










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.69 no.10 Johannesburg Nov. 2014
CLINICAL REVIEW
A novel use of the Reciproc R25 Endodontic file for root canal obturation
I Cassim
(BDS (Wits), PG Dip Dent (Endo) (Cum Laude),MSc (Fret). Private practice: 1 Riverside Mews, 3 Ridgeside Road, Umgeni Park, Durban North 4051, South Africa. Tel: 031 709 3080. Fax: 031 710 7438. Cell: 084 657 5557. Email: ijcassim@worldonline.co.za
INTRODUCTION
Thermo-mechanical compaction of gutta-percha was first described by Mcspadden in 19801. This involved the use of McSpadden compactors (Dentsply/Maillefer, Bellaigues, Switzerland) which are stainless steel inverted hedstrom files with a 2% taper. In this technique, the use of McSpadden's compactors at 20 000 rpm produces friction between the gutta-percha and the internal walls of the root canal, leading to the thermo-plasticising of gutta-percha. The gutta-percha is moved apically and laterally due to the orientation of the blades of the McSpadden compactors.2 When a Reciproc file (VDW, Germany) is used in clockwise rotary motion, any substance engaged by the flutes of the blades is, similarly, driven apically and laterally.
The use of Reciproc endodontic instruments in thermo-mechanical compaction during obturation has not previously been described in the literature.
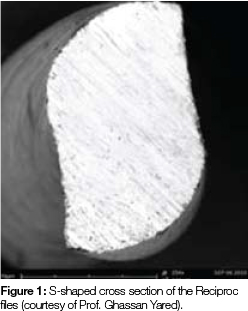
The Reciproc file system (VDW, München, Germany) was developed by Prof. Ghassan Yared and launched in 2011. The system consists of three files: the R25 which has an ISO tip size 25 and an 8% taper in the apical 3mm and the taper decreases to D16 (diameter of 1.05mm); the R40 has an ISO tip size 40 and a 6% taper in the apical 3mm and the taper decreases to D16 (diameter of 1.1mm) ; the R50 has an ISO tip size 50 and a 5% taper in the apical 3mm and the taper decreases to D16, (diameter of 1.17).3 The files are manufactured from M-Wire which has been shown to be more flexible, stronger and more resistant to cyclic fatigue compared with traditional nickel-titanium instruments.4,5 The cross section of the files is S-shaped (Figure 1) for greater flexibility, more efficient cutting and channelling of debris. The blades are non-landed and are designed to cut in a counter-clockwise direction with asymmetric reciprocating motion. The routine use of the Reciproc files has been described in initial endodontic treatment and in non-surgical retreatment.3,6-8
Thermo-mechanical compaction should not be used for condensing gutta-percha in teeth with wide open, resorbed or perforated apices as this can lead to gross extrusion of the root filling.
Important guidelines for the use of Reciproc files for thermo-mechanical compaction:
a) straight line access to the coronal third of the root canal should be confirmed, especially in the mesial roots of upper and lower molars;
b) tapered preparation is required to a minimum of a size 25, 6% or size 30, 4%;
c) gutta-percha points with a minimum 4% taper should be used;
d) i t is essential to confirm tug back of the gutta-percha point in the apical part of the prepared root canal;
e) a minimal amount of root canal sealer should be used (Figure 2);
f) the gutta-percha cone should be cut at least 3 to 5mm above the orifice level;
g) the file should be used in a contra-angle hand piece, inserted into the gutta percha cone and used at 20 000 rpm;
h) the file should be inserted to a depth of only 5mm beyond the orifice, which can be pre-measured and the rubber stopper adjusted on the file;
i) the duration of compaction should be a maximum of 5 seconds;
j) i n oval canals or when more than one gutta-percha cone is used, a slight pumping and lateral motion can be used to compact the gutta percha cones;
k) the rotating file should be removed along the outer wall of the canal; and
l) a gutta-percha plugger eg. Machtou plugger (Dentsply/ Maillefer) can be used to vertically condense the plasti-cised gutta-percha mass.

