










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.70 n.1 Johannesburg Feb. 2015
RESEARCH
Comparison of colour components between maxillary central incisors - an in vivo study
DS MoodleyI; SR GroblerII; Yl OsmanIII; TJvW KotzeIV
IBDS, MSc (Dent), PDD (Aesthetic Dent), PhD(Restorative Dent).Department of Restorative Dentistry, Faculty of Dentistry, University of the Western Cape, Tygerberg, South Africa
IIBSc, BSc(Hons), MSc(Phys. Chem), DSc(Chem), PhD(Dent).Oral and Dental Research Institute, Faculty of Dentistry, University of the Western Cape, Tygerberg, South Africa
IIIBChD, MChD, Hons BBA, MBA, PGDHM.Department of Restorative Dentistry, Faculty of Dentistry, University of the Western Cape, Tygerberg, South Africa
IVBSc, MSc(Stats), DSc(Stats). Oral and Dental Research Institute, Faculty of Dentistry, University of the Western Cape, Tygerberg, South Africa
ABSTRACT
OBJECTIVES: The purpose of this study was to determine the relationship of colour in the CIE L*a*b* scale between the maxillary central incisors.
METHODS: The colour of the maxillary central incisors of 83 patients was measured (in vivo) using a spectrophotometer. Three measurements (6 mm diameter) at the centre of the crown of each of the maxillary central incisors were performed.
RESULTS: The total colour difference (∆E*ab) showed wide variability with the average ∆E*ab = 1.79. The Wilcoxon Signed Rank Test showed statistically significant differences (p < 0.05) between maxillary right (11) and left central incisors (21) in both the L* and b* colour components. In the a* scale no significant difference was noted.
CONCLUSION: Small colour differences exist between the maxillary central incisors in the same individual when evaluated with a spectrophotometer.
CLINICAL SIGNIFICANCE: As there is often a difference between the colours of the two central incisors in the same patient, the colour of both the central incisors should be taken into consideration when shade matching anterior teeth.
Key words: Colour, incisors, spectrophotometer, L*a*b*, CIELAB.
INTRODUCTION
In clinical dentistry colour matching of teeth is already a challenging task but as the aesthetic demands and expectations of patients escalate, so will there be an increasing need to achieve accuracy.1,2 Hence, precise colour matching, and obtaining a base line colour, especially of the anterior teeth, is critical for success in aesthetic dentistry. Currently, some of the major problems with colour matching are due to the subjective nature of the procedure, or as a result of operator variability, the limitations of shade guide tabs that do not fully represent the colour space of natural teeth, polychromaticity of teeth, lighting conditions, wetness/ dryness of teeth and/ or variations in the texture of the tooth surface.3
Tooth colour selection can be performed using either visual shade matching or instrumental colour analysis. Visual shade matching is affected by many factors, such as surrounding illumination and conditions, physiological variables of the operator including age, metamerism and the method used.4,5 These limitations can lead to inaccurate colour matching when relying on shade guides, and can result in dissatisfaction of patient, technician and clinician.6
Commercial digital cameras have been proposed as a means of tooth shade matching.7 However, the image quality is dependent on many factors and can vary depending on the type of camera, the camera settings, lighting conditions, size of the image captured, the relative position of teeth, and shade guides.1 Furthermore, the interpretation of tooth colour using a digital photograph is highly dependent on the individual and can be subjective and often in-accurate.1 Recently, various numerically-based instruments such as the spectrophotometer and the colorimeter have become available. These colour-measuring devices are reportedly more effective, uniform and accurate in quantifying the natural tooth colour, thus enabling improved communication between technicians and dentists.7 Better results can be achieved if both the dentist and the technician calibrate the spectrometer.
