










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.70 n.4 Johannesburg May. 2015
CLINICAL WINDOW
What's new for the clinician? Summaries of and excerpts from recently published papers
Compiled and edited by V Yengopal
MChD (Community Dentistry) Stellenbosch. Department of Community Dentistry, School of Oral Health Sciences, University of the Witwatersrand. E-mail: \/eerasamyYengopal@wits.ac.za
1. Cone beam computed tomography in comparison to conventional imaging techniques for the detection of bone invasion in oral cancer
Linz C, Müller-Richter ÜDA, Buck A, Mottok A, Ritter C, Schneider P, et. al.
The precise determination of the extent of a local tumour in oral cancer patients is crucial for therapy planning and prognostic stratification.1 Bone invasion is present in 1256% of all oral cancer patients and often requires radical surgery with wide resection which can significantly reduce the quality of life and increase morbidity and mortality of affected patients.1
Standard preoperative staging consists of clinical examination and non-invasive imaging, including computed tomography (CT) or magnetic resonance imaging (MRI), to detect loco-regional metastasis and to determine the extent of the primary tumour and infiltration into adjacent structures. Other available options include bone scintigraphy (BS), which visualizes the bone metabolism of the whole body, and is a highly sensitive imaging method, cone beam computed tomography (CBCT) and panoramic radiography (PR). Linz and colleagues (2015)1 reviewed a cohort of 197 patients with confirmed diagnoses of oral cancer and compared CBCT with other imaging technologies (PR, CT, MRI, and BS) in predicting bone invasion.
MATERIALS AND METHODS
This German study consisted of 352 patients with a suspected diagnosis of oral cancer. The standard CT or M RI was performed in all of the patients for the assessment of cervical lymph nodes and the extent of the local tumour. A total of 197 of these 352 patients underwent additional BS and CBCT and were therefore included in the study. Medical history, tumour localization, and recent interventions in the oral cavity, e.g., tooth extraction or probe sampling, were documented and accounted for in image interpretation. The imaging findings were validated by histopathology after either a rim or segmental bone resection or a clinical follow-up of at least six months.
For the PR and CBCT two experienced maxillofacial surgeons evaluated the images in consensus using Sidexis XG software, version 2.56 (Sirona Dental Systems Inc.). The diagnosis was first made on the basis of the reconstructed panoramic view. The absence or presence of bone invasion was judged. Osseous tumour invasion was considered to be present when at least cortical bone erosion or degradation was observed.
For bone scintigraphy, images were evaluated by two experienced nuclear physicians. Bone tissue invasion was suspected if (focally) increased radiotracer uptake in comparison to the surrounding bone tissue or the contralateral bone structures was evident and was observed adjacent to the primary cancer.
For CT and MRI, the scans were evaluated by two radiologists who assessed the extent of the local tumour and cervical lymph node metastasis. If both CT and MRI were performed in the same patient 10/197 patients; 5.1%), the presence of bone invasion was primarily assessed using CT.
Following surgical resection, the tissue samples were submitted to Pathology for further macroscopic and microscopic examination, especially to determine the tumour stage and grade.
The results of the different imaging modalities were compared with the histopathology or follow-up data results. The sensitivity, specificity, accuracy, negative and positive predictive values, and false-positive and false-negative values were obtained for each imaging modality. The results of the imaging methods were compared using McNemar's test.
RESULTS
The mean age of the patients (n = 197) at the time of surgery was 63.7 years (range 40-92 years; standard deviation (SD) ±8.8 years). The imaging findings were validated by histopathology in 114 of 197 patients (57.9%), confirming bone invasion in 66 (57.9%) and excluding it in 48 (42.1%). Due to the absence of clinical signs of bone invasion in the remaining 83/197 patients (42.1%), no bone resection was performed. In these cases, at least six months of follow-up (mean 22.3 months, range 6.0-66.3 months, SD ±14.4 months) confirmed the absence of bone invasion, resulting in an overall presence of bone invasion in 33.5% (66/197) of the patients.