CASE REPORT 1
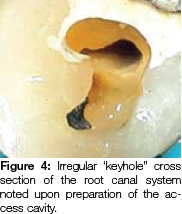
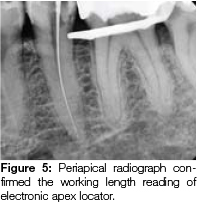
A 66-year old male patient was referred for endodontic treatment and restoration of his lower left second premolar, after he presented with acute irreversible pulpitis and acute apical periodontitis. Radiographic evaluation revealed that the decay had exposed the pulp and that the tooth had a single root canal system (Figure 3a and 3b). An irregular 'keyhole" cross section of the coronal root canal system was observed during access cavity preparation (Figure 4). Working length was determined using the I-pex apex locator (NSK, Nakanishi, Japan) and confirmed with a periapical radiograph (Figure 5). The canal was prepared with the Reciproc R25 (VDW) and, following apical gauging, the canal was enlarged to a 35, 4% taper using the BT3 Race file (FKG Dentaire, Switzerland). During instrumentation, the canal was irrigated with 3.5% sodium hypochlorite (Jik, Reckert-Benkieser, South Africa). The Endovac (Axis/Sybron, Coppel, Texas) apical negative pressure irrigation system was used to optimise the volume of irrigant delivered through the root canal system. Ultracal (Ultradent, Utah, USA), a non-setting calcium hydroxide was used as an inter-appointment medicament in the root canal.

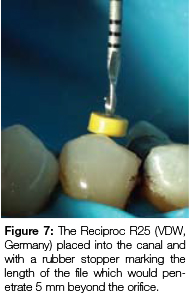
At the second visit, the medicament was removed and the irrigation regime as above was resumed. An additional final rinse of a 17% EDTA and cetrimide combination (Smear Clear, Axis/Sybron, Coppel, Texas) was used to remove the smear layer. A size 35, 4% tapered gutta-percha cone (Diadent, Korea) was tested for fit and tug back confirmed. A "cone fit" radiograph was taken to confirm the seating of the gutta-percha cone (Figure 6), The Reciproc FÍ25 file (VDW, Germany) was seated to the orifice and a rubber stopper used to mark the depth (Figure 7). The stopper was then adjusted to a depth of 5mm beyond the level of the orifice.

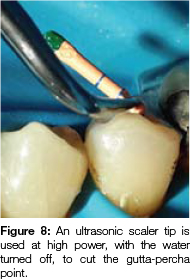
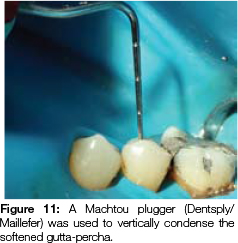
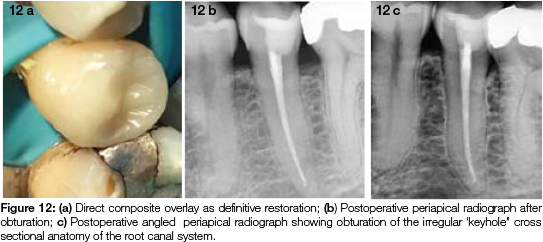
The canal was dried with the Endovac (Axis/Sybron) and paper points. The gutta-percha cone was coated with AH plus sealer (Dentsply/Maillefer) and seated in the canal. The gutta-percha cone was cut off at 4mm above the orifice using an ultrasonic scaler tip at full power with the water turned off (Figure 8). The Reciproc R25 instrument was placed in a 1:1 contra angle blue ring hand piece, and positioned alongside the gutta-percha coronally. The hand piece was turned on at 20 000 rpm and the file pushed apically (Figure 9) to a depth 5mm below the orifice level for 3 seconds and then withdrawn along the wall of the canal. Some of the condensed gutta-percha mass remained embedded in the flutes of the file once it was removed (Figure 10). A size 2 Machtou plugger (Dentsply/Maillefer) was used to condense the softened gutta-percha mass (Figure 11). The tooth was restored with a direct composite overlay and post operative radiographs show the obturation of the irregular cross sectional anatomy (Figures 12 a-c).