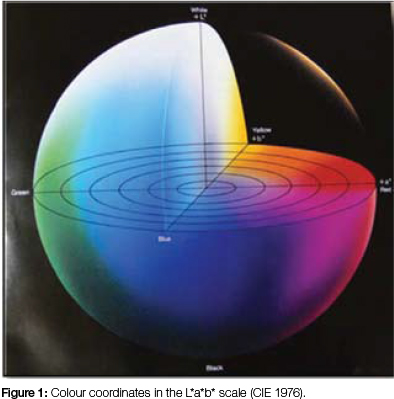
The two main colour measuring processes are the Munsell Colour Order System and the CIE System (Commission In-ternationaie de i' Eclairage or International Commission on Illumination).8 The CIE system relies on wavelengths to define a uniform colour space based on tristimulus values (i.e. three spectral stimuli received by the three types of cone cells in the eye and as perceived by a standardized observer). This was further expanded in 1976 to become the CIE L*a*b* system (Figure 1). In this system the L* axis is lightness/brightness, is defined as the perceived brightness, ranging from black to white, and measured on a scale from 0 (black) to 100 (white). The a* value gives the quantity of green (if negative) or red (if positive). The b* value describes the quantity of blue (if negative) or yellow (if positive). CIE L*a*b* allows for quantification of colour differences between objects. The delta values associated with this colour scale, ∆L*, ∆a*, and ∆b,* indicate by how much a standard and a sample differ from one another in the L*, a*, and b* scale.
The apparent colour of a tooth is dependent on the structure of the tooth i.e. thickness of the enamel layer, which will, through absorption or scattering, modify the amount of light reflected from the dentin.9 A number of factors may affect shade selection, including specular transmission of light through the tooth; specular reflection at the surface; diffuse light reflection at the surface; absorption and scattering of light within the dental tissues; enamel mineral content; enamel thickness; dentine colour,and the presence of extrinsic and intrinsic stains as well as surface texture, wetness of the surface and contour.9,10,11,13,14,15
Differences in tooth colour exist among people, among different teeth in the same person9 and within the same tooth.10 Colour varies in the same tooth with a gradual decrease in lightness from incisal to cervical area11 making colour matching of teeth even more complicated. The cervical area of the tooth may appear either reddish or yellowish, being either affected by gingival pink for redness, or yellowness from root colour if covered by a thin layer of enamel.10 Hence, Schwabacher and Goodkind12 suggested that during colour matching of maxillary anterior teeth, the best representation will be in the middle third of the crown.
Tooth colour differences have been reported between central incisors and canines,13,14 between maxillary incisors and mandibular incisors15 as well as varying with age11,13 and gender,15 but to our knowledge no studies have been done comparing the colours of the two maxillary central incisors. Specifically, it has not been determined whether the maxillary right and left central incisors actually do occupy the same colour space in the CIE L*a*b* scale.
Therefore, the aim of this study was to determine the relationship of colour components in the CIE L*a*b* scale of the two maxillary central incisors within the same patient, to determine whether or not they occupy the same colour space.
MATERIALS AND METHODS
Eighty three randomly selected patients aged between 17 and 25 years took part in this study. Inclusion criteria were that they had to have both permanent central incisors present, that teeth were free of any caries or restorations, absence of fluorosis, intrinsic or extrinsic staining and had not previously been subjected to any tooth whitening procedures. Prior to colour recording, the teeth were polished using a rubber cup (Nu-PRO Disposable Prophy Angle; Dentsply Intl; USA) and a slurry of pumice (Nu-PRO Prophylaxis Paste; Dentsply Intl; USA), flowed by rinsing with water and finally blot drying. A spectrophotometer (Model: CM-2600d, Konica Minolta Sensing, Inc., Japan) was set on the CIE L*a*b* colour space and calibrated as outlined by the manufacturer. The colour of the maxillary central incisors, (11 and 21) was recorded at the centre of the crown using a six mm diameter probe. Three measurements of this area were performed on each of the two teeth. The average of the three readings was calculated and recorded for statistical analysis. Multiple factors were then analyzed in terms of the colour matching process using the CIELAB8 colour coordinates as shown in Figure 1 and described using the following calculations:8
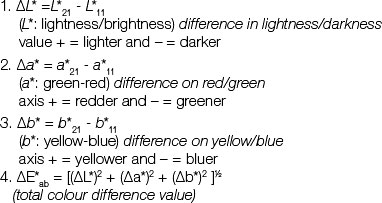
∆L*, ∆a* and ∆b* are the mathematical differences in the L*, a* and b* components of the CIE LAB scale between the readings on the upper right and upper left central incisors. The ∆E*ab was then determined as the mathematical difference in colour between the two central incisors, permitting a precise numerical definition of the magnitude of that dif-ference.16 The CIE L*a*b* values were then plotted in a 3-di-mensional graph (Image J software 1.47v; National Institute of Health, USA), enabling visual comparisons.