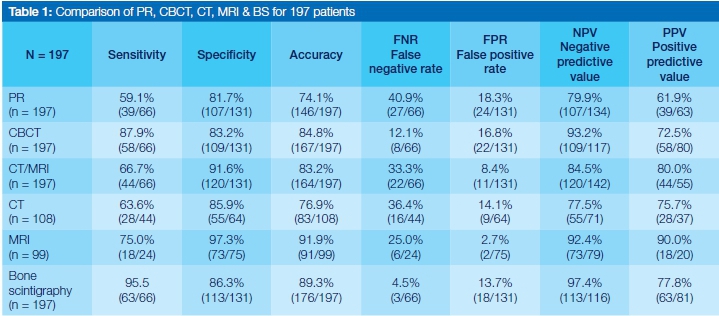
CBCT was significantly better than PR (p = 0.002), with a sensitivity of 87.9% (58/66), specificity of 83.2% (109/131), and corresponding accuracy of 84.8% (167/197). The negative predictive value was 93.2% (109/117) and the positive predictive value was 72.5% (58/80).
The sensitivity of BS was 95.5% (63/66) and the specificity was 86.3% (113/131), resulting in an accuracy of 89.3% (176/197). The negative predictive value was calculated as 97.4% (113/116) and the positive predictive value as 77.8% (63/81). Significantly better results were observed for BS compared to PR (p= 0.000). The accuracy of CBCT (p=0.188) was not significantly different.
The sensitivity of CT/MRI was 66.7% (44/66), the specificity was 91.6% (120/131), and, accordingly, the accuracy was 83.2% (164/197). With CT/MRI, the achieved accuracy was lower than with CBCT or BS (p = 0.771 and p = 0.058, respectively) and significantly different from PR (p = 0.020). All of the results are summarized in Table 1.
CONCLUSION
The authors concluded that CBCT and BS showed the highest accuracy for the detection of bone invasion and showed better performance than PR and CT/MRI.
IMPLICATIONS FOR PRACTICE
Regarding the evaluation of bone invasion, CBCT and BS might be the modalities of choice. However, CT and/or MRI remain essential for lymph node staging and for the detection of soft tissue involvement. Clinicians should note that each method has certain advantages and the setting, context and patient circumstances should be considered when choosing the type of imaging to aid diagnosis and therapy planning for patients with oral tumours.
ACRONYMS
Bs: bone scintigraphy
CT: computed tomography
CBCT: cone beam computed tomography
MRI: magnetic resonance imaging
PR: panoramic radiography
REFERENCE
2. Surgical versus non-surgical treatment of mandibular condylar fractures: a meta-analysis
Chrcanovic BR
Approximately 30-40% of all mandibular fractures (MFs) are fractures of the mandibular condyle.1 Most are not caused by direct trauma, but follow indirect forces transmitted to the condyle from a blow elsewhere. Consequently, mandibular condylar fractures (MCFs) are those most commonly missed.1 There are two principal therapeutic modalities for these fractures: non-surgical (functional) and surgical. Historically, non-surgical treatment of MCFs by means of maxillomandibular fixation (MMF) followed by physiotherapy was the standard practice.1
With the development of improved materials for fixation and the refinement of surgical techniques, open reduction and internal fixation (ORIF) has gained higher acceptance by surgeons for the management of MCFs.1 The ORIF technique provides stable three-dimensional reconstruction, promotes primary bone healing, shortens the treatment time, and eliminates the need for early release of the MMF. There has been considerable controversy regarding the treatment of MCFs, in particular whether they should be treated conservatively or surgically. Chrcanovic (2015)1 undertook a systematic review and meta-analysis of studies published in the literature up to and including February 2014 in order to verify whether there was a significant difference in the clinical outcomes and post-treatment complications between the surgical and the non-surgical treatment of unilateral or bilateral MCFs, in patients of any age or gender.
MATERIALS AND METHODS
An electronic search without time or language restrictions was undertaken in February 2014 in the following databases: PubMed, Web of Science, and the Cochrane Oral Health Group Trials Register. A manual search of selected journals on the subject was also performed and the reference lists of the identified studies and relevant reviews on the subject were also scanned for possible additional studies. Eligibility criteria included clinical human studies-randomized controlled trials (RCTs), controlled clinical trials (CCTs), or retrospective-comparing the clinical outcomes between surgical and non-surgical treatment of MCFs, and reporting the incidence of post-treatment complications. The following were excluded: case reports, technical reports, animal studies, in vitro studies, and reviews papers.
The titles and abstracts of all reports identified through the electronic searches were assessed. The full text was obtained for studies appearing to meet the inclusion criteria and for studies for which there were insufficient data in the title and abstract to make a clear decision.
