










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.70 no.2 Johannesburg mar. 2015
RESEARCH
A comparison of the efficacy of various disinfection protocols in endodontic treatment: An in vitro study
N WarrenI; PJ van der VyverII; FS BothaIII
IBChD, Dip Odont (Endo), MSc (Odont) (Pret). Oral and Dental Hospital, Division of Endodontics, Department of Odontology, School of Dentistry, Faculty of Health Care Sciences, University of Pretoria
IIBChD, Dip Odont (Endo), Dip Odont (Aest), MSc (Odont) (Pret). Extraordinary Professor, Department of Odontology, School of Dentistry, University of Pretoria
IIIBSc (Hons), MSc (PU for CHO), PhD (Pret). Department of Paraclinical Sciences, Faculty of Veterinary Science, University of Pretoria
SUMMARY
INTRODUCTION: Disinfection is the main objective of root canal preparation and whilst irrigation is most commonly used, another method is Photo-activated Disinfection (PAD).
AIMS AND OBJECTIVES: The aim of this in vitro study was to compare the efficacy of eradication of bacteria from root canals by six different disinfection protocols.
METHODS: Root canals of 84 extracted human teeth were prepared to a standardised size and taper. The teeth were sterilised and then inoculated with E. faecalis. The teeth were randomly assigned to one of seven groups (n = 12), each of which underwent a different disinfection protocol. Dentine samples were plated onto BHI plates and incubated anaerobically. After five days, colony-forming units (cfu) were counted. The Pairwise Wilcoxon Rank Sum test and the Kruskal-Wallis test were used for statistical analysis of the data.
RESULTS: The most effective disinfection protocol was: 3% NaOCl with 2% CHX, followed by 3% NaOCl with PAD, Chlor-XTRA and 2% CHX. The 3% NaOCl-protocol performed significantly better than PAD and distilled water. The PAD-protocol performed significantly better than distilled water.
CONCLUSION: The most efficient protocol in eradicating E. faecalis from the root canals was 3% NaOCl followed by irrigation with 2% CHX.
INTRODUCTION
The majority of persistent endodontic infections are strongly associated with the invasion of the pulp by facultative anaerobic bacteria.1,2,3 Chemo-mechanical root canal preparation is crucial in endodontic treatment4 to ensure removal of the residual pulp tissue, fragments of dentine and pathogenic microorganisms.1 The chemical dissolution of these organic and inorganic components is equally important to the physical flushing action of irrigation solutions.5,6,7
Enterococcus faecalis is a gram-positive, facultative, anaerobic microorganism that is frequently implicated in persistent periapical infection.3,8,9
Mechanical root canal cleaning and shaping leads to the occlusion of dentinal tubules by a deposit referred to as a "smear layer".10,11 If this barrier is in place, debris and organic and inorganic matter remain in the tubules and resident bacteria are not killed.12,13
Removing the smear layer is accomplished most efficiently by rinsing the root canal with 0.5%-5.25% sodium hypochlorite (NaOCl) to dissolve and flush out the organic remnants, followed by rinsing with a liquid chelating agent (17% liquid ethylene-diamine-tetra-acetic acid, EDTA) to dissolve inorganic components.14, 15, 16,17
A commercially available endodontic irrigant, Chlor-XTRA (Vista Dental Products, Racine, Wisconsin, USA), is an improved NaOCl (5.25%) solution containing also a wetting agent, surface modifying agents to reduce surface tension and alkylating agents to increase electrical ca-pacity.18 Chlorhexidine gluconate (CHX) is a cationic bis-guanide considered to be a broad-spectrum antimicrobial agent that can be used for root canal irrigation.6,19 Chlorhexidine molecules bind to hydroxyapatite crystals and to soft tissues resulting in a residual bacteriostatic phenomenon known as substantivity.19,20,21 Chlorhexidine gluconate would in all probability be the ideal endodontic irrigant were it not for its incapacity to dissolve organic matter.22 An endodontic irrigation regime that includes both CHX and NaOCI is beneficial in that the two solutions complement each other, one making up for the shortcomings of the other.23,24
A relatively new method of disinfection is Photo-activated disinfection (PAD) in which, for endodontic therapy, a non-toxic photo-sensitive agent (dye) is placed into the prepared root canal. Molecules within the dye attach to contacting bacterial cells and act as markers. A light source is applied inside the canal to initiate a chemical reaction. The molecules within the dye become excited. Highly reactive "singlet" oxygen* released from the dye has a toxic effect upon the "marked" bacterial cells, damaging their protoplasm, cell membrane and DNA. Ultimately this results in bacterial cell lysis and death.25,26
The aim of this in vitro study was to compare the efficacy of six different root canal disinfection regimens in the eradication of E. faecalis from the root canals of human maxillary incisors. The disinfection efficacy was compared by microbiological culture.
