










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.70 n.7 Johannesburg 2015
RADIOLOGY CASE
Maxillo-facial radiology case 134
CJ Nortjé
BChD, PhD, ABOMR, DSc. Faculty of Dentistry, University of the western Cape. e-mail: cnortje@uwc.ac.za
This 20 year-old male patient presented with periorbital and facial soft tissue masses of the left side of the face and a swelling affecting upper left maxilla (Figure.A, B). The patient also presents with mental retardation and epilepsy. What is your diagnosis?

INTERPRETATION
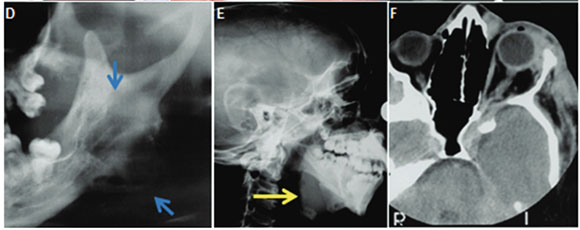
Cropped pantomograph showing sharply demarcated lytic lesions of left mandibular ramus and angle and an enlarged mandibular notch, red arrow (Figure C). Follow-up cropped pantomograph three years later showing subperiosteal "blister" lesion at left mandibular ramus, fusiform enlargement of the left mandibular canal, and "elongated" left condyle, blue arrows (Figure D). Lateral skull radiograph demonstrating neurofibroma subjacent to mandible which has resulted in upward displacement of lower border, yellow arrow (Figure E). Figure F is a coronal CT scan showing the soft tissue mass affecting the left orbit. A diagnosis of multiple neurofibromatosis was made. The classic description of this disease was given by von Recklinghausen in 1882 and the disease is often mentioned together with his name. The main features of the disease are the presence of multiple subcutaneous neurofibromas, and café au lait cutaneous pigmentation. Neurofibromatosis occurs in all races and is found in about 1 in 3,000 in the general population. Affected patients develop multiple neurofibromas. Superficial lesions are sessile or pedunculated, frequently consisting of numerous smooth-surfaced nodules that are widely distributed in the skin. Deeper, more diffuse lesions, or "elephantiasis neuromatosa" are often large in dimension. Moreover, most affected individuals have asymmetric areas of alanine pigmentation of the skin, termed café au lait spots. Intraoral neurofibromas occur in up to 20% of cases. When neurofibromas are present within the jaws, they are usually associated with the mandibular nerve, resulting in a fusiform enlargement of the canal with pain or paraesthesia. In the early literature, malignant transformation of neurofibromas was reported to occur in 15% of patients. Radiolucent defects involving the maxilla and mandible have been described in some cases. Generally the radiolucent areas are closely related to the foramina of the trigeminal nerve. The cardinal radiologic features are: fusiform enlargement of mandibular canal, sharply defined, and occasionally corticated radiolucency, subperiosteal "blister" lesion and enlargement of the jaw adjacent to a soft tissue tumour.
Reference
1. Farman AG, Nortjé CJ & Wood R E: Oral and Maxillofacial Imaging, 1st Ed, Mosby. St. Louis, Missouri 1993 p 134-136. [ Links ]
