










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.70 n.5 Johannesburg Jun. 2015
RESEARCH
The need for physiotherapy intervention for mandibular condyle fracture patients: A needs analysis
A van der MerweI; R BarnesII
IBSc Physiotherapy (Stell), MSc Physiotherapy (UFS). Lecturer, Department of Physiotherapy, University of the Free State
IIBSc Physiotherapy (UFS), MSc Physiotherapy (UFS). Department Head, Department of Physiotherapy, University of the Free State
ABSTRACT
INTRODUCTION: The need for physiotherapy intervention in the treatment of mandibular condyle fractures has been highlighted in international research but no such study has been conducted in South Africa.
AIMS AND OBJECTIVES: To perform a needs analysis amongst academically affiliated maxillo-facial surgeons and physiotherapists in South Africa regarding their perceived need for a post-operative physiotherapy intervention program for patients who sustained mandibular condyle fractures.
DESIGN: Quantitative, non-experimental study, by means of a needs analysis questionnaire.
METHODS: The questionnaire was distributed to qualified experts: one physiotherapist and one maxillo-facial surgeon from each of the South African training institutions. A convenience sampling method was used to select appropriately trained participants.
RESULTS: The sample of participants was unanimous in confirming that there was a definite need for a physiotherapy intervention for mandibular condyle fracture patients whilst 85.7 % of respondents indicated that the patients should receive hospital physiotherapy.
CONCLUSIONS: Experts in the field recommended that physiotherapists should provide post-operative rehabilitative therapy to patients who had sustained mandibular condyle fractures to enhance the rehabilitation process. The data obtained from the needs analysis will be applied, using the Delphi method to develop a post-operative functional exercise programme for patients who had sustained these fractures.
Key words: mandibular condyle fractures; physiotherapy; exercise; temporomandibular joint; needs analysis
INTRODUCTION
Maxillofacial trauma represents a costly socio-medical problem, as it affects a considerable number of trauma patients.1
Previous South African studies conducted by maxillo-facial surgeons have recorded a high prevalence of facial fractures.2,3 The mandible is mostly affected, with injuries resulting from high-velocity impact, such as interpersonal assaults (86.5%), or a road traffic accident (13.5%), resulting in fractures.2,5,6 Rikhotso and Ferretti (2008) stated that condylar fractures accounted for up to 57 % of all man-dibular fractures.3
The oldest treatment protocol for mandibular fractures is closed reduction and internal fixation and the procedure was the preferred treatment by maxillofacial surgeons.7,8 Currently, however, open reduction and internal fixation (ORIF) surgery is becoming the main treatment of choice for mandibular fractures, with an average of 182.6 ORIF's being done per annum in a Johannesburg Public Hospital setting.2,6
Complications can and do occur with treatment of mandibular fractures, during any of the treatment phases,9 and can include periodontal problems, facial pain, tension in masticatory musculature, poor chewing function, chin deviation, limited mouth opening as well as malocclusion, which in the long run may influence the quality of life of the patient.10,11,12 A large number of studies have found that an ideal prognosis for oral function cannot be obtained without the appropriate post-surgical functional exercises.3,6,101614 Active and passive joint exercises for increasing the range of motion of the TMJ is regarded as a key component in the post-surgical management of these patients, and long-term follow-up is recommended.15 Positive effects of exercise and manual therapy were reported in the systematic review undertaken by McNeely et al (2006), validating the contribution made by physiotherapists in the rehabilitation of patients who sustained mandibular condyle fractures.16
No research has been conducted in South Africa regarding the need for post-operative physiotherapy intervention for patients who sustained mandibular condyle fractures. The aim of this study was therefore to perform a needs analysis amongst academically affiliated South African physiotherapists and maxillo-facial surgeons to determine the perceived need for a post-operative physiotherapy intervention program for patients with mandibular condyle fracture. This study will serve as a baseline for a further Delphi project in compiling a recommended physiotherapeutic intervention programme for this patient population.
METHODS
Study design
This was a quantitative, non-experimental study, performed by means of a needs analysis questionnaire.
Participants
As this study explored a relatively new area for physiotherapy research, a convenience sampling method was used to select appropriately trained participants for the needs analysis. Sampling focused on academic institutions providing training in physiotherapy and/ or maxillo-facial surgery, as individuals in these programmes would have the appropriate training and knowledge equipping them to participate.
The needs analysis consisted of 11 participants: four qualified maxillo-facial surgeons, one from each of the training institutions in South Africa; and seven physiotherapists representing seven of the eight South African physiotherapy training institutions. Physiotherapy participants had to have completed post-graduate training in Orthopaedic Manipulative Physical Therapy (OMPT). One South African physiotherapy training institution did not provide or nominate a suitable participant representative of their institution.