*an electronically excited molecular oxygen known as dioxygen or dioxidene.
MATERIALS AND METHODS
This in vitro study is based on a method modified from that first used by Haapasalo and 0rstavic in 1987,27 and applied successfully in many other experiments.5,28,29 Eighty four extracted single rooted teeth were collected. The crowns of the teeth were removed using a diamond wafering blade in an Isomet low speed saw (Buehler Ltd., Lake Bluff, Illinois, USA) leaving a standardised root canal length of 15mm.
The root canals were prepared using ProTaper Universal (Dentsply/Maillefer, Baillaigues, Switzerland) Nickel Titanium rotary endodontic files. The two shaper files S1 and S2 were used for crown-down preparation. Then the finisher files were used from the F1 to the F3 file, according to the manufacturers' instructions. A standardised taper was produced with a size 45, 6% taper ProFile (Dentsply/ Maillefer) rotary file. During preparation, copious amounts of 3% NaOCl (Rekitt Benckiser, South Africa (Pty) Ltd., Elandsfontein, Gauteng, South Africa) were used for root canal irrigation. After preparation the following sequencial irrigations were completed for each canal:
- 3% NaOCl for five minutes
- distilled water for two minutes.
- 17% EDTA (Vista Dental Products, Toronto, Canada) for one minute.
- distilled water for two minutes.
The teeth were then sterilised by autoclave (Hung-Lin Medical Instruments Co. Ltd.) at 121°C for 15 minutes. Before the inoculation procedure sterility of the root canals was assessed. Sterile paper points were inserted into the root canals of five randomly selected teeth. The paper points were placed onto Brain Heart Infusion (BHI) plates (Onderstepoort Biological Products Ltd.) which were incubated under facultative anaerobic conditions using Anae-rocult A® (Merck SA (Pty) Ltd.) at 37°C for three days. All cultures were negative, verifying that all the canals were sterile. The prepared teeth were randomly divided into seven groups (n=12) and the groups were placed into sterile glass containers. A McFarland standard 1 suspension (8 x 108 colony-forming units) in BHI broth (Merck SA (Pty) Ltd.) was prepared from 48-hour cultures of E. faecalis (ATCC 49474).30 A 1% inoculum of this was added to the teeth which were then incubated in a Vortex platform incubator (Ika-Works Inc. Germany) for 48 hours. Random dentine samples were taken from the prepared root canal of one tooth from each group, using a sterile round tungsten carbide bur size ISO 014 (Dentsply/Maillefer). The samples were placed onto BHI plates and incubated under anaerobic conditions (positive control). After 72 hours, numerous cfu's of the test organism were observed on the BHI plates. This served as confirmation that the root canals had been successfully inoculated with E. faecalis.
