










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.70 no.7 Johannesburg 2015
COMMUNIQUE
K Barnard
SADA Dental mediator, E-mail:dentalmediator@sada.ac.za
SUMMARY
By law you are required to provide your patients with a cost estimate and it is far better to do so in writing. It is a fact that more patients are prepared to make a formal complaint when they feel they have not been given the correct information about the cost of their treatment.
It is clear that more of your patients will challenge discrepancies in their billing and accounts. Without being able to raise their concerns at the practice, (even though the fault may be with the scheme or their benefits), patients will look to SADA and the HPCSA to help them correct an error. Dentists are required to discuss costs with their patients and record the discussions as you would with their treatment. If you take the time to do so, there might be less need for me to highlight this problem in the future.
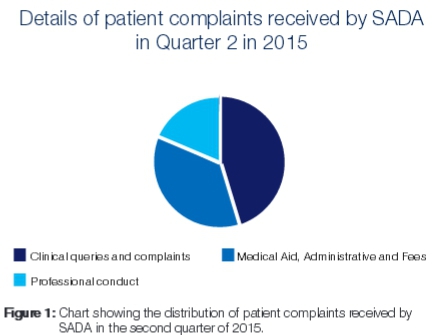
Without a doubt, the highest percentage of patient complaints received by the Dental Mediator are related to financial consent, and administration around medical aids. About 47% of patient complaints received in 2015 fell into this category. It was therefore decided during the Private Practice Committee meeting on 23 July 2015 that more information is needed by our members to help reduce and hopefully prevent complaints from patients in this regard. Traditionally dentists in South Africa have been reluctant to discuss costs with the patient before treatment is provided. This has resulted in an increase in dissatisfaction amongst patients who are making complaints in increasing numbers to the Health Professional Council. Quite rightly and by law, our patients have a right to know the expected cost of the treatment they require. They also have the right to know, and understand any alternative treatments available at the time. The consent is only valid if the patient has been given all the information about the likely costs of treatment and agrees to proceed on the basis that this is a cost estimate. If informed financial consent is obtained, and documented, complaints are less likely to arise and can be more easily defended.
MEDICAL AIDS
The administration around gaining pre-authorization, and establishing available benefits on behalf of the patient for certain procedures from Medical Aids remains a huge concern. By offering this valuable service to patients, a practitioner arguably undermines the patient's responsibility for the fees. It comes as no surprise then that most complaints received are because the patient was led to belief by the practice that the medical aid would cover the cost, and cannot possibly afford the shortfall/co-payment not paid by the scheme. In many cases the patients are saying they would not have proceeded with the treatment if they knew exactly how big the portion would be that they would have to contribute.
The complaints normally reach SADA/HPCSA when the dentist hands the account over to the debt collectors, and patients contact SADA out of desperation.
There are many technical challenges when dentists offer to establish available dental benefits, and gain authorisation from the patient's medical aid on behalf of the patient. The most common ones leading to complaints are:
• Most medical aids, especially Discovery, GEMS and Polmed would give telephonic confirmation of an available amount "at the time". The problem then occurs when other family members use some of these benefits when visiting the optometrist, doctor or pharmacy. Sometimes these fees are also deducted from the same "day to day OR savings account". By the time the dentist submits a claim for his treatment on behalf of the patient, there is an unexpected, inevitable shortfall of funds, and patients can't possibly pay the difference nor were they expecting to make a co-payment.
• There seems to be confusion between getting pre-authorization for certain specialized procedures, and actual available funds. Once pre-authorization is obtained from the medical aid, available benefits still need to be confirmed at the medical aid from a different internal department.
• The "scheme rules" of various different medical aids can vary so much, and there seems to be inconsistency, and confusion especially around which codes can be used from day-day fees vs. which codes are reserved for specialized dentistry. (For example code 8937 -Surgical removal of a tooth).
• Communication with medical aids can be very time consuming, frustrating and often unreliable, despite reference and authorization numbers.
Other common problems leading to complaints are:
• Dentists often exclude certain codes in the original treatment estimate. For example pre/post-operative x-rays, infection control, sutures, examination and follow-up fees. This can add up, and lead to a large discrepancy between the total cost and the original estimate.
• Patients see the treatment estimate as a "quotation" rather than a treatment estimate.
• Patients feel dentists charge exorbitant fees.
DISCUSSION
There are currently NO regulations in place to say what may or may not be charged by a healthcare practitioner. However this does not mean that we can charge exorbitant fees. A clinician's fees should be fair, and represent his qualifications, experience and the costs of his/her overheads. As healthcare practitioners we should always act in our patient's best interest, and aim to treat our patients like we would like to be treated.
Good Practice Guidelines:
• Practitioners should give every patient a full cost estimate -before treatment begins. This could be orally, but should preferably be in writing and kept in the patients records. The cost estimate should be presented in a way the patient understands, and include a value in Rand and cents. A situation of "my word against yours" should be avoided where possible. This should be done even if medical aid rates are charged, or if the treatment would be claimed directly from the medical aid.
• Any written estimate agreements to be signed by the patient should be tailored to the patient and specific to the treatment the patient will receive.
• If there is likely to be more than one treatment required, you should provide the patient with a full cost estimate for each treatment that will be undertaken.
• The patient should also be informed; that should there be any short-falls in the amount paid by the medical scheme in relation to the costs of treatment it will be the patient who will be responsible for the remainder of the costs.
• You should make sure that the patient fully understands the costs and their responsibility towards payment. This could be achieved by asking the patient to provide you with a verbal summary of their understanding from the information you have provided them.
• You should make sure that you have recorded your conversation with the patient regarding costs of treatment in your records. This will assist in showing that you have been able to obtain the patients informed consent.
• Never make assumptions about the patient's ability, or willingness to pay for treatment. Patients are real people, with real problems including financial ones, and they would naturally be reluctant to discuss this with a third party.
• You should inform your patient if there will be any third parties costs involved in their treatment (such as laboratory fees). If this will be the case you should provide the patient with full information of who will provide the treatment and what costs they should expect to receive.
• If any discrepancies occur between the fees the patient thought they would be charged and the final account, this should be addressed pro-actively in a discussion, rather than presume the patient will understand without an explanation. Most of our patients value our services however the right to know about the cost of treatment is now enshrined in law and we all have an ethical duty to discuss costs just as much as the clinical detail.
• Before chasing any outstanding accounts, always check if the patient is satisfied with the treatment you provided. It makes sense to approach unpaid accounts in a non- confrontational way. Any confrontation regarding outstanding fees will naturally invite complaints about the quality of the treatment provided. Warning - Do not assume that every patient who expresses dissatisfaction is trying to avoid payment.
• Practitioners should refrain from taking the responsibility to communicate with the medical aids on behalf of their patients. Neither should they provide guarantees, or expectations that the medical aid would cover the cost of the proposed treatment plan.
• Each member of the team should be trained specifically in dealing sensitively with fee collection. Always respect the patient's privacy, and dignity. Collecting outstanding debts can be very challenging yet has become a critical business skill. If done correctly it increases profitability, saves time, and prevent the likelihood of complaints arising.
• Take clinical decisions based on the patient's best interest, and not considering the financial restrictions placed by the patients' medical aid.