STATISTICAL ANALYSIS
The data was analyzed using a statistical software package NCSS 2007 (NCSS, LLC, Kaysville, UT, USA). The L*, a* and b* values and the total colour differences for the central incisors were compared using the Wilcoxon Signed Rank Sum Test with the level of significance set at p<0.05.
RESULTS
The Wilcoxon Signed Rank Test showed statistically significant differences between maxillary right (11) and left central incisors (21) in both the L* and b* colour components (Table 1).
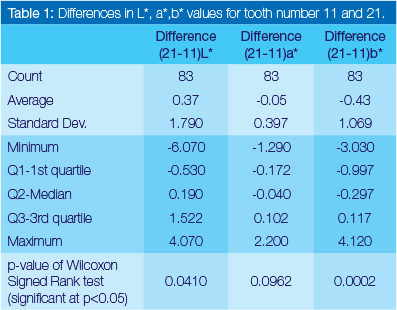
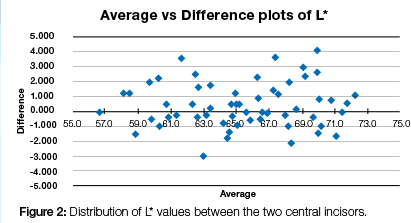
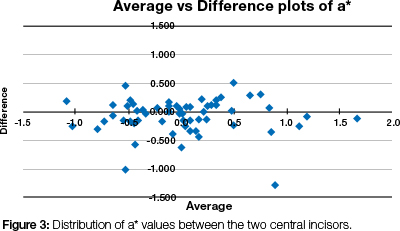
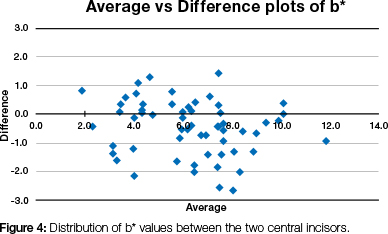
In the L* (lightness/brightness) scale, about 50% of the individuals showed differences between the two central incisors. In the a* scale i.e. green/red range, no significant difference was found, but, in the b* scale, about 37% of the individuals showed a difference between the two central incisors i.e. in the yellow/blue range, with the values for 11 being the larger (Figures 2, 3 and 4). Calculation and analysis of the ∆E*ab values revealed a wide range (coefficient of variation 70.7%), suggesting that there is a disparity in the colour differences between the two central incisors. The average ∆E*ab was 1.79 (standard deviation 1.26) with 70.6% of the individuals having an ∆E*ab > 1, while 14% of the individuals showed a ∆E*ab > 3.