CASE REPORT 2
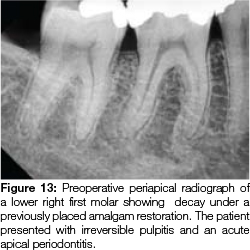
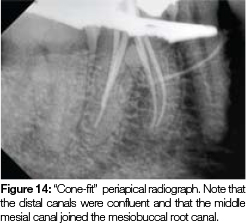
A 36-year old male patient was referred for endodontic treatment of his lower right first molar after he presented with irreversible pulpitis and an acute apical periodontitis. Radiographic examination revealed a previously placed amalgam restoration with secondary decay on the distal aspect of the tooth (Figure 13). An access cavity was prepared and five root canal orifices were located. The canals were shaped with the Reciproc R25 (VDW). The two distal canals were confluent after shaping, and formed a ribbon shaped cross section. The middle mesial canal joined the mesiobuccal canal 4mm below the orifice. A combination of 3.5% sodium hypochlorite (Jik, Reckert-Benkieser, South Africa) and Smear Clear (Axis/Sybron) solutions were used for root canal irrigation. The irrigants were agitated by active ultrasonic agitation using a size 15 NSK U-file (NSK, Nakanishi, Japan). Irrigation was further optimised in the mesial root canal system, by synchronous use of the Endovac System (Axis/Sybron) and irrigant delivery through a 31 gauge Navitip sideport needle (Ultradent,Utah, USA) in the adjacent root canal. A "cone fit" radiograph with corresponding R25 Gutta-percha cones (VDW, Germany) was taken after shaping of the canal (Figure 14). The gutta-percha cones were coated with AH plus sealer (Dentsply/Maillefer) and placed in the prepared root canals.The gutta-percha was cut off above the level of the orifice, using an ultrasonic tip. The Reciproc R25 was placed in a 1:1 contra angle blue ring hand piece and placed in the distal orifice along the lingual wall adjacent to the gutta-percha. The hand piece was turned on at 20 000 rpm and the file pushed apically to 5mm below the orifice for 3 seconds in the distal canal and then in a light pumping motion the file was moved in and out laterally from lingual to buccal and withdrawn along the buccal wall. The gutta-percha was then condensed with the size 3 Machtou plugger (Dentsply/Maillefer). The confluent middle mesial and mesiobuccal canals were compacted in a similar manner. In the mesiolingual canal the gutta-percha was cut 2mm above the orifice and the Reciproc R25 was placed adjacent to the gutta-percha lingually and the handpiece turned on at 20 000 rpm. The file was pushed apically to 5mm below the level of the orifice for 3 seconds and the file withdrawn along the lingual wall. Straight and distal angulated periapical radiographs taken after obturation demonstrated the three dimensional obturation of the ribbon shaped distal root canal system and the anastomosis between the canal systems in the mesial root (Figures 15a and 15b). The patient was referred back to his dentist for a permanent coronal restoration with cuspal coverage.


