










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.70 n.4 Johannesburg May. 2015
RADIOLOGY CASE
Maxillo-facial radiology case 130
CJ Nortjé
BChD, PhD, ABOMR, DSc. Faculty of dentistry, University of the western Cape. e-mail: cnortje@uwc.ac.za
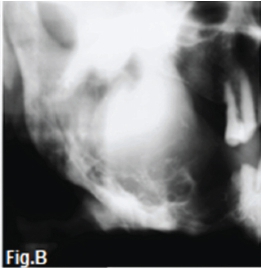
This elderly man (Fig. A) presents with a history of a painful slow growing soft tissue swelling in his right jaw. The patient also reported paraesthesia of the right lower lip as well as paroxysms of intense general bone pain. During clinical examination of the oral cavity a very large soft tissue swelling was observed in the right angle and body of the mandible. You decide to take a panoramic radiograph of the jaws. What is your diagnosis?

INTERPRETATION
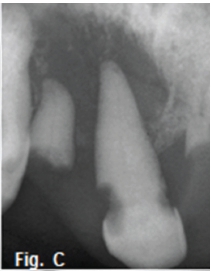
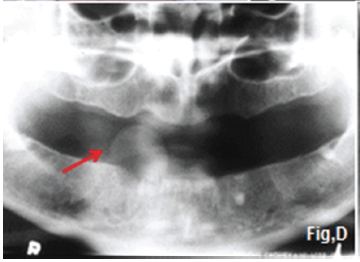
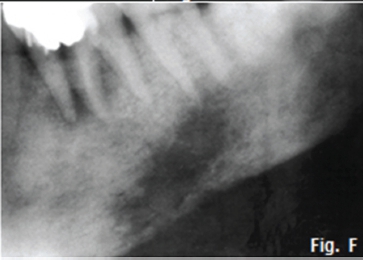
A soft tissue mass (Fig. B) with an underlying multilocular bone lesion is discernible. There is also destruction of the superior border of the cortex. Due to the presence of paraesthesia a provisional diagnosis of a malignancy was made. Histological diagnosis confirmed the presence of a metastatic prostate carcinoma. Secondary or metastatic carcinoma is the commonest malignant tumour in bone. Notwithstanding the frequency with which bone is involved in metastatic disease, the jaws are rarely affected. The unsolicited complaint of numbness or paraesthesia is the main symptom, and it is very striking how frequently it occurs and yet is neglected. The most frequent sites of metastasis to bone are areas occupied by red bone marrow. Most carcinomas that occur in the jaws from metastasis often arise in the central portion of the jaws, an area richest in red marrow. Metastases may occur anywhere in either jaw, but there seems to be a preference for the third molar region of the mandible. Fig. C is a case of metastatic adeno-carcinoma of the lung, showing a well circumscribed but uncorticated lytic lesion while Fig. D (red arrow) is a metastatic carcinoma of the uterus which presented after a loose tooth was extracted. Note the irregular "moth-eaten" rarefaction adjacent to first molar and second premolar teeth of a metastatic carcinoma of the breast (Fig. F). Metastases in bone show two main radiographic appearances, firstly, frank destruction of an area of bone without new bone formation within the lesion or adjacent bone. In this instance, the lesion is considered to be relatively slow growing and less aggressive than other malignant presentations, such as moth-eaten and infiltrative patterns. The second radiographic appearance of the lytic or radiolucent type of metastasis in the jaw has considerable resemblance to some manifestations of osteomyelitis, characterized by the presence of many areas of bone destruction, some of which may not be more than 2 mm in diameter. Generally, osteomyelitis presents a moth-eaten pattern only. Pathologic fracture may be seen in the area of rarefaction, although this is very uncommon. Metastatic disease is more common in older age groups, with a mean age in the mid-fifties.
References
1. Pindborg, J.J & Hjorting-Hansen, E: Atlas of Diseases of the Jaws. W.B Saunders, 1974: p 50-4. [ Links ]
2. Farman AG, Nortjé CJ & Wood R E: Oral and Maxillofacial Imaging, 1st Ed, Mosby. St. Louis, Missouri 1993 p 300-4. [ Links ]
Note: Permission has been granted to reproduce the photograph of the patient.