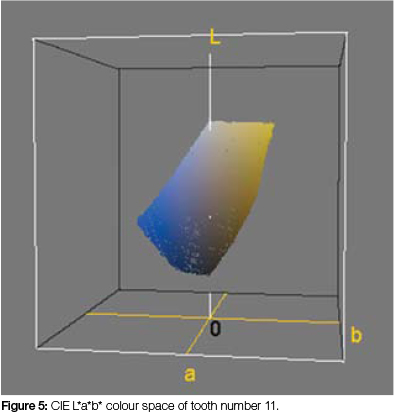
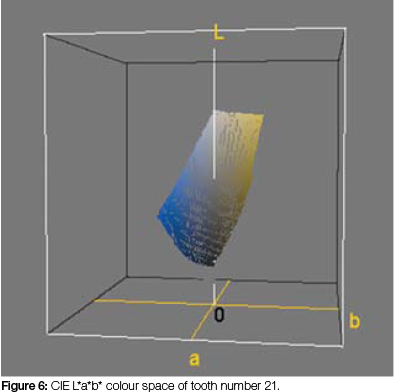
CIE L*a*b* mean values plotted using the software : Image J 1.47v (National Institute of Health, USA) show the colour space of teeth number 11 (Figure 5) and of teeth number 21 (Figure 6) within a 3D-representation. It may be observed that tooth numbers 11 and 21 indeed do not occupy the same colour space in the CIE L*a*b* colour system.
DISCUSSION
Colour matching of natural maxillary central incisors is one of the most difficult challenges in clinical dentistry.1 A colour-measuring device that produces constant values under any given condition may thus be the ideal means to achieve re-peatable and consistent measurements.7 The advantage of the spectrophotometer is that it is not affected by ambient light, and the amount of light reflected from objects is measured over a full spectral wavelength1 whereas the colorimeter measures light only in the red/green/blue (RGB) scale. The spectrophotometer provides consistent shade measurement regardless of light conditions or operator variabil-ity17. Hence, in order to avoid errors arising from subjectivity and the inaccuracies of shade-matching guides, the spec-trophotometer (Konica, Minolta) set in the CIE L*a*b* colour space was used in this study.
Our findings demonstrated that when comparing the maxillary central incisors (∆E*ab) in each individual patient, there is an overall difference in colour in the L*a*b* scale. Significant differences in colour components between the two central incisors were observed in both the L* and b* scales (p<0.05).
The distribution of the differences in L* values (Figure 2) tends towards the positive side indicating a wide distribution of the L* values above the zero line suggesting a higher difference in the lightness/brightness of both the central incisors. The a* values (Figure 3) show much closer grouping along the zero line suggesting not much of a difference between the two central incisors in the red/green scale. The distribution of b* values is more on the negative side i.e. tooth number 11 having larger b* values than tooth number 21 (Figure 4). There is a much wider distribution of the b* values suggesting a wider variation in the yellow/blue scale between the two central incisors. The larger b* values indicate a more yellowish scale is seen on tooth number 11 than on tooth number 21.
The ΔE*ab equation in the L*a*b* scale enables the quantitative comparison of colour differences among teeth. The clinical significance of ∆E*ab in terms of both "perceptibility" and "acceptability" have been studied by various research-ers.18,19,20 Whilst there is no clear indication at which value a difference (ΔE*ab) between teeth would be discernible by the human eye, it has been reported that a ΔE*ab value of 1 or higher could be perceived by the human eye when industrial colours were being observed.21 A study on colour differences of composites showed, however, that ∆E*ab has to approach 3.3 before the human eye can detect a colour difference,18 while a difference of only 0.7 ΔE*ab units was perceptible when observers compared porcelain discs.22 Douglas and Brewer22 reported that 50% of the prosthodontists in their study rejected a shade match for metal-ceramic crowns when the mean colour difference for ∆E*ab was 1.7. In the current study the mean colour difference (∆E*ab) between the observed natural teeth was 1.79, a comparatively low value. At present there is no consensus in the dental literature as to how much colour difference is considered acceptable, even as a mismatch, nor how much of a colour difference is perceptible to the observer.16 No significant colour differences of the maxillary central incisors were reported by Hayward et al.23and Grobler et al.24,26,26in their studies on the effect of various bleaching agents on tooth colour. This may possibly be as a result of the small sample size (n<21) used in their project. Dozic et al27have, however, reported variations in colour within the same tooth.