CASE REPORT 3
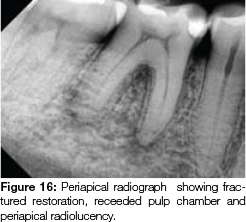
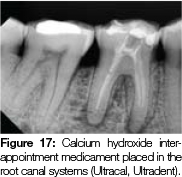
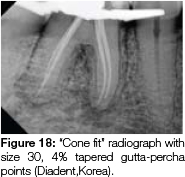
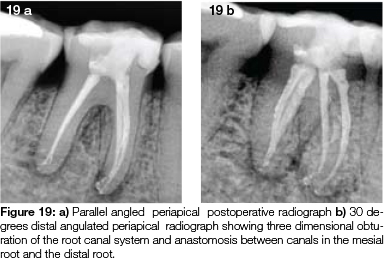
A 56-year old female patient was referred for endodontic treatment of her lower right first molar after she presented with an acute absess. Radiographic examination revealed a fractured restoration, receded pulp chamber and periapical radiolucency (Figure 16). Four canal orifices were found and the canals shaped using the following sequence: Protaper Next X1 (Dentsply/Maillefer) followed by size 25, 4% taper and finally size 30, 4% taper (Flexmaster files, VDW, Germany). The distal canals were confluent. A calcium hydroxide (Ultracal,Ultradent) inter-appointment medicament was used as there was still periapical exudate after shaping (Figure 17). A 3.5% NaOCl irrigant was used, followed by a final rinse with 17% EDTA (Smearclear, Axis/Sybron). Irrigants were agitated by active ultrasonic agitation using a size 15 NSK U-file (NSK, Nakanishi, Japan). The distal pulp horn was cleaned using a precurved 15 U file with ultrasonic agitation. Irrigation through the root canal systemwas further optimised by synchronous use of the Endovac system (Axis/Sybron) with irrigant delivery through a 31 gauge Navitip sideport needle (Ultradent) in the adjacent root canal. Size 30, 4% tapered gutta-percha points (Diadent, Korea) were tried in, confirmed radiographically (Figure 18) and tug back verified. The gutta-percha cones were coated in AH Plus sealer (Dentsply/ Maillefer) and the Reciproc R25 (VDW,Germany) was used for thermo-mechanical compaction as described previously. The core build up was completed and post-operative radiographs revealed a filling of the anastomosis between canal systems in the mesial root and also in the distal root (Figures 19a and b). The patient was referred back to her dentist for an indirect onlay with cuspal coverage.
DISCUSSION
A scanning electron microscopic comparative study found that thermo-mechanical compaction and warm vertical compaction provided equally good obturation of the root canal sys-tem.9 Leakage studies have shown that thermomechanical compaction compared favourably with lateral condensation.10-13 In widely prepared, oval, ribbon-shaped or irregular root canals, thermo-mechanical compaction has been shown to result in better filling than was achieved with lateral condensation.14,15
One of the disadvantages of the Mc-Spadden Compactor is its tendency to break in the root canal.15 The M-Wire alloy of the Reciproc files makes them more resistant to cyclic fatigue and fracture. Furthermore these files are indicated for single patient use which also reduces the risk of cyclic fatigue frature associated with repeated use of nickel-titanium instruments.16 The variable pitch of the flutes, slightly vertical orientation of the non-landed blades and S-shaped cross section of the Reciproc files makes them suitable for vertical compaction of gutta-percha. Due to the taper of the instrument it needs to be taken to only 5mm past the orifice at 20 000 rpm for 3 seconds. This provides sufficient compaction and apical and lateral displacement of a well fitted gutta-percha cone and reduces heat generation on the outer surface of the root.
It is important to confirm tug back of the gutta-percha cone and to use a minimal amount of root canal sealer, as this will reduce the incidence of sealer extrusion through the apex, a drawback of the technique. This is important when the apical foramen is close to anatomical structures such as the mental foramen, the inferior alveolar nerve and the floor of the maxillary sinus. In oval or irregular canals the gutta-percha can be laterally condensed before thermo-mechanical compaction, to provide better apical control and reduce inadvertent sealer or gutta-percha extrusion.17 The gutta-percha should be cut at least 3 to 5mm above the level of the orifice. This provides the volume needed for compaction and compensates for the amount that will be embedded in the flutes of the blade (Figure 10). Another important consideration is to remove the file along the outer wall of the canal during compaction, which reduces the volume of gutta-percha removed from the canal. If an