










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.70 no.2 Johannesburg Mar. 2015
RADIOLOGY CASE
Maxillo-facial radiology case 128
CJ Nortjé
BChD, PhD, ABOMR, DSc. Faculty of Dentistry, University of the western Cape. e-mail: cnortje@uwc.ac.za
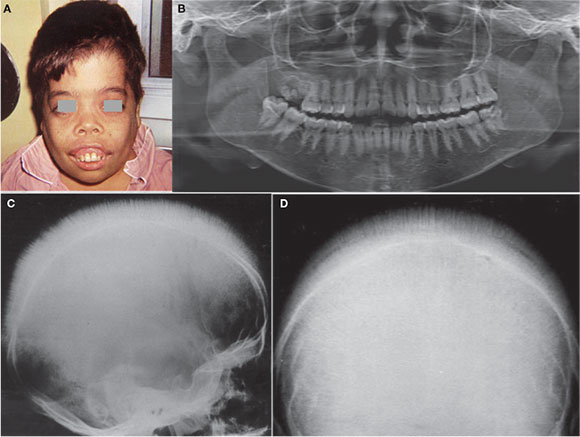
The lower clinical picture and radiographs represents a condition where the general growth is retarded, the children are pale due to anaemia and the most noticeable change of the oral structures is enlargement of the maxilla. What is your diagnosis?
INTERPRETATION
The images represent features of Thalassemia which is a congenital, familial haemolytic anaemia, also named Cooley's anaemia or Mediterranean anaemia.Three forms of the anaemia are recognised, the major, the intermediate and the minor type. Thalasemia major is genetically the homozygous type with both parents having the abnormal haemoglobin, whereas the thalassemia minor is genetically the heterozygous type. Symptoms are almost exclusively connected with the major type. The excact nature of the disease is unknown, although it is recognized that the red blood cells in thalassemia major have a shortened life span and also contain fetal haemoglobin. This would suggest a defect in some component of the factors controlling the rate synthesis of adult haemoglobin (Hb A). The onset of the severe form of the disease (thalassemia major) is within the first two years of life. Siblings are commonly affected. The child has a yellowish pallor of the skin and exhibits fever, chills, malaise and a generalized weakness. Thalassemia is common in Africans but also in Italians and Greeks. The thalassemia trait may confer a degree of protection against malaria, which confers a selective survival advantage on carriers. Enlargement of the maxilla is the most noticeable change of the oral structures. The maxilla in children is rich in red marrow. Since the erythrocytes are deficient, the production is high and the marrow becomes hyperplastic; this causes the overgrowth. There is bulging of the alveolar process, and overbite or open bite is often present (Figure A courtesy of Dr. M, Ulmansky, Jerusalem, Israel). A coarse trabecular pattern of the alveolar bone of the maxilla and mandible is very often encountered as well as thinning of inferior cortex of the mandible and stepladder arrangement of interdentally trabeculae resembling very fine lattice (Figure B). Enlargement of the jaws in a vertical dimension is also discernible. In later stages the calvarium presents the classic "hair on end appearance" This is a very striking appearance. The individual bony spicules may stand above the bone for a distance of over a centimetre; there are many and they may involve the whole or greater part of the vault of the skull (Figures C and D). Treatment of thalassemia is regular transfusion protocol. Recent studies recommend RBC transfusion when the Hgb level is less than 9.5g /dl. This therapy appears to be a reasonable compromise that is effective in reducing ineffective eryythropoiesis and other pathophysiologic consequences of thalassemia.
Reference
1. Farman AG, Nortjé CJ & Wood R E: Oral and Maxillofacial Imaging, 1st Ed, Mosby. St. Louis, Missouri 1993 pp 151-152 [ Links ]
2. Pindborg JJ &Hjorting-Hansen E: Atlas of Diseases of the Jaws 1st Ed. Munksgaard, Copenhagen. 1974 p126. [ Links ]