A quality assessment was performed using the recommended approach for assessing the risk of bias in studies included in Cochrane reviews. The classification of the risk of bias potential for each study was based on the following four criteria: sequence generation (random selection in the population), allocation concealment (steps must be taken to secure strict implementation of the schedule of random assignment by preventing foreknowledge of the forthcoming allocations), incomplete outcome data (clear explanation of withdrawals and exclusions), and blinding (measures to blind study participants and personnel from knowledge of which intervention a participant received). Incomplete outcome data was also considered addressed when there were no withdrawals and/or exclusions. A study that met all the criteria mentioned above was classified as having a low risk of bias. A study that did not meet one of these criteria was classified as having a moderate risk of bias. When two or more criteria were not met, the study was considered to have a high risk of bias.
The following data were extracted (when available) from the studies included in the final analysis: year of publication, study design, number of patients, patient age range and/or mean age, follow-up period, number of MCFs, associated MFs, fixation methods, surgical approach, length of operation, post-treatment MMF, use of antibiotics and/ or chlorhexidine, inclusion criteria for patients, post-treatment radiological assessment, and post-treatment complications. Authors were contacted via e-mail to request missing data if possible.
The I2 statistic was used to express the percentage of the total variation across studies due to heterogeneity, with 25% corresponding to low heterogeneity, 50% to moderate heterogeneity, and 75% to high heterogeneity. The estimates of an intervention for dichotomous outcomes were expressed as the risk ratio (RR) and for continuous outcomes as the mean difference (MD) in millimeters, both with a 95% confidence interval (CI). Only if there were studies with similar comparisons reporting the same outcome measures was a meta-analysis to be attempted. A funnel plot to assess publication bias was done. The data were analysed using the statistical software Review Manager (version 5.2.8).
RESULTS
From the initial 400 "hits" identified in the search strategy, a total of 36 publications were included in the review. In total 1982 patients were enrolled in the 36 studies, with 1094 MCFs in the surgical treatment group and 1307 MCFs in the non-surgical treatment group. The presence of associated MFs was reported in 19 studies, but only seven studies reported the precise location of the fractures. The most prevalent associated MF was fracture of the symphysis/ parasymphysis region, with 78.3% (227/290) of the reported associated MFs of known location. The maximum follow-up period varied between 3 months and 13 years.
All 36 studies were judged to be at high risk of bias.
When considering only the dichotomous outcomes, there was heterogeneity among the studies for the outcome TMJ pain (I2 = 53%, P = 0.009), but not for infection (|2=0%, P=0.99), malocclusion (I2 = 11%, P = 0.30), lateral deviation during maximum inter-incisal opening (MIO) (I2 = 24%, P = 0.21), or TMJ noise (I2 = 0%, P = 0.41). There was a statistically significant effect on the outcome of post-treatment malocclusion (RR 0.46, 95% CI 0.34-0.62, P<0.00001) and lateral deviation during MIO (RR 0.56, 95% CI 0.43-0.74, P < 0.0001) favouring surgical treatment, and of post-treatment infection (RR 3.43, 95% CI 1.10-10.75, P = 0.03) favouring non-surgical treatment. There was no statistically significant effect on the outcome TMJ pain (RR 0.81, 95% CI 0.46-1.42, P = 0.46) or TMJ noise (RR 1.44, 95% CI 0.78-2.65, P = 0.24) in favour of surgical treatment. Only three studies provided information on malunion and non-union, with no cases reported. Thus, an analysis of these outcomes was not performed.
The test for overall effect revealed a statistically significant advantage for surgical treatment when the incidence of all post-treatment complications (dichotomous outcomes) was considered (RR 0.70, 95% CI 0.54-0.90; P = 0.006). The cumulative RR was 0.70, meaning that surgical treatment in the management of MCFs decreases the risk (relative risk reduction-RRR) of these events (post-treatment complications of dichotomous outcome) by 30%.
When only considering the continuous outcomes, there was heterogeneity among the studies for the outcomes MIO (I2=95%, P < 0.0001), laterotrusion (I2=61%, P<0.0001), and protrusion (I2 = 59%, P = 0.004), but not for lateral deviation during maximum inter-incisal opening (MIO) (I2=31%, P=0.18). There was a statistically significant effect on the outcome of protrusion (MD 0.68, 95% CI 0.141.22, P = 0.01), laterotrusion (MD 0.53, 95% CI 0.05-1.01, P=0.03;), and lateral deviation during MIO (MD -0.75, 95% CI -1.23 to -0.27, P = 0.002) favouring surgical treatment. There was no statistically significant effect on the outcome of MIO (MD 2.24, 95% CI -0.70 to 5.19, P = 0.14) in favour of surgical treatment.
