










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.70 n.1 Johannesburg Feb. 2015
CASE BOOK
Oral medicine case book 66: Physiological/racial oral melanin hyperpigmentation
A MasilanaI; RAG KhammissaII; J LemmerIII; L FellerIV
IBSc, BDS. Department of Periodontology and Oral Medicine, University of Limpopo, Medunsa Campus, South Africa
IIBChD, PDD, MSc(Dent), MDent (OMP). Department of Maxillofacial and Oral Surgery, University of Limpopo, Medunsa Campus, South Africa
IIIBDS., HDipDent., FCD (SA) OMP., FCMSAae., Hon.FCMSA. Department of Periodontology and Oral Medicine, University of Limpopo, Medunsa Campus, South Africa
IVD. M. D, MDent (OMP). Department of Periodontology and Oral Medicine, University of Limpopo, Medunsa Campus, South Africa
ABSTRACT
Physiological/racial oral melanin hyperpigmentation is common, is seen more frequently in darker skinned persons and affects both males and females equally. It may involve any oral mucosal site, but particularly the gingiva, and usually develops during the first two or three decades of life, although many persons with this hyperpigmentation are unaware of its presence.
Physiological/racial oral melanin hyperpigmentation is brought about by increased melanogenic activity of a normal number of melanocytes in the basal cell layer of the oral epithelium. However, the intracellular molecular mechanisms and the intercellular and other micro-environmental signalling pathways that mediate this development are unknown.
Although no definitive relationship between oral mucosal melanoma and physiological/racial oral melanin hyperpig mentation has been demonstrated, and although in the vast majority of cases there should not be any cause for concern, nevertheless it has been observed that melanomas sometimes arise at sites of oral hyperpigmentations.
Key words: melanocytes, melanosomes, melanin.
INTRODUCTION
The normal colour of the oral mucosa is determined by several factors. These include the number, and the degree of melanogenic activity, of the melanocytes in the basal cell layer of the epithelium, the type and amount of melanin produced, the thickness of the epithelium, whether it is ortho or para-keratinized, the vascularity of the lamina propria and the haemoglobin content of the blood.1
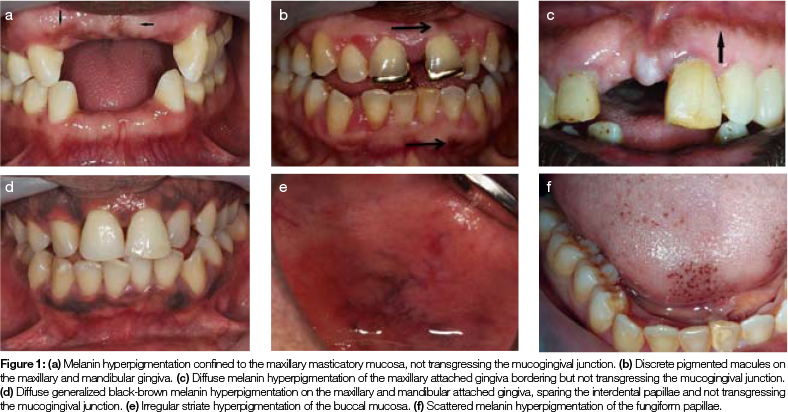
Physiological/racial oral melanin hyperpigmentation (POH) is common, is equally frequent in females and in males, usually develops during the first two decades of life, is asymptomatic, does not need treatment and occurs in all ethnic/racial groups. It is more prevalent in dark- than in light- skinned subjects,2 but the degree of oral mucosal pigmentation is not necessarily consistent with the degree of skin pigmentation.3 It can manifest as solitary or as multiple discrete macules, with either well-demarcated or ill-defined borders or as diffused generalised hyperpigmentation (Figure 1a-f).2,4-6 On the gingiva, the pigmentation may be quite extensive but is always confined by the muco-gingival junction. The pattern of distribution, the shape and the intensity of the POH are highly variable.2
There are similar numbers of melanocytes in the basal cell layers of the oral epithelia of persons with or without POH, and the development of POH can thus be attributed to genetically determined upregulation of melanogenic activity rather than to any increase in number of the melanocytes.2 The intensity and extent of POH may be influenced by endogenous and exogenous factors including hormones, neuropeptides, inflammation, drugs, tobacco smoke, and radiation.5,6
DISCUSSION
Melanosomes within the melanocytes in the basal cell layer of the epithelium are the sites of biosynthesis of melanin.7 The melanin-containing melanosomes are transported from the cytoplasm of the melanocytes to the ends of the specialised dendritic processes protruding from the cell membrane of the melanocytes. From thence the transported melanosomes are subsequently transferred through the cell membrane to the neighbouring keratinocytes, and the complex of melanocytes which produce, and keratinocytes which receive, the melanin are referred to as the 'keratinocyte-melanin unit'.2 In the skin, within the keratinocytes, the melanin forms protective supranuclear 'caps' shielding the nuclear DNA from ultraviolet radiation.8 Whether there is any such phenomenon in the oral keratinocytes which are not exposed to ultraviolet radiation is unknown.
