










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.70 n.6 Johannesburg Jul. 2015
CLINICAL WINDOW
What's new for the clinician? Summaries of and excerpts from recently published papers
V Yengopal
MChD (Community Dentistry) Stellenbosch. Department of Community Dentistry, School of Oral Health Sciences, University of the Witwatersrand. E-mail: \/eerasamyYengopal@wits.ac.za
1. Toothbrushing and flossing behaviour in young adults -a video observation
Winterfeld T, Schlueter N, Harnacke D, Wig J, Margraf-Stiksrud J, Deinzer R , Ganss C. Toothbrushing and flossing behaviour in young adults-a video observation. clin oral Investigations 2015; 19: 851-858.
Oral hygiene is a cornerstone of maintaining gingival and dental health, provided that the removal of plaque is sufficiently thorough. Despite the intensive efforts made in many settings to establish good oral hygiene performance, self-performed mechanical plaque removal often is not sufficiently effective, and clinicians observe daily that patients exhibit considerable amounts of plaque, even though these patients report performing oral hygiene routines. The cause of this discouraging finding is not well understood. The performance of oral hygiene procedures has been primarily investigated using levels of plaque as a surrogate parameter but was rarely verified by observational data, for instance, video filming.
Amongst the few observational studies of toothbrushing behaviour, it was noted that the time spent on brushing various areas of the mouth varied considerably and that the oral surfaces were rarely brushed. Subjects used more than one type of stroke, frequently alternated between brushed areas of the mouth, and often tended to move the toothbrush from the left to the right. These findings clearly show a marked difference between the recommendations for adequate toothbrushing (in particular, brushing systematically) and what was implemented in daily practice. These studies were published more than two decades ago and have not been repeated since.1 Winterfeld and colleagues (2015)1 reported on a study that sought to collect information about oral hygiene practice by observing and analysing habitual brushing and flossing.
MATERIALS AND METHODS
This German-based study was a descriptive, cross-sectional, non-disguised observational study. Participants were inhabitants of Giessen (Hesse, Germany) and of the same age. From the register of residents, a random sample of subjects was drawn, aiming to obtain a final sample of 100 subjects. Included subjects were all born in 1992, in good general health (no mental or physical disability with the potential to influence oral hygiene), used a manual toothbrush and provided informed consent.
All procedures and conversations (e.g. telephone script, welcome/information/inclusion and explanation of video procedures) were standardised. The study was carried out by two investigators, who were trained and calibrated.
Participants performed their habitual oral hygiene in a separate prepared room (simulation of a washbasin bathroom) while standing in front of a parabolic mirror with an integrated video camera. A toothbrush with a short brushing head and medium bristle stiffness and floss that was 0.5 m long was offered, and participants were invited to clean their teeth as they did habitually in everyday life. They were left alone in the room, but they were aware of being filmed. There was no clock provided and no time restriction; toothpaste was not provided to simplify the analysis of the video.
The video recordings were analysed after data collection was complete using the observation software INTERACT. A count coding system for measuring continuous timed events was developed after several rounds of discussion with all persons involved in the project. Videos were coded exhaustively, meaning that every second of the observation session was coded using continuous timed-event behaviour sampling. Videos were coded in four passes as follows: In the first pass, the time of the start and stop of the brushing process were determined; in the second pass, the areas where the teeth were brushed were determined; and in the third pass, the types of brushing strokes were coded. A fourth pass of coding was performed if the participant flossed.
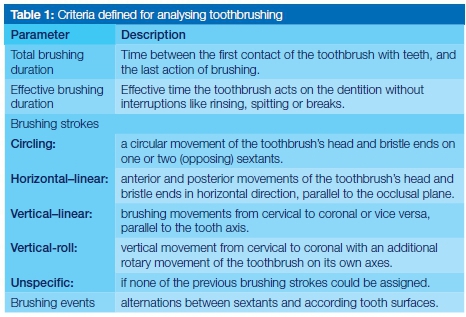
Basic characteristics of interest were brushing duration and the types of brushing strokes. More in-depth analysis focused on patterns of movements within the dentition, including the frequency of alternations between sextants and tooth surfaces. The dentition was divided into sextants (S1-S6) and three tooth surfaces (oral, occlusal and vestibular) that summed to 18 areas.