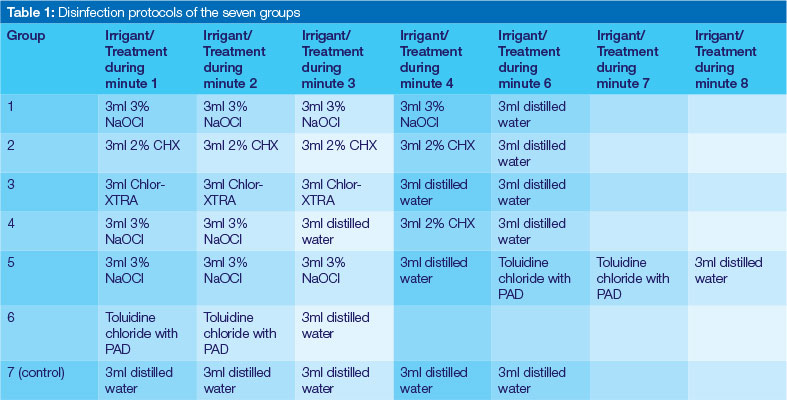
To each group was assigned a specific disinfection regime and the teeth treated according to that protocol (Table 1). The teeth were then split longitudinally. Three dentine samples were taken from one of the two sections (coronal, middle and apical) using a sterile round tung sten carbide bur size ISO 014. The dentine powder was collected over separate sterile pre-weighed Bijou bottles (Merck SA (Pty) Ltd.). The weight of the collected dentine was determined and the weight/volume concentration of each sample was calculated. This concentration was used to quantify the amount of viable E. faecalis that survived in each root canal.
One millilitre of sterile saline was added to the dentine in the Bijou bottles. The cfu were determined as follows: ten-fold dilutions were made in sterile quarter-strength Ringers solution. A quantity of 1ml of 10-3 to 10-7 of these dilutions was plated onto BHI agar plates.31 The BHI plates were incubated at 37°C for five days in facultative anaerobic conditions using Anaerocult A®. Colony forming units were counted after a period of five days.
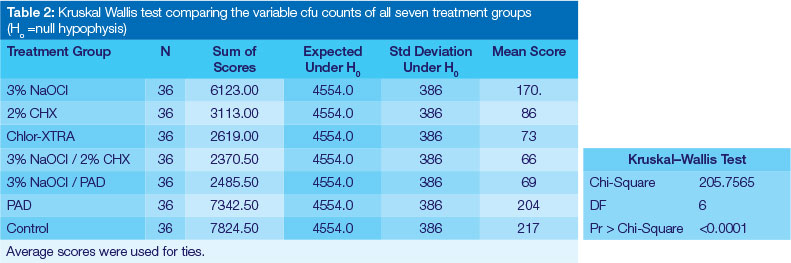
Data were collected and submitted to a statistician. A pairwise comparison of the cfu counts of all seven treatment groups was done using the Pairwise Wilcoxon Rank Sum test and a non-parametric analogue of the one-way ANOVA test, the Kruskal Wallis test.
RESULTS
The results of this study are presented in Tables 2 and 3. The results were analysed using the Pairwise Wilcoxon Rank Sum test and the Kruskal-Wallis test. A comparison of the cfu counts of all seven treatment groups is presented in Table 2. Of the six test groups, the irrigation regimen of 3% NaOCl combined with 2% CHX was the most effective in eradicating E. faecalis from the root canals. In descending order of efficacy, this protocol was followed by: 3% NaOCl in combination with PAD, Chlor-XTRA and 2% CHX. The protocols that performed the most poorly in this in vitro study were 3% NaOCl alone and PAD alone.
The Pairwise Wilcoxon Rank Sum test showed that there were no statistically significant differences between the disinfection effects of 2% CHX, Chlor-XTRA or 3% NaOCl/ PAD protocols. That using 3% NaOCl combined with 2% CHX was significantly more efficient than 2% CHX alone. PAD, 3% NaOCl and distilled water were significantly less efficient than the other disinfection protocols. The results of the group in which PAD was used did show that this method was statistically more effective in eradicating the test organism than was distilled water.