Melanin biosynthesis is regulated by a complex interaction between multiple biological mediators. Adrenocorticotrophic hormone (ACTH), α-melanocyte stimulating hormone (α-MSH), β-endorphins, prostaglandins, endothelin-1, histamine and oestrogen are some of the agents in the microenvironment which have the capacity to stimulate production of melanin; while melatonin, glucocorticoids, and some cytokines can inhibit melanin biosynthesis.9
Keratinocytes appear to have some control over the regulation of skin and oral mucosal melanin pigmentation as they have the capacity to produce and to secrete ACTH, α-MSH, β-endorphins and endothelins; and also to have some influence over the transfer of melanosomes from the melanocytic dendritic processes to the keratinocytes of the keratinocyte-melanin unit of which they themselves are a part.10
Besides their role in influencing the colour of skin, hair and eyes, melanin has the capacity to neutralize reactive oxygen species and free radicals in the local microenvironment and to neutralize bacteria-derived enzymes and toxins, to sequester metal ions, and to bind to organic molecules, thus acting as a physical barrier against microorganisms. As keratinocytes ascend through the cell layers of the oral epithelium to desquamate at the surface, melanosomes within the keratinocytes disintegrate releasing melanin 'dust' that protects the oral mucosa against microbial toxins and other microenvironmental stressors.8
The population of melanocytes of the oral epithelium appears to be more or less constant throughout life, despite the fact that some melanocytes are lost owing to the natural process of programmed cell death, and to mechanical, thermal or chemical injury. The mechanism by which the population of oral melanocytes is maintained in a steady state is unknown and the location of the reservoirs of undifferentiated melanocytes stem/progenitor cells containing the genetic information and the regenerative capacity of the oral melanocyte population is obscure. However, since there is clearly a source of melanocyte stem/progenitor cells capable of maintaining a stable number of oral epithelial melanocytes, such a niche reservoir of melanocyte stem/progenitor cells must exist.
COMMENTS
- Further research is needed into why most POH develops in the first two or three decades of life and thereafter diminishes; and into whether POH plays any role in maintaining the homeostasis of the oral epithelium and lamina propria.
- It is not possible to differentiate between a melanotic macule and POH manifesting as a solitary macule or as multiple discrete melanotic macules, because of the clinical and microscopical similarities of these two entities. This naturally leads one to question whether these two 'entities' exist separately.
- Although up to thirty percent of oral mucosal melanomas develop at sites previously affected by melanin hyperpigmentation,11-13 and although in most cases the nature of the hyperpigmented pre-melanoma cases has not been determined, there must be concern about any POH being a potential site for future melanoma.
- Although both POH and oral mucosal melanoma most frequently affect the gingiva, the biopathological significance of this is unknown.
ACRONYMS
ACTH: Adrenocorticotropic hormone
α-MSH: α-melanocyte stimulating hormone
POH: Physiological oral hyperpigmentation
References
1. Dummett CO. Physiologic pigmentation of the oral and cutaneous tissues in the Negro. J Dent Res 1946;25:421-32. [ Links ]
2. Chandra S, Keluskar V, Bagewadi A, Sah K. Extensive physiologic melanin pigmentation on the tongue: An unusual clinical presentation. Contemp Clin Dent 2010;1:204-6. [ Links ]
3. Gaeta GM, Satriano RA, Baroni A. Oral pigmented lesions. Clin Dermatol 2002;20:286-8. [ Links ]
4. Caldeira PC, de Sousa SF, Gomez RS, Silva TA. Diffuse pigmentation of the oral mucosa. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:550-3. [ Links ]
5. Eisen D. Disorders of pigmentation in the oral cavity. Clin Dermatol 2000;18:579-87. [ Links ]
6. Meleti M, Vescovi P, Mooi WJ, van der Waal I. Pigmented lesions of the oral mucosa and perioral tissues: a flow-chart for the diagnosis and some recommendations for the management. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:606-16. [ Links ]
7. Kauzman A, Pavone M, Blanas N, Bradley G. Pigmented lesions of the oral cavity: review, differential diagnosis, and case presentations. J Can Dent Assoc 2004;70:682-3. [ Links ]
8. Feller L, Masilana A, Khammissa RA, Altini M, Jadwat Y, Lemmer J. Melanin: the biophysiology of oral melanocytes and physiological oral pigmentation. Head Face Med 2014;10:8. [ Links ]
9. Slominski A, Wortsman J, Plonka PM, Schallreuter KU, Paus R, Tobin DJ. Hair follicle pigmentation. J Invest Dermatol 2005;124:13-21. [ Links ]
10. Hirobe T. Role of keratinocyte-derived factors involved in regulating the proliferation and differentiation of mammalian epidermal melanocytes. Pigment Cell Res 2005;18:2-12. [ Links ]
11. Lourenco SV, Bologna SB, Hsieh R, Sangueza M, Fernandes JD, Nico MM. Establishment and characterization of an oral mucosal melanoma cell line (MEMO) derived from a longstanding primary oral melanoma. Am J Dermat-opathol 2013;35:248-51. [ Links ]
12. Mohan M, Sukhadia VY, Pai D, Bhat S. Oral malignant melanoma: systematic review of literature and report of two cases. Oral Surg Oral Med Oral Pathol Oral Radiol 2013;116:e247-54. [ Links ]
13. Tlholoe MM, Khammissa RA, Bouckaert M, Altini M, Lemmer J, Feller L. Oral mucosal melanoma: some pathobiological considerations and an illustrative report of a case. Head Neck Pathol 2014. [ Links ]
 Correspondence
Correspondence
L Feller
Head: Dept. Periodontology and Oral Medicine
Box D26 School of Dentistry
MEDUNSA 0204
South Africa
Tel: 012 521 4834
E-mail: liviu.feller@ul.ac.za

{kind=link}