The precision of the differences in this study using a spec-trophotometer will enable comparison with values obtained when assessing colour spaces on other materials like porcelain discs22, metal-ceramic crowns22 and industrial colours.21
Hence, a follow up study could be designed to determine whether these differences are detected by the human eye.
A null hypothesis on which this study could have been based would state that no significant differences in colour in the CIE L*a*b* scale exist between the upper two anterior teeth in the same individual. That hypothesis would be rejected. Thus, inter-arch shade variation exists not only between central incisors and canines10,13,16,28 but as shown in this study, colour variation may exist between the maxillary central incisors in the same patient.
CONCLUSION
1. Differences within the colour components of maxillary central incisors exist. Spectrophotometer analysis has shown in this study that small colour differences (∆E*ab) do occur between central incisors in the L*a*b* scale in the same individual.
2. The colour of central incisors showed significant differences in both the lightness/brightness (differences in the L* values in 50% of the individuals) and on the blue/ yellow scale (differences in the b* values in 37% of the individuals).
CLINICAL SIGNIFICANCE
During shade matching procedures the colour of both central incisors should be taken into consideration to establish a base line. This is especially applicable prior to tooth whitening and shade matching in aesthetic restorative procedures where the random use of either one of the two central incisors is not advocated.
Ethical statement: Ethical clearance was obtained from the Senate Research Committee, University of the Western Cape.
Acknowledgement: Financial support was received from the South African Dental Association.
Declaration: No conflict of interest was declared.
ACRONYM
CIE System: Commission Internationale de l' Eclairage or International Commission on Illumination
References
1. Ishikawa-Nagai S, Yoshida A , Da Silva JD, Miller L. Spectro-photometric analysis of tooth colour reproduction on anterior all-ceramic crowns: Part 1: Analysis and interpretation of tooth colour. J Esthet Rest Dent 2010;22:42-62. [ Links ]
2. Dancy WK, Yaman P, Dennison JB, O'Brien WJ, Razzoog ME. Colour measurements as quality criteria for clinical shade matching of porcelain crowns. J Esthet Rest Dent 2003;16(2):114-22. [ Links ]
3. Brewer JD, Wee A, Seghi R. Advances in colour matching. Dent Clin North Am 2004;48:341-68. [ Links ]
4. Park JH, Lee YK, Lim BS. Influence of illuminants on the colour distribution of shade guides. J Prosthet Dent 2006;96:402-11. [ Links ]
5. Cho BH, Limb YK, Lee YK. Comparison of the colour of natural teeth measured by a colorimeter and Shade Vision System. Dent Mater 2007;23:1307-12. [ Links ]
6. Yuan JCC, Brewer JD, Monaco EA, Davis EL. Defining a natural tooth colour space based on a 3-dimensional shade system. J Prosthet Dent 2007;98:110-9. [ Links ]
7. Odaira C, Itoh S, Ishibashi K. Clinical evaluation of a dental colour analysis system: The Crystal eye Spectrophotometer. J Prosthet Research 2011;66: 199-206. [ Links ]
8. Commission Internationale de l'Eclarirage (CIE). Recommendations on uniform colour spaces, colour difference equations, psychometric colour terms. Supplement No. 2 of publication CIE No. 16 (E-1.3.1) ed. Paris: Bureau Central de la CIE; 1978. [ Links ]
9. Pustina-Krasniqi T, Pustina B. The correlation of colour in the maxillary central incisors. Digital Dental News 2012; 6-11. [ Links ]
