases, SCC occurred on the lip, while 26 occurred on the tongue, four on the gingiva, one on the cheek and 28 sites were unreported.1 Tattemanti et al reviewed reports of oral SCC in 55 paediatric patients between 1894 and 2011 in which it was found that the most common site for oral SCC was the tongue (34 cases), while only three cases occurred on the lower lip.8 An increasing incidence of oral SCC in the younger population has been reported in several countries.1 Recent studies have reported it to occur with a frequency of approximately 4% of all oral neoplasms in patients younger than 40 years of age.1,8 Few cases of oral SCC occur in patients younger than 18years. The incidence is lowest in the first decade of life.8 Using the tumour, node and metastasis (TNM) staging of head and neck cancers, Salihu et al reported that the 10 year survival rates for stages I, II, III and IV for lower lip cancers are 91.7%, 83.7%, 28% and 11.4% respectively.9 They emphasised that early intervention is essential in order to achieve favourable survival rates. Chidzonga and Mahomva reported on 358 orofacial malignancies of which four (1.1%) occurred in the upper lip. These consisted of one well differentiated, two moderately differentiated and one poorly differentiated SCC, with an equal gender distribution.10
CONCLUSION
To the best of our knowledge this is the first case of a Squamous cell carcinoma of the upper lip, being reported in an eight-year-old child. Squamous cell carcinoma caused by HPV from sexual abuse was suspected in this case. The child was subsequently referred for counselling. The father of the child believed that their ancestral spirits were displeased for some reason. This has resulted in punishment being inflicted on the child in the form of an illness. This illness, he believed, could be managed with the help of a traditional healer. A belief in traditional medicine and traditional healers is common in South Africa, and is therefore likely to persist for a long time in the future. The co-existence of traditional medicine and belief systems in the 21st century can result in the delay of patients seeking medical or surgical intervention timeously. It is therefore necessary that the plight of such patients be brought to the attention of the law makers, the health professionals and the public at large. Failure to give this matter the seriousness that it deserves, could result in adverse outcomes.
Conflict of interest: None declared
References
1. Stolk-Liefferink SAH, Dumans AG, Van Der Meij EH, Knegt PP, Van Der Wal KGH. Oral squamous cell carcinoma in children; review of an unusual entity. Int J Pediatr Otorhinolaryngol 2008; 72: 127-31. [ Links ]
2. Bodner L, Manor E, Friger MD, Van Der Waal I. Oral squamous cell carcinoma in patients twenty years of age or younger - review and analysis of 186 reported cases. Oral Oncol 2014; 50: 84-9. [ Links ]
3. Solanki MC, Gandhi S, Koshy G, Mathew GC. Squamous cell carcinoma of maxilla in 10 year old boy: a rare case report. Int J Pediatr Otorhinolaryngol Extra 2012; 7: 33-5. [ Links ]
4. Cao Z, Wang Y, Ishikawa K, et al. Maxillary cancer in a child: a case report. Auris Nasus Larynx 2003; 30: 113-6. [ Links ]
5. Muir C, Weiland L. Upper aerodigestive tract cancers. Cancer 1995; 75(1 Suppl): 147-53. [ Links ]
6. De Visscher JGAM, Van Der Waal I. Etiology of cancer of the lip. A review. Int J Oral Maxillofac Surg 1998; 27: 199-203. [ Links ]
7. Larque AB, Hakim S, Ordi J, Nadal A, et al. High-risk human papillomavirus is transcriptionally active in a subset of sinona- sal squamous cell carcinomas, Mod Pathol 2014; 27, 343-51. [ Links ]
8. Tettamanti L, Caprioglio A, Tecco S, et al. Oral squamous cell carcinoma in the pediatric patient: A literature review. Eur J Paediatr Dent 2012; 13: 35-40. [ Links ]
9. Salihu S, Güven O, Gllareva E, Prekazi M, Salihu L. A clinical study on the survival rate of patients with squamous cell carcinoma of the lower lip in Kosovo. J Craniomaxillofac Surg 2014; 1-5. [ Links ]
10. Chidzonga MM, Mahomva L. Squamous cell carcinoma of the oral cavity, maxillary antrum and lip in a Zimbabwean population: A descriptive epidemiological study. Oral Oncol 2006; 42: 184-9. [ Links ]
 Correspondence:
Correspondence:
K rajkumar
Division of Maxillofacial and Oral Surgery, Greys Hospital
P.O Box 138676, Cascades 3202
Pietermaritzburg, KwaZulu-Natal, South Africa
Cell: 083 793 1913
E-mail: kavirraj@gmail.com