The test for overall effect revealed a statistically significant advantage for surgical treatment when the incidence of all post-treatment complications (continuous outcomes) was considered (MD 1.17, 95% CI 0.50-1.84; P = 0.0006).
Concerning the length of operation, only one study provided information on the mean operation time, with a mean time of 132 min for the surgical treatment group and 72 min for the non-surgical treatment group. Thus, a meta-analysis was not possible.
The funnel plot for the dichotomous outcomes did not show asymmetry, indicating an absence of publication bias. The funnel plot for the continuous outcomes showed asymmetry, indicating the possible presence of publication bias.
CONCLUSION
The results of this meta-analysis suggest that the surgical treatment of MCFs provides a better clinical outcome with regard to post-treatment malocclusion, protrusion, laterotrusion, and lateral deviation during maximum inter-incisal opening in comparison with non-surgical treatment. However, patients are more affected by post-treatment infection when a surgical treatment is performed. There were no statistically significant differences in post-treatment TMJ pain, TMJ noise, or MIO when the two techniques were compared.
IMPLICATIONS FOR PRACTICE
As more refined surgical techniques are introduced, the option of surgical versus non-surgical management of MCFs seems to favour the surgical approach.
ACRONYMS
CI: confidence interval
CCTs: controlled clinical trials
MCFs: mandibular condylar fractures
MMF: maxillomandibular fixation
MFs: mandibular fractures
MIO: maximum inter-incisal opening
MD: mean difference
ORIF: open reduction and internal fixation
RCT: randomized controlled trials
RRR: relative risk reduction
RR: risk ratio
REFERENCE
3. Immediately loaded non-submerged versus delayed loaded submerged dental implants: a meta-analysis
Chrcanovic B.R, Albrektsson T, Wennerberg A
Historically, the original Bránemark protocol for placing dental implants prescribed a two-stage surgery with a submerged healing period of at least three months in the mandible and six months in the maxilla, allowing the implant to osseointegrate without being exposed to external forces.1 After bone healing, a second surgery is performed to connect a healing abutment.
Over time, the concepts of implant placement in fresh extraction sockets, immediate loading, and non-submerged implants were introduced, focusing on shorter and less invasive procedures.1 To reduce the treatment time and offer the patient early function and aesthetics, a one-stage surgical procedure and loading of the implants as soon as possible are recommended.1 In the one-stage surgical approach (non-submerged implant), the coronal part of the implant is positioned above the gingiva level in the case of single-part implants, or transmucosal healing abutments are placed in the case of two-part implants. In the one-stage surgical approach, the implant can be loaded immediately or not.
Inserting implants in one stage has several advantages. Only one surgical intervention is required, which is convenient for the patient, especially for the medically compromised patient.1 In addition, there is a considerable cost-benefit advantage. The prosthetic phase can start earlier because there is no wound-healing period related to a second surgical procedure! Although immediate loading of implants shortens the treatment duration and also provides patients with an acceptable aesthetic appearance, there is concern that immediate loading may increase the risk of implant failure.1
Chrcanovic et al (2015)1 undertook a systematic review with meta-analysis to compare the survival rate, postoperative complications, and marginal bone loss of non-submerged immediately-loaded dental implants with those of submerged delayed-loaded implants.
MATERIALS AND METHODS
An electronic search without time or language restrictions was undertaken in March 2014 in the following databases: PubMed, Web of Science, and the Cochrane Oral Health Group Trials Register. A manual search of selected journals covering dental implant research was also done and the reference lists of the studies identified and relevant reviews on the subject were also scanned for possible additional studies.
Eligibility criteria included clinical human studies, either randomized or not, comparing implant failure rates in any group of patients receiving submerged versus immediately loaded non-submerged dental implants. Only the studies immediately loading all non-submerged implants were considered.
The titles and abstracts of all reports identified through the electronic searches were read independently by the three authors. For studies appearing to meet the inclusion criteria, or for which there were insufficient data in the title and abstract to make a clear decision, the full report was obtained. Disagreements were resolved by discussion between the authors.