DISCUSSION
In this in vitro study comparing the efficacy of six different root canal disinfection regimens, E. faecalis was chosen as the test organism for its resilient, resistant nature,32,33,34 whilst the extracted tooth model has been shown to be a reliable method in the evaluation of the bactericidal effects of root canal irrigants.35 In an attempt to remove the smear layer which is formed during root canal preparation, 2.5% NaOCl was used for irrigation during preparation of the samples and 17% EDTA as the final rinse (continuous passive irrigation) for one minute.36,37,38
The combination of 3% NaOCl and 2% CHX was slightly more efficient at eradicating E. faecalis from the root canals than were the five other disinfection regimens that were tested. However, Vianna and Gomes (2009) found no enhancement of the bacterial eradication ability of CHX by using it in combination with NaOCl.39 Baca et.al (2011) showed a 100% increase in bactericidal rate when 2.5% NaOCl irrigation was followed by a final rinse with 2% CHX.24 Their study showed that under ideal conditions 2% CHX was able to destroy bacterial biofilm within two minutes, a finding supported by several other investigations.24,40
In contradiction to some literature, the results of the present study indicate that 3% NaOCl is not the best irrigation solution. However, one other paper does report a poor performance of this solution.41 The most likely reason for this inefficiency may be that the concentration of 3% NaOCl is not sufficiently potent to completely eradicate E. faecalis from infected dentine within the time of exposure to the irrigant.
There are few studies specifically investigating Chlor-XTRA as an irrigation solution. In 2012 Jungbluth et.al compared the activity of Chlor-XTRA with that of several brands of household bleach (NaOCl).42 The results of this study indicate that Chlor-XTRA (5.25% NaOCl) was significantly better than 3% NaOCl at eradicating E faecalis as also confirmed by several other studies.41,43,44
Souza et.al found that PAD applied with either methylene blue (MB) or toluidine blue (TB) did not significantly enhance root canal disinfection compared to chemo-mechanical preparation using NaOCl as an irrigant followed by PAD.45 The results of this present investigation, supported Souza' findings whether PAD was used after conventional irrigation with 3% NaOCl or was used alone. In fact, high numbers of E. faecalis cells were found in the PAD only treatment group. Several contradictory conclusions have been reported. Soukos et.al showed PAD to be 97% effective in reducing E. faecalis when applied alone for root canal disinfection46 whilst Foschi et.al also observed good results with the system, finding that PAD used with a diode laser achieved a bacterial reduction of 77,5%.47 In 2010, Schlafer et.al demonstrated a 99.7% reduction of the bacteria in suspension and a 95.82% reduction in the quantum of bacteria in adherence to the root canal wall.48 The number of viable E. faecalis cells in the root canal was reduced to 2.9% when Rios et.al treated root canals with PAD for 30 seconds alone and, when PAD was applied after NaOCl, they observed a reduction down to 0.1%.49
Irrigation with distilled water had no significant effect on the number of bacteria in the root canals.
Further studies should be carried out to determine the best application of the NaOCl/CHX solution combination regimen for endodontic irrigation. Additional studies need to be carried out to determine whether the additional time, effort and expense needed to apply PAD as a supplementary method of root canal disinfection is justifiable or not.
CONCLUSIONS
Whilst this study failed to identify any regime as offering complete eradication of E.faecalis it may be concluded that 3% NaOCl used in combination with 2% CHX will offer the clinician the best option to achieve the desired disinfection of the root canal.
Acknowledgements
The authors would like to thank Prof H.S. Schoeman for statistical analysis of the results. The authors acknowledge that funding for this research project was obtained from the Professor Cornelis H Pameijer Fellowship.