Ethical considerations
Ethical clearance was obtained from the Ethics Committee of the Faculty of Health Sciences of the University of the Free State (ECUFS NR 05/2012). Informed consent was obtained from each participant before completion of the needs analysis questionnaire. Confidentiality of all collected information was ensured as the questionnaire did not require that the participant state his/her name or put any identifiable data on the questionnaire.
Procedure
The needs analysis questionnaire was formulated to obtain the maximum amount of information from participants regarding their treatment, or proposed treatment, for patients who had sustained mandibular condyle fractures. Open-ended and closed questions were posed to participants. The questions were formulated after conducting an extensive literature search and using personal information gained from communication with maxillo-facial surgeons. The face validity of the study was enhanced by piloting the needs analysis questionnaire before it was sent to the participants. Piloting was done by two experts in the field, one physiotherapist and one maxillo-facial surgeon, to ensure that the study objectives were met by the questionnaire. Demographic data was collected in order to describe the participants of the study population.
SurveyMonkey™, an online research tool, was used to electronically send the needs analysis questionnaire to the eleven participants.
Statistical analysis
SurveyMonkey™ reported all results in a percentage. For each question there was an indication of how many participants answered or omitted questions, as well as a full report of any comments made by participants regarding each question. The results for each question, portrayed as a percentage, were analysed by the researcher.
Responses to the open-ended questions were tabulated and used to compile possible answer options for a Delphi study which was conducted after completion of the needs analysis.
RESULTS
Demographics and response rate
Eight participants (73%), two maxillo-facial surgeons and six physiotherapists, completed the needs analysis questionnaire.
Only twenty seven percent of the participants currently treat mandibular condyle fracture patients in-hospital, with 13% of participants providing out-patient treatment. These disclosures resulted in questions regarding physiotherapeutic treatment techniques, precautionary measures to be considered and the incidence of reported functional loss by mandibular condyle fracture patients to remain unanswered by many participants.
Proposed need for physiotherapy intervention for mandibular condyle fracture patients
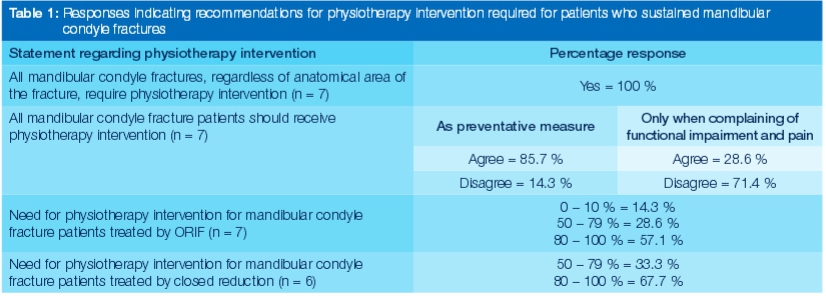
Results tabulated in Table 1 indicated that participants all agreed that (regardless of the anatomical area of the con-dyle fractured) all mandibular condyle fracture patients should receive physiotherapy intervention. All participants unanimously agreed that there is a need for physiotherapy intervention for in-hospital patients who had sustained mandibular condyle fractures. As illustrated by the needs analysis results, physiotherapy intervention should not only be given when patients complain of functional impairment and pain, but as a routine preventative measure. Participants are of the opinion that patients receiving post-operative physiothera-peutic intervention would recover quicker and may present with less functional limitations compared with those patients receiving no physiotherapy intervention.
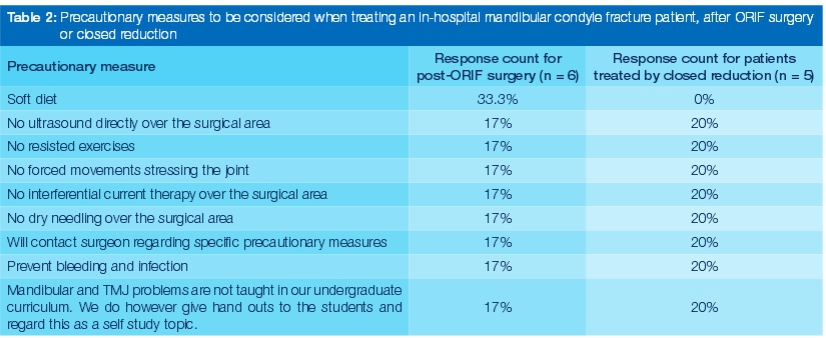
The open-ended questions regarding possible post-ORIF and closed reduction pre-cautionary measures, and the duration of these precautionary measures, elicited a variety of responses from participants. For mandibular con-dyle fracture patients who underwent either ORIF surgery or closed reduction, it was deemed safe by participants to administer the treatment modalities tabulated in Table 2. It was found that participant responses indicated a recommendation for precautionary measures to be administered for two (20%) or six (40%) weeks when managing mandibular condyle fracture patients treated by ORIF surgery, and two (40%) or three (20%) weeks for those treated by closed reduction.