The quality assessment was performed using the recommended approach for assessing risk of bias in studies included in Cochrane reviews. The classification of the risk of bias potential for each study was based on the four following criteria: sequence generation, allocation concealment, incomplete outcome data and blinding. A study that met all the criteria mentioned above was classified as having a low risk of bias, a study that did not meet one of these criteria was classified as having a moderate risk of bias, and when two or more criteria were not met, the study was considered to have a high risk of bias.
The following data were extracted from the studies included in the final analysis, when available: year of publication, study design, single centre or multi-centre study, number of patients, patient age, follow-up, days of antibiotic prophylaxis, use of mouth rinse, implant healing period, failed and placed implants, and postoperative infection. Contact was made with authors to obtain missing data, if possible.
Implant failure and postoperative infection were the dichotomous outcome measures evaluated. Weighted mean differences were used to construct forest plots of marginal bone loss, a continuous outcome. The statistical unit for the outcomes was the implant. Whenever outcomes of interest were not clearly stated, the data were not used for analysis. The I2 statistic was used to express the percentage of the total variation across studies due to heterogeneity, with 25% corresponding to low heterogeneity, 50% to moderate and 75% to high. In the case of statistically significant (p<0.10) heterogeneity, a random-effects model was used to assess the significance of treatment effects. Where no statistically significant heterogeneity was found, analysis was performed using a fixed-effects model. The estimates of an intervention were expressed as the risk ratio (RR) and as the mean difference (MD) in millimetres for continuous outcomes, both with a 95% confidence interval (CI). Statistical significance was set at P < 0.05. Only if there were studies with similar comparisons reporting the same outcome measures was a meta-analysis to be attempted.
A funnel plot (plot of effect size versus standard error) was used to assess publication bias. The data were analysed using the statistical software Review Manager (version 5.2.8)
RESULTS
The search strategy resulted in identified 1328 papers, of which 28 were included in the review. In the 28 studies comparing the procedures, a total of 3918 dental implants were non-submerged and immediately loaded, with 263 failures (6.71%), and a total of 7194 implants were submerged, with 446 failures (6.20%). There was no implant failure in three studies. Twenty-three studies were judged to be at high risk of bias, whereas one study was considered at moderate risk of bias and four studies at low risk of bias.
In this study, a random-effects model was used to evaluate implant failure in the comparison between the procedures, since statistically significant heterogeneity was observed (P < 0.00001; I2 = 76%). The insertion of dental implants through the two different techniques statistically affected the implant failure rate in favour of the submerged procedure (P = 0.02). The RR of 1.78 (95% CI 1.12-2.83) implies that failures are 1.78 times more likely to happen when implants are immediately loaded than when implants are submerged. Thus, the relative risk reduction (RRR) is -78%. The RRR is negative, i.e. immediately loaded non-submerged implants increase the risk of implant failure by 78%. The number needed to treat (NNT) to prevent one patient having an implant failure is 50 (95% CI 25-100).
The funnel plot showed asymmetry when the studies reporting the outcome 'implant failure' were analysed, indicating the possible presence of publication bias.
CONCLUSION
The difference between immediately loaded non-submerged dental implants and delayed loaded submerged implants statistically affected the implant failure rate (failures were 1.78 times more likely to happen when implants were immediately loaded than when implants are submerged). No statistically significant effects on the occurrence of postoperative infection or on marginal bone loss were observed between the two different techniques.
IMPLICATIONS FOR PRACTICE
This systematic review with meta-analysis provides good evidence that the traditional delayed loading of implants resulted in significantly less implant failure than with the immediately loaded non-submerged dental implants.
ACRONYMS
CI: confidence interval
MD: mean difference
RRR: relative risk reduction
RR: risk ratio
REFERENCE
1. B.R. Chrcanovic, Albrektsson T, Wennerberg A. Immediately loaded non-submerged versus delayed loaded submerged dental implants: A meta-analysis. International Journal of Oral & Maxillofacial Surgery, 2015; 44: 493-506. [ Links ]
1. Linz C, Müller-Richter UDA, Buck A, Mottok A, Ritter C, Schneider P, et. al., Performance of cone beam computed tomography in comparison to conventional imaging techniques for the detection of bone invasion in oral cancer. International Journal of Oral & Maxillofacial Surgery, 2015; 44: 8-15. [ Links ]
1. Chrcanovic BR. Surgical versus non-surgical treatment of mandibular condylar fractures: a meta-analysis. International Journal of Oral & Maxillofacial Surgery, 2015; 44: 158-179. [ Links ]

{kind=link}