ACRONYMS
BHI: Brain Heart Infusion
Cfu: Colony-forming units
CHX: Chlorhexidine gluconate
EDTA: Ethylene-diamine-tetra-acetic acid
PAD: Photo-activated Disinfection
NaOCl: Sodium Hypochlorite
References
1. Berutti E, Castellucci A. Cleaning and shaping the root canal system In: Castellucci A editor. Endodontics: Volume II. Italy: Edizioni Odontoiatriche Il Tridente S.r.l. 2005. [ Links ]
2. Ingel JI, Backland LK. Endodontics. 5th ed. Ontario: Decker BC, Inc. 2002:63-202. [ Links ]
3. Wang Q, Zhang C, Chu C, Zhu X. Prevalence of Enterococcus faecalis in saliva and filled root canals of teeth associated with apical periodontitis. Int J Oral Sci 2012; 4:19-23. [ Links ]
4. van der Sluis LWM, Gambarini G, Wu MK, Wesselink PR. The influence of volume, type of irrigant and flushing method on removing artificially placed dentine debris from the apical root canal during passive ultrasonic irrigation. Int Endod J 2006; 39:472-6. [ Links ]
5. Heling I, Chandler NP. Antimicrobial effect of irrigant combinations within dentinal tubules. Int Endod J 1998; 31:8-14. [ Links ]
6. Ferraz CCR, Gomes BPFA, Zaia AA, Teixeira FB, Souza-Filho FJ. Comparative study of the antimicrobial efficacy of chlorhexidine gel, chlorhexidine solution and sodium hypochlorite as endodontic irrigants. J Endod 2007; 18:294-8. [ Links ]
7. Brándle N, Zehnder M, Weiger R, Waltimo T. Impact of growth conditions on susceptibility of five microbial species to alkaline stress. J Endod 2008; 34(5):579-82. [ Links ]
8. Sundqvist G, Figdor D. Endodontic treatment of apical periodontitis. In: 0rstavic D, Pitt Ford T, ed. Essential Endodontology. Oxford: Blackwell Science Ltd; 1998; 242-77. [ Links ]
9. Chavez de Paz LE, Dahlén G, Molander A, Mòller A, Bergen-holtz G. Bacteria recovered from teeth with apical periodontitis after antimicrobial endodontic treatment. Int Endod J 2003; 36:500-8. [ Links ]
10. Peters OA, Barbakow F. Effect of irrigation on debris and smear layer walls prepared by two rotary techniques. A scanning electron microscopic study. J Endod 2000; 26:6-10. [ Links ]
11. McComb D, Smith DC. A preliminary scanning electron microscopic study of root canals after endodontic procedures. J Endod 1975; 1:238-42. [ Links ]
12. Torabinejad M, Handysides R, Khademi AA, Bakland LK. Clinical implications of the smear layer in endodontics: a review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002; 94:658-66. [ Links ]
13. Ørstavic D, Haapasalo M. Disinfection by endodontic irrigants and dressings of experimentally infected dentinal tubules. Endod Dent Traumatol 1990; 6:142-9. [ Links ]
14. Baumgartner JC, Mader CL. A scanning electron microscopic evaluation of four root canal irrigation regimens. J Endod 1987; 13:147-57. [ Links ]
15. Sedigheh K, Shokouhinejad N. Comparison of the efficacy of three chelating agents in smear layer removal. J Endod 2008; 34:599-602. [ Links ]
16. Hülsmann M, Heckendorff M, Lennon A. Chelating agents in root canal treatment: mode of action and indications for their use. Int Endod J 2003; 36:810-30. [ Links ]
17. Giovannone T, Foschi F, Nucci C, Ferrari M, Gallottini L. SEM evaluation of root canal walls after hybrid preparation with NiTi rotary instruments and four different irrigation techniques. Int Dent SA 2006; 8(1):38-47. [ Links ]