Treatment modalities listed by participants for mandibu-lar condyle fracture patients following ORIF surgery and closed reduction included active jaw exercises, isometric jaw exercises, cervical postural advice, ultrasound therapy, Transcutaneous Electrical Stimulation, cryotherapy and facial massage.
Active jaw exercises were recommended by only a few participants (29% post-ORIF surgery, and 40% after closed reduction) as a treatment intervention. One of the participants (a maxillo-facial surgeon) commented that active jaw movements, within the limits of pain, would without a doubt be required by patients treated by either ORIF surgery or closed reduction for mandibular condyle fractures.
Forty two percent of participants felt that passive accessory TMJ mobilisation was adequate and safe to perform one day after ORIF surgery. The concerns raised by physiotherapy participants regarding the in-hospital use of passive accessory TMJ mobilisation may indicate that the definition of passive joint mobilisations, included in the question, might not have been clear enough to convey the exact anatomical joint movement to be executed by the physiotherapist.
The participants identified symptoms which may be experienced by patients and which warranted physiothera-peutic intervention, if the patients were not already being seen routinely by a physiotherapist. These included: TMJ joint stiffness (100%), TMJ pain (85.7%), loss of function regarding speech and chewing (85.7%), incorrect jaw movements (85.7%), and facial muscle pain (71.4%).
DISCUSSION
Rikhotso and Ferretti's research (2008) emphasised the need for appropriate physiotherapy treatment for mandib-ular condyle fracture patients to aid healing and to achieve more favourable post-surgical results.3 The results of the current needs analysis questionnaire also clearly indicates that there is a recommended requirement for post-operative physiotherapy intervention in the treatment of these patients, treated by either ORIF surgery or closed reduction. Post-operative rehabilitation would have the benefit of enhancing the recovery and rehabilitation process.
The majority of participants indicated that physiotherapy intervention should not only be provided when patients complain of functional impairment and pain, but as a routine preventative measure.
The response rate for the needs analysis, 73%, was well within the acceptable parameters set by previous questionnaire based studies.17-20 However, only 27% of the participants currently treat patients who have sustained mandibu-lar condyle fractures, resulting in uncertainty in answering some of the questions regarding physiotherapeutic treatment techniques, precautionary measures to be considered and the incidence of reported functional loss.
As highlighted by one participant, the uncertainty regarding the answering of questions could have been due to the fact that every mandibular condyle fracture patient presents and is treated differently, and some participants might have felt uncomfortable to generalise when providing answers. However, due to the specific inclusion criteria, all respondents had received training and knowledge sufficient to provide opinions regarding the treatment and the precautionary measures and their duration, which should be considered, when treating mandibular condyle fracture patients. Variation in management policies does emphasise that an open channel of communication between the surgeon and physiotherapist is of the utmost importance in establishing the most beneficial physiotherapy treatment programme for each individual patient.14, 21
The results obtained through the needs analysis have since been used to compile a Delphi questionnaire in order to develop proposals for a post-operative physiotherapy intervention programme for mandibular condyle fracture patients.
CONCLUSION
The study results confirmed that, according to expert opinion, adequate and prompt post-operative physiotherapeutic intervention for patients who sustained mandibular condyle fractures is important to achieve more favourable post-surgical results. The study provided a platform for expanding the evidence-base for physiotherapy in maxillo-facial conditions.
LIMITATIONS
The majority of respondents were physiotherapists which could have introduced bias.
The small needs analysis sample size could lead to misrepresentation of results therefore care was taken during the interpretation of the results. As the needs analysis investigated the need for physiotherapy in a currently unexplored area in South Africa, the original sample was planned to include one adequately qualified academic representative from each training institution in South Africa, to ensure that the results were applicable and of value. The needs analysis has formed the basis for a further in-depth Delphi study, consisting of an expert review panel of maxillo-facial surgeons, physiotherapists as well as dentists, regarding a possible physiotherapeutic intervention programme for mandibular condyle fracture patients.
Some participants demonstrated hesitance when answering questions regarding physiotherapy treatment for mandibular condyle fractures, as they did not necessarily have practical experience in the field. This resulted in some needs analysis questions not being answered by all participants.
There is a strong possibility that recall bias may have affected the answers to questions relating to patient reporting of functional loss in-hospital and at follow-up after surgical intervention.
The questionnaire did not provide for participants who had not the experience of managing the cases. The setup for the questionnaire could be adjusted according to the participants' clinical experience so that those without the relevant background would respond to a separate bank of questions. This would enhance the validity of the process.
Declaration: No conflict of interest declared
ACRONYMS
ORIF: Open Reduction and Internal Fixation
OMPT: Orthopaedic Manipulative Physical Therapy
References
1. Sawazaki R, Lima SM, Asprino L, Moreira LWF, de Moraes M. Incidence and patterns of mandibular condyle fractures. J Oral Maxillofac Surg 2010; 68:1252-9. [ Links ]
2. Desai J. Mandibular fracture patterns as related to mechanism and nature of injury- a prospective audit of Johannesburg patients. Faculty of Health Sciences, University of the Witwatersrand, Johannesburg. 2006. [ Links ]
3. Rikhotso E, Ferretti C. A prospective audit over a six month period of condylar fractures at Chris Hani Baragwanath Hospital. SADJ 2008; 63: 222-5; 228-9. [ Links ]
4. Singh AS. An Audit of Maxillofacial Fractures in Patients attending the Medunsa Oral Health Centre, University of Limpopo, Medunsa Campus. Faculty of Health Sciences, University of the Witwatersrand, Johannesburg. 2009. [ Links ]
5. Yun PY, Kim YK. The role of facial trauma as a possible etiologic factor in temporomandibular joint disorder. J Oral Maxillofac Surg 2005; 63: 1576-83. [ Links ]
6. Feng Z, Chen R, Zhang Y et al. Outcome of postsurgical sequential functional exercise of jaw fracture. J Craniofac Surg 2009; 20: 46-8. [ Links ]
7. Gonzalez AJJ, SakamakiH, Hatori M, NagumoM. Evaluation of trismus after treatment of mandibular fractures. J Oral Maxillofac Surg 1992; 50:223-8. [ Links ]
8. Andreasen JO, Jensen SS, Kofod T, Schwartz O, Hillerup S. Open or closed repositioning of mandibular fractures: Is there a difference in healing outcome? A systematic review. Dent Traumatol 2008; 24:17-21. [ Links ]
9. Zwieg BE. Complications of mandibular fractures. Atlas Oral Maxillofac Surg Clin. North Am 2009; 17: 93-101. [ Links ]
10. Thiele RB, Marcoot RM. Functional therapy for fractures of the condyloid process in adults. J Maxillofac Surg 1985; 43: 226-8. [ Links ]
11. Bevilaqua-Grosso D, Monteiro-Pedro V, De Jesus Guirro RR, Bérzin F. A physiotherapeutic approach to craniomandibular disorders: a case report. J Oral Rehabil 2002; 29: 268-73. [ Links ]
12. Chen CT, Feng CH, Tsay PK, Lai JP, Chen YR. Functional outcomes following surgical treatment of bilateral mandibular condylar fractures. Int J Oral Maxillofac Surg 2011; 40: 38-44. [ Links ]
13. Hwang K, Park JH, Lee HJ. Miniplate fixation of high condylar fracture and postoperative exercise regimen. J Craniofac Surg 2005; 16: 113-6. [ Links ]
14. Trott PH. The management of TMJ patients: part 1. 2011. Available from: <http://www.clinicalsolutions.co.za. [ Links ] [Accessed on 7 September 2011].
15. McCarty WL Jr, Darnell MW. Rehabilitation of the temporo-mandibular joint through the application of motion. Cranio 1993; 11: 298-307. [ Links ]
16. McNeely ML, Olivio SA, Magee DJ.A. Systematic review of the effectiveness of physical therapy interventions for temporo-mandibular disorders. Phys Ther 2006; 86: 710-23. [ Links ]
17. Miles-Tapping C, Dyck A, Bunham S, Simpson E, Barber L. Canadian therapists' priorities for clinical research: A Delphi study. Phys Ther 1990; 70:448-54. [ Links ]
8. Deutskens E, De Ruyter K, Wetzels M, Oosterveld P. Response rate and response quality of internet-based surveys: An experimental study. J. Mark. Res 2004;15:1, 21-36. [ Links ]
19. Keeny S, Hasson F, McKenna H. Consulting the oracle: ten lessons from using the Delphi technique in nursing research. J Adv Nurs 2006; 53:205-12. [ Links ]
20. Hung H, Altschuld JW, Lee Y. Methodological and conceptual issues confronting a cross-country Delphi study of educational program evaluation. Eval Program Plann 2008; 31: 191- 8. [ Links ]
21. Pruitt SD, Epping-Jordan JE. Preparing the 21st century global healthcare workforce. BMJ 2005; 330:637-9. [ Links ]
 Correspondence:
Correspondence:
A van der Merwe
Department of Physiotherapy
Christiaan de Wet Building
Rektor Avenue
University of the Free State
Bloemfontein, 9301
Tel: 051 401 3289
Cell: 082 446 4923
E-mail: gonzalesa@ufs.ac.za

{kind=link}
{kind=link}