10. Goodkind RJ, Keenan K, Schwabacher WB. Use of fiber-optic colorimeter for in vivo colour measurement of 2830 anterior teeth. J Prosthet Dent 1987;68:636 - 642. [ Links ]
11. Hasegawa A, IIkeda I, Kawaguchi S. Colour and translucency of in vivo natural central incisors. J Prosthet Dent 2000;83:418-23. [ Links ]
12. Schwabacher WB, Goodkind RJ. Three-dimensional colour coordinates of natural teeth compared with three shade guides. J Prosthet Dent 1990;64:426-31. [ Links ]
13. Eiffler C, Cevirgen E, Helling S, Zornek J, Pritsch M, Hassel AJ. Differences in lightness, chroma, and hue in the anterior teeth of quinquagenarians and septuagenarians. Clinical Oral Investigations 2010;14:587-91. [ Links ]
14. Dozic A, Kleverlaan CJ, Aartman IHA, Feilzer AJ. Relation in colour among maxillary incisors and canines. Dent Mater 2005;21:187-91. [ Links ]
15. Tuncdemir AR, Polot S, Ozturk C, Tuncdemir MT. Colour differences between maxillary and mandibular incisors. Europ J Gen Dent 2012; 1(3): 170-3. [ Links ]
16. Douglas DR, Steinhauer TJ, Wee AG. Intraoral determination of the tolerance of dentists for perceptibility and acceptability of shade matching. J Prosthet Dent 2007;97:200-8. [ Links ]
17. Goldstep F, Freedman G. Colour and Shade. In: Freedman G, editor. Contemporary Esthetic Dentistry. PA: Elsevier;2012.135-67. [ Links ]
18. Ruyter IE, Niler K, Moller B. Colour stability of dental composite resin materials for crowns and bridge veneers. Dent Mater 1987;3:246-51. [ Links ]
19. Seghi RR, Hewlett ER, Kim J. Visual and instrument colorimetric assessments of small colour differences on translucent dental porcelain. J Dent Res 1989;68:1760-4. [ Links ]
20. Lindsey DT, Wee AG. Perceptibility and acceptability of CIE-LAB colour differences in computer-simulated teeth. J Dent 2007;35:593 -9. [ Links ]
21. Kuehni RG, Marcus RT. An experiment in visual scaling of small colour differences. Colour Research and Application 1979;4:83-91. [ Links ]
22. Douglas RD, Brewer JD. Acceptability of shade differences in metal ceramic crowns. J Prosthet Dent 1998;79:254-60. [ Links ]
23. Hayward R, Osman Y, Grobler SR. A clinical study of the effectiveness of a Light Emitting Diode system on tooth bleaching. The Open Dent J 2012;6:51-5. [ Links ]
24. Grobler SR, Majeed A, Hayward R, Rossouw RJ, Moola ML, van W Kotze TJ. A clinical study of the effectiveness of two different 10% carbamide peroxide bleaching products: a 6-month follow up. Int J Dent 2011a, Article ID 1675250, 5 pages doi:10.1155/2011/167525. [ Links ]
25. Grobler SR, Majeed A, Moola MH, Rossouw RJ, van W Kotze TJ. in vivo spectrophotometric assessment of the tooth whitening effectiveness of Nite White 10% with amorphous calcium phosphate, potassium nitrate and fluoride, over a 6-month period. Open Dent J 2011b;2:18-23. [ Links ]
26. Grobler SR, Hayward R, Wiese S, Moola MH. Spectrophotomet-ric assessment of the effectiveness of Opalescence PF 10%. A 14-month clinical study. J Dent 2010;38:113-7. http://dx.doi.org/10.1016/j.jdent.2009.09.009. [ Links ]
27. Dozic A, Kleverlaan CJ, Aartman IHA, Feilzer AJ. Relation in colour of three regions of vital human incisors. Dent Mater 2004;20:832-8. [ Links ]
28. Kim TJ, Kwon KR, Kim HS, Woo YH. A study of the shade between maxillary and mandibular anterior teeth in the Korean. J Korean Acad Prostho 2008;46(4):343-50. [ Links ]
 Correspondence:
Correspondence:
DS Moodley
Department of Restorative Dentistry
Faculty of Dentistry
University of the Western Cape
Private Bag X1
Tygerberg 7505
Cape Town
South Africa
Fax:+27 21 937 3024. Tel:+27 21 937 3090
E-mail:dmoodley@uwc.ac.za