18. Williamson AE, Cardon JW, Drake DR. Antimicrobial susceptibility of mononuclear biofilms of a clinical isolate of Enterococcus faecalis. J Endod 2009; 35(1):95-7. [ Links ]
19. Lin Y, Mickel AK, Chogle S. Effectiveness of selected materials against Enterococcus faecalis: part 3. The antibacterial effect of calcium hydroxide and chlorhexidine on Enterococcus faecalis. J Endod 2003; 29:565-6. [ Links ]
20. Leonardo MR, Tanomaru Filho M, da Silva LAB, Nelson Filho P, Bonifacio KC, Ito IY. In vivo antimicrobial activity of 2% chlorhexidine used as a root canal irrigating solution. J Endod 1999; 25:167-71. [ Links ]
21. Gomes BPFA, Souza SFC, Ferraz CCR, Teixeira FB, Zaia AA, Valdrighi L, Souza-Filho FJ. Effectiveness of 2% chlorhexidine gel and calcium hydroxide against Enterococcus faecalis in bovine root dentine in vitro. Int Endod J 2003; 36:267-5. [ Links ]
22. Jeansonne MJ, White RR. A comparison of 2% chlorhexidine gluconate and 5.25% sodium hypochlorite as antimicrobial endodontic irrigants. J Endod 1994; 20:276-8. [ Links ]
23. Kuruvilla JR, Kamath MP. Antimicrobial activity of 2.5% sodium hypochlorite and 0.2% chlorhexidine gluconate separately and combined, as endodontic irrigants. J Endod 1998; 24(7):472-6. [ Links ]
24. Baca P, Mendoza-Llamas ML, Arias-Moliz MT, Gonzalez-Rodriguez MP, Ferrer- Luque CM. Residual effectiveness of final irrigation regimens on Enterococcus faecalis-infected root canals. J Endod 2011; 37:1121-3. [ Links ]
25. Wainwright M. Photodynamic antimicrobial chemotherapy (PACT). J Antimicrob Chemother 1998; 42:13-28. [ Links ]
26. Garcez AS, Núnez SC, Lage-Marques JL, Jorge AOC, Ribeiro MS. Efficiency of NaOCl and laser-assisted photosensitization on the reduction of Enterococcus faecalis in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 102:e93-8. [ Links ]
27. Haapasalo M, Ørstavic D. In vitro infection and disinfection of dentinal tubules. J Dent Res 1987; 66:1375-9. [ Links ]
28. Almyroudi A, Mackenzie D, McHugh S, Saunders WP. The effectiveness of various disinfectants used as endodontic intracanal medications: an in vitro study. J Endod 2002; 28:163-77. [ Links ]
29. Mohammadi Z, Shahriari S. Residual antibacterial activity of chlorhexidine and MTAD in human root dentin in vitro. J Oral Sci 2008; 50:63-7. [ Links ]
30. MacFarland J. The nephelometer: an instrument for estimating the number of bacteria in suspensions for calculating the opsonic index and for vaccines. J Am Med Assoc 1907; 49:1176. [ Links ]
31. Gerhardt P, Murray RGE, Costilow RN, Nester, EW, Wood,WA. Manual of methods for general bacteriology. Washington: American Society for Microbiology; 1981: 186-7. [ Links ]
32. Ferrari PHP, Cai S, Bombana AC. Effect of endodontic procedures on enterococci, enteric bacteria and yeasts in primary endodontic infections. Int Endod J 2005; 38:372-80. [ Links ]
33. Appelbe OK, Sedgley CM. Effects of prolonged exposure to alkaline pH on Enterococcus faecalis survival and specific gene transcripts. Oral Microbiol Immunol 2007; 22:169-74. [ Links ]
34. Bryce G, O'Donnell D, Ready D, Ng Y-L, Pratten J, Gulabivala K. Contemporary root canal irrigants are able to disrupt and eradicate single- and dual-species biofilms. J Endod 2009; 35:1243-8. [ Links ]
35. Hope CK, Burnside G, Chan SN, Giles LH, Jarad FD. Validation of an extracted tooth model of endodontic irrigation. J Microbiol Methods 2011; 84(1):131-3. [ Links ]