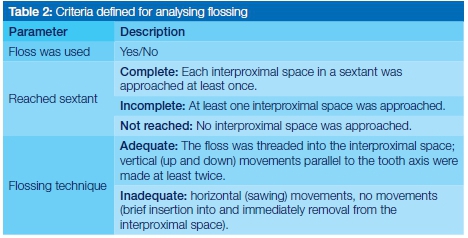
Measures of interest regarding flossing were whether subjects flossed, their flossing technique and the completeness of flossing interproximal spaces. The parameters used to analyse toothbrushing and flossing are described in Tables 1 and 2.
Intra-rater agreement was calculated in INTERACT, which offers the possibility to compare timed-event sequential data of multiple observers based on the kappa statistic.
RESULTS
Participants included 58 females and 43 males with a mean age of 18.9 ± 0.3 years. The overall response rate was 42%.
The mean total brushing duration was 162.5 ± 73.9s. The effective brushing duration was 156.0 ± 71.1s; 63 % of the participants brushed for 2min or longer, and only 14% brushed less than 1.5min.
The effective brushing duration in the upper jaw was 75.9 ± 35.4s and, in the lower jaw, was 80.2 ± 38.3s (p < 0.05). The right side was brushed for 52.0 ± 26.0s, the left side for 48.8 ± 26.0s, and the anterior area for 55.3 ± 29.0s (p>0.05). Handedness had no significant impact. The vestibular surfaces were brushed more than twice as long (72.1 ± 31.8s) as the oral surfaces (27.1 ± 27.8s) (p < 0.001).
Concerning completeness of brushing, except for the occlusal tooth surfaces, 26 participants reached all 12 areas of the dentition (the oral and vestibular surfaces of S1-S6), 36 brushed between 9 and 11 areas, and 39 brushed less than 9 areas.
Circular and horizontal strokes were predominant on the vestibular surfaces, whereas the oral surfaces were predominantly brushed with horizontal strokes in the posterior sextants and with vertical strokes in the anterior sextants
Participants moved frequently between areas (45.1 ± 22.4 brushing events; upper tercile range was between 50 and 133 brushing events). The most frequent alternations between sextants occurred within a jaw. In the upper jaw, movements often changed from posterior to anterior and vice versa whereas, in the lower jaw, changes often occurred between the posterior sextants and did not include the anterior area. Diagonal alternations or alternations between jaws were observed much less often; there was a frequency peak for movements between S6 and S1.
The alternations from one area to another were most frequently from (I) the anterior vestibular area to the left and right vestibular area; (II) from the left and right vestibular area to the anterior vestibular area and (III) from the right occlusal to the left occlusal and vice versa.
Almost half of the participants (n = 47) flossed. The flossing performance of five participants was not completely visible in the video recording. Of the remaining 42 participants, only five flossed all sextants completely; 26 flossed between one and five sextants completely, and 11 flossed only sporadically.
In the upper jaw, the anterior teeth were flossed completely more often (S2: 21 participants) than were the posterior teeth (S1: 12 participants; S3: 12 participants); this difference was not observed in the lower jaw (S4: 18 participants; S5: 18 participants; S6: 19 participants).
Two participants performed an adequate (see Table 2) flossing technique, whereas the others (n = 40) used an inadequate flossing technique.
Only one participant flossed all sextants completely and performed the technique defined as adequate.
CONCLUSION
The authors concluded that although the toothbrushing duration of young adults complied with international recommendations, toothbrushing was not complete in many subjects, and there was a striking neglect of the oral surfaces. Although circular and horizontal movements were used most often, there was intra-individual heterogeneity in the types of strokes at different areas of the dentition.
Subjects brushed with specific recurrent motion sequences that were very similar to those observed in studies published more than 30 years ago, indicating a strongly anchored brushing behaviour independent of oral hygiene education and socio-demographic background. Flossing was performed by almost half of the participants; however, only two subjects flossed according to the technique we defined as adequate, and only one of them flossed completely.
IMPLICATIONS FOR PRACTICE
These findings suggest that oral health professionals should continue to highlight the importance of proper oral hygiene instruction in their patients and demonstrate and monitor patient compliance to brushing and flossing protocols.
Reference
2. Comparison between Neocone®, Alvogyl® and Zinc Oxide Eugenol packing for the treatment of Dry Socket: A RCT
Faizel S, Thomas S, Yuvaraj V, Prabhu S, Tripathi G. comparison Between Neocone, Alvogyl and Zinc oxide Eugenol Packing for the Treatment of Dry Socket: A Double blind Randomised control Trial. J Maxillofacial & oral Surgery 2015; 14: 3120320.
Alvoelar osteitis (AO), more commonly referred to as "Dry Socket", is a painful debilitating condition that occurs as a complication of tooth extraction in the permanent dentition. There appears to be no consensus on the criteria used to determine the diagnosis of AO and thus the wide range (1-30%) in the rate of incidence reported in published papers and reviews must be viewed with caution. Generally, though, the signs and symptoms usually occur 1-3 days following an extraction and include features such as postoperative pain [unrelieved by analgesics] in and around the extraction site, a partially or totally disintegrated blood clot within the alveolar socket, halitosis, necrotic debris, etc.1 Dry socket has a multifactorial etiology, which can be divided into general factors such as age, sex, decreased body resistance due to systemic disease, nutritional deficiency, etc., and local factors such as anatomical location, traumatic surgery, smoking, fibrinolysis of clot, local circulation, local anesthesia, and vasoconstrictors.1 Since dry socket is the most common post extraction complication, many researchers have attempted to find a successful method for its prevention. Systemic antibiotics, topical antibiotics, chlorhexidine, para-hydroxybenzoic acid, tranexemic acid, polylactic acid, steroids, eugenol containing dressings, lavage, 9-aminoacridine, etc., have been proposed to assist in the prevention of dry socket.1 However, this area remains controversial as no single method has gained universal acceptance.
The management of dry socket is as controversial as its aetiology and prevention. Different medicaments and carrier systems are commercially available with little scientific evidence to guide a selection process for their use. Faizel and colleagues (2015)1 reported on a trial that sought to assess the relative efficacy of different dressings for the management of pain and promotion of healing in AO.
MATERIALS AND METHoDS
This study was conducted among patients who reported for dental extraction at the Department of Oral and Maxillofacial Surgery, Peoples College of Dental Sciences and Research Centre, Bhopal, India. Exclusion criteria included conditions such as pregnancy, history of radiotherapy, and coexisting cellulitis/fascial space infections.
Patients who reported with pain after tooth extraction were evaluated to ascertain the cause for this complaint. Diagnosis of AO was clinically established on the basis of the following features by a blinded assessor: (1) Pain in and around the extraction socket with or without radiation that increased in severity for some period from 1 and 3 days after extraction; (2) Partial or total clot loss in the interior of the alveolus with or without halitosis.
Any other associated findings such as halitosis, lymphadenopathy, etc., were also recorded. Patients were randomly assigned using a randomization table to one of the three groups A, B, and C in order to receive treatment for AO. Patients within these groups were managed as follows: Group A: Alvogyl®. (content: iodoform 15.8gm, eugenol B.P. 13.7gm, and butamben 25.7gm). A few fibers of Alvogyl® were placed with the help of a sterile instrument deep into the socket ensuring that the denuded bone was completely covered followed by the placement of sterile gauze. The gauze was removed after 5min.
Group B: Zinc Oxide Eugenol (ZOE). A piece of gauze soaked with freshly prepared ZOE paste was placed in the extraction socket under aseptic conditions.
Group C: Management of dry socket by Neocone®. (Content- polymyxine B sulfate, tyrothricin, neomycin sulfate, tetracaine hydrochloride). A single pellet of Neocone® was placed inside the socket followed by the placement of a piece of sterile gauze to cover the socket. The gauze was removed after 5 min.
The infected socket in all patients was irrigated with warm sterile saline solution. Curettage was avoided. Loose debris was removed, taking care to avoid dislodging any residual clot present in the socket.
The pain levels were assessed on the basis of Wong Baker Visual Analogue Scale after 5min, 30 min, 1h, day 1, day 2, day 3, day 5, day 7, and day 10 after placement of the medicament. The dressings were evaluated by a blinded assessor at every follow-up visit and were changed in case of persistence of pain. No further dressings were done if the patients had sustained pain relief for more than 48 h.
Clinical examinations for the signs of healing of dry socket were performed on 1st, 3rd, 5th, 7th, and 10th day by a blinded assessor. Persistence of parameters such as empty socket, bare bone, and erythema around the socket were noted after removal of the pack. For assessment of pain relief as well as healing, the patients were followed up on a daily basis if signs and symptoms persisted beyond 10 days.
RESULTS
A total of 7,106 teeth were extracted during the study period, of which 3,097 (43.59%) were extracted in males and 4,009 (56.41%) in females. 105 patients (1.64%) returned with signs and symptoms of dry socket in a total of 117 extractions. Of these, 69 (2.22%) dry sockets were noted in females and 48 (1.19%) dry sockets in males (male to female ratio was 1.86; P = 0.0008)
The patients in this series were divided into seven age groups. Mean age of the patients was 34.6 years. The highest incidence of dry socket was seen in the age group of 21-40 years; P < 0.0001).
Pain was present in 117 (100%) cases, empty socket was present in 57 (48.71%), bare bone (partially denuded socket) was present in 53 (45.20%), halitosis in 61 (52.10%), and redness around socket was found in 45 (38.60%) cases. The time for onset of dry socket was calculated from the time lag between extraction and onset of pain. The analysis of data revealed that the largest number of cases [55 (47.10%)] had an onset on the third day after extraction. In 22 (18.80%) cases, symptoms manifested on the 2nd day, while 24 (20.51%) cases noted symptoms on the fourth day. Sixteen cases had an onset on the fifth day after extraction. Mean time for onset of the complication was 3.2 days. Teeth were grouped into anatomical sites for the purpose of analysing dry socket distribution. Higher incidence of dry socket was found in the lower jaw (63.24%), as compared with the upper jaw (36.75%; P < 0.05).
Highest incidence of dry socket in mandibular arch was seen in the third molar region (6.91%). The highest incidence in maxillary arch occurred in the second molar region (1.97%). It was observed that the incidence of dry socket in patients who underwent single tooth extraction was much higher than those who underwent multiple extractions (single extraction to multiple extraction ratio was 4.4:1(P < 0.05).
The incidence of dry socket was found to be higher in cases of trans-alveolar extraction than in intra-alveolar extraction (trans-alveolar extraction to intra-alveolar extraction ratio was 8.36:1( P < 0.0001)
When the reasons for extraction of teeth were analysed and correlated with incidence of dry socket, it was apparent that the highest incidence was noted in teeth which were extracted for recurrent pericoronitis (13.9%), while the lowest incidence was noted in patients who underwent pre-prosthetic extractions (0.75%).
Of the 7,106 extractions, 1,020 were performed in patients with medical comorbidities including those on oral contraceptives and 6,086 extractions were performed in otherwise healthy individuals. The incidence of dry socket in the former set of patients 57 (5.58%) was higher than the latter 60 (0.98%). Among the patients with coexisting medically compromised states, higher incidence was noted in asthmatics (4/19 extractions), hypertensives (12/389 extractions), and those consuming oral contraceptive pills (14/110 extractions). These differences were again statistically significant.
A total of 1,085 teeth were extracted in smokers. The number of dry sockets in this subset was 30, an incidence of 2.76%. A total of 6,021 teeth were extracted in non-smokers. This subset had 87 dry sockets, an incidence of 1.44 %. The difference was statistically significant (P=0.02)].
Out of 7,106 teeth, 1,540 teeth were extracted in patients with good oral hygiene. The number of dry sockets in these patients was 9, an incidence of 0.58%. A total of 2,156 teeth were extracted in patients having fair oral hygiene; 31 dry sockets were encountered, an incidence of 1.43%. A total of 3,310 teeth were extracted in patients with poor oral hygiene. The incidence of dry socket was 2.32% (77 dry sockets).
The mean time to obtain initial pain relief with Alvogyl®, Neocone®, and ZOE were 7.35, 17.23, and 25.02min respectively (i.e., Alvogyl® < Neocone® < ZOE pack). The difference in initial pain relief between all three groups was statically significant (P<0.0001). Results suggest that Alvogyl® is superior to the other two medicaments for providing initial pain relief.
The mean times for complete pain relief with Alvogyl®, ZOE, and Neocone® were 6.47, 8.64, and 4.85 days, respectively (i.e., Neocone® < Alvogyl® < ZOE). The difference in complete pain relief between all three groups was statistically significant (P < 0.0001).
The baseline clinical examination prior to initiation of treatment revealed severe pain in all patients (n=117; 100%). Other signs and symptoms included halitosis (n=61, 52.10%), empty socket, i.e., completely denuded socket (n=57, 47.50%), bare bone, i.e., partially denuded socket (n=53, 45.20%), and redness around socket (n=45, 38.60%).
Out of 117 sockets with AO, 57 presented with empty sockets. Numbers of sockets treated for this sign with Alvogyl®, ZOE, and Neocone®, were 19, 18, and 20, respectively. Of the 19 sockets treated with Alvogyl®, 12 (63.15%) remained empty on the third day of follow up with 100% resolution on the tenth day. Of the 18 sockets treated with ZOE, significant reduction was noted only on the fifth day with 100% resolution on the eleventh day. Of the 20 sockets treated with Neocone®, eight (40%) remained empty on the third day of follow up with 100% resolution on the seventh day of follow up. The complete disappearance of this sign was therefore fastest with Neocone® and slowest with ZOE.
Out of 117 sockets with AO, 53 presented with bare bone. Numbers of sockets treated for this sign with Alvogyl®, ZOE, and Neocone®, were 19, 16, and 18, respectively. Of the 19 sockets treated with Alvogyl®, only ten (52.63%) still showed bare bone on the third day of follow up with 100% resolution on the tenth day of follow up. Of the 16 sockets treated with ZOE, twelve (75%) still exhibited bare bone on the third day of follow up with 100% resolution on the twefth day of follow up. Of the 18 sockets treated with Neocone®, only seven (38.89%) were noted to have persistent bare bone on the third ay of follow up, with 100% resolution on the fifth day of follow up. The resolution of this sign was fastest with Neocone® and slowest with ZOE
Of the 117 sockets with AO, 57 had redness around the socket. The numbers of sockets treated for this sign with Alvogyl®, ZOE, and Neocone® were 16, 14, and 15, respectively. Of the 16 sockets treated with Alvogyl®, ten (62.5%) continued to show redness around the socket on the third day with 100% resolution on the tenth day. Of the 14 sockets treated with ZOE, twelve (85.71%) still had persistent sign on the third day of follow up with 100% resolution on the tenth day. Of the 15 sockets treated with Neocone®, only seven (46.67%) had persistent redness around the socket on the third day of follow up. All three products had 100% resolution on the tenth day.
CONCLUSIONS
The authors concluded that:
- Neocone® emerged as the most suitable dressing material for the management of dry socket by virtue of shorter time required for complete pain relief, fewer visits for dressing change, and faster clinical healing of the socket. Onset of pain relief with Alvogyl® was faster but not sustained. ZOE was most cost effective and easily available medicament for dressing. Intervention is preferably initiated immediately upon diagnosis. While all the three tested medicaments showed positive outcomes, Neocone® required the least replacement and was quicker in providing lasting pain relief. It may therefore be advantageous to use Neocone® dressings to facilitate faster recovery. To the patients, this may translate into earlier return to work and productivity.
- Alveolar osteitis is more likely in young adults, females, smokers, patients with medical co-morbitities, particularly asthmatics, and patients with poor oral hygiene and local infection such as pericoronitis. The likelihood is also higher in the mandibular molar region, particularly after trans-alveolar extractions and after singleton extraction rather than multiple. It is unclear whether these factors contribute to the risk independently or collectively. Further studies are required to clarify this aspect in order to implement effective preventive strategy.
IMPLICATIONS FOR PRACTICE
Whilst Alvogyl® was found to be superior to the other two medicaments in providing initial pain relief, Neocone® clearly shows superior, longer lasting pain relief and healing potential as evidenced by improvement in clinical signs.
ACRONYMS
AO: Alvoelar osteitis
ZOE: Zinc Oxide Eugenol
Reference
1. Faizel S, Thomas S, Yuvaraj V, Prabhu S, Tripathi G. Comparison Between Neocone, Alvogyl and Zinc Oxide Eugenol Packing for the Treatment of Dry Socket: A Double Blind Randomised Control Trial. J Maxillofacial & Oral Surgery 2015; 14: 3120320. [ Links ]
1. Winterfeld T, Schlueter N, Harnacke D, Illig J, Margraf-Stiksrud J, Deinzer R, Ganss C. Toothbrushing and flossing behaviour in young adults-a video observation. Clin Oral Investigations 2015; 19: 851-858. [ Links ]
