










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.70 n.6 Johannesburg Jul. 2015
CASE REPORT
A tongue ring barbell shank in the floor of the mouth: An incidental finding by panoramic and cephalometric radiographs - a case report and review of literature
NP Zwane
BDS (Medunsa). Lecturer in Department of Prosthodontics: Sefako Makgatho Health Sciences University. Tel: 012 521 4871. E-mail: zodwa.zwane@smu.ac.za
INTRODUCTION
Body adornment in the form of piercing has increased in popularity especially amongst young people in westernised societies.1 Body piercing has a long history with the most pierced areas being the navel, lip, tongue, earlobe, eyebrows and genitalia. Health professionals are likely to see an increase in complications of these piercings as their popularity increases.2,3
Piercing of the tongue is usually performed in the midline of the tongue anterior to lingual frenum. A barbell shank of about 1.8cm must be placed first in the tongue to accommodate the initial swelling that normally occurs after piercing. This is then followed by the insertion of a shorter barbell shank after healing. The procedure is usually performed without anaesthesia. The tongue is protruded using a clamp and is then pierced by a needle bearing a gauge equal to that of the barbell stem.4,5
CASE REPORT
A 20 year old female presented at the MEDUNSA Oral Health Centre with complaints of malocclusion. Her medical history was uneventful, but on her dental history she indicated that she had "braces" at the age of 12 and whilst eating an apple the braces had come out and she had never attended for follow-up. She then later confirmed that it was a maxillary Hawley appliance that she had and that it had broken in less than a year. Lateral cephalom-etric examination revealed a radiologically- dense rod-like structure superimposed on the roots of tooth 45. The soft tissue location in the tongue and floor of mouth was confirmed on panoramic view. A hard object was palpated in the sublingual area directly behind the lingual frenum and was too thick and straight to have been an orthodontic wire from a broken Hawley appliance. The patient initially denied knowledge of the object but later admitted to a failed tongue piercing procedure. She finally admitted to having gone to the tongue piercing parlour where an unsuccessful attempt had been made to pierce her tongue.
DISCUSSION
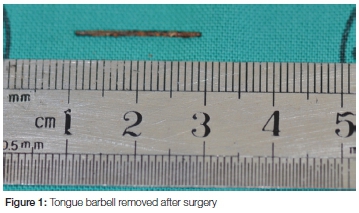
Tongue piercing complications are categorised as acute or chronic.6 Acute complications include tongue swelling, pain, changes of speech and foreign material rejection especially if the metals used contain nickel.7,8 Less frequently experienced symptoms include generation of a galvanic current between barbell and metallic dental restorations,9 infection, airway obstruction due to trauma and obstruction of the airway by the jewellery as well as prolonged hemorrhage.10,11,12 In our case the rod was an incidental finding on routine radiographs and was not the source of the patient's main complaint. The metal was found on the sublingual folds just behind the lingual frenum, and had projected a ghost image on the radiographs. The patient was referred for surgical excision of the foreign object which consisted of a metal rod about 2cm in length, surrounded by fibrotic tissue (Figure 1).
Chronic complications of tongue piercing include trauma to the teeth, trauma to the gingiva and localised tissue overgrowth.9,12,13 There have been a few similar reports on jewellery becoming embedded in the oral soft tissues of the patients.13
CONCLUSION
Strict follow up is essential of any strange and unexplained objects that are found coincidentally through radiographic examination during dental treatment.
Conflict of interest: None declared.
References
1. Folz BJ, Lippert BM, Kuelkens C, WernerJA. Hazards of piercing and facial body art: a report of three patients and literature review. Ann Plast Surg. 2000; 45:374-381. doi: 10.1097/00000637-200045040-00004. [ Links ]
2. Tweeten SM, Rickman LS. Infectious complications of body piercings. Clin Infect Dis. (1998) 26 (3): 735-740. doi:10.1086/514586. [ Links ]
3. Armstrong ML. Body piercing: what practicing RNs should know. Texas Nursing 1996; 70:8-10. [ Links ]
4. Farah CS, Harmon DM. Tongue piercing: Case report and review of current practice. Australian Dental Journal 1998; 43 :( 6):387-9. [ Links ]
5. Botchway C, Kuc I. Tongue piercing and associated tooth fracture. Jnl Can Dent Assoc. 1998;64(11):803-5. [ Links ]
6. Campbell A, Moore A, Williams E, Stephens J, Tatakis DN. Tongue piercing: Impact of time and barbell stem length on lingual gingival recession and tooth chipping. J Perio 2002; 73: 289-97. [ Links ]
7. Reichl RB, Dailey JC. Intraoral body piercing: a case report. Gen Dent 1996; 44: 346-7. [ Links ]
8. Armstrong ML. You pierced what? Ped Nurs, 1996; 22: 236-8. [ Links ]
9. De Moor RJG, De Witte AMJC, De Bruyne MAA. Tongue piercing and associated oral and dental complications. Endo Dent Trauma 2000; 16: 232-7. [ Links ]
10. Meltzer DI. Complications of body piercing. Am Fam Physician. 2005 Nov 15; 72(10):2029-34. [ Links ]
11. Ziebolz D, Hildebrand A, Proff P, Rinke S, Hornecker E Mausberg RF. Long-term effects of tongue piercing, Clin Oral Investig. Feb 2012; 16(1): 231-7. Published online Jan 27, 2011. doi: 10.1007/s00784-011-0510-6 [ Links ]
12. Hardee PSGF, Mallya LR, Hutchinson IL. Tongue piercing resulting in hypotensive collapse. Br Dent J 2000; 188: 657-8. [ Links ]
13. Theodossy TA. Complication of tongue piercing: A case report and review of the literature. Br Dent J 2003; 194: 551-2. [ Links ]