36. Tinaz AC, Karadag LS, Alaçam T, Mihçioglu T. Evaluation of the smear layer removal effectiveness of EDTA using two techniques: an SEM study. J Contemp Dent Pract 2006; 7:9-16. [ Links ]
37. Arruda M, de Arruda MP, de Carvalho JR, de Souza-Filho FJ, Sousa-Neto MD, de Freitas GC. Removal of the smear layer from flattened canals using different chemical substances. Gen Dent 2007; 55:523-6. [ Links ]
38. Saito K, Webb TD, Imamura GM, Goodell GG. Effect of shortened irrigation times with 17% ethylene diamine tetra-acetic acid on smear layer removal after rotary canal instrumentation. J Endod 2008; 34:1011-4. [ Links ]
39. Vianna ME, Gomes BP. Efficacy of sodium hypochlorite combined with chlorhexidine against Enterococcus faecalis in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009; 107(4):585-9. [ Links ]
40. Rôças IN, Siqueira JF. Comparison of the in vivo antimicrobial effectiveness of sodium hypochlorite and chlorhexidine used as root canal irrigants: a molecular microbiology study. J Endod 2011; 37:143-50. [ Links ]
41. Retamozo B, Shabahang S, Johnson N, Aprecio RM, Torabinejad M. Minimum contact time and concentration of sodium hypochlorite required to eliminate Enterococcus faecalis. J Endod. 2010; 36:520-3. [ Links ]
42. Jungbluth H, Peters C, Peters O, Sener B, Zehnder M. Physicochemical and pulp tissue dissolution properties of some household bleach brands compared with a dental sodium hypochlorite solution. J Endod. 2012; 38(3):372-5. [ Links ]
43. Ayhan H, Sultan N, Cirak M, Ruhi MZ, Bodur H. Antimicrobial effects of various endodontic irrigants on selected microorganisms. Int Endod J. 1999; 32(2):99-102. [ Links ]
44. Oliveira DP, Barbizam JV, Trope M, Teixeira FB. In vitro antibacterial efficacy of endodontic irrigants against Enterococcus faecalis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103(5):702-6. [ Links ]
45. Souza LC, Brito PRR, de Oliveira JCM, Alves FR, Moreira EJL, Sampaio-Filho HR. Photodynamic therapy with two different photosensitizers as a supplement to instrumentation/irrigation procedures in promoting intracanal reduction of Enterococcus faecalis. J Endod. 2010; 36 :292-6. [ Links ]
46. Soukos NS, Chen PS, Morris JT, Ruggiero K, Abernethy AD, Som S, Foschi F, Doucette S, Luschke Bammann L, Raquel Fontana C, Doukas AG, Stashenko PP. Photodynamic therapy for endodontic disinfection. J Endod. 2006; 32:979-84. [ Links ]
47. Foschi F, Fontana CR, Ruggiero K, Riahi R, Vera A, Stashenko PP. Photodynamic inactivation of Enterococcus faecalis in dental root canals in vitro. Lasers Surg Med. 2007; 39:782-7. [ Links ]
48. Schlafer S, Vaeth M, H0rsted-Bindslev P, Frandsen EVG. Endodontic photoactivated disinfection using a conventional light source: an in vitro and ex vivo study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 109:634-41. [ Links ]
49. Rios A, He J, Glickman GN, Spears R, Schneiderman ED, Honeyman AL. Evaluation of photodynamic therapy using a light-emitting diode lamp against Enterococcus faecalis in extracted human teeth. J Endod. 2011; 37:856-9. [ Links ]
 Correspondence:
Correspondence:
PJ van der Vyver
PO Box 2609, Cresta, 2118, Gauteng
South Africa
Tel: 011 781 1020
E-mail: peetv@iafrica.com

{kind=link}
{kind=link}
{kind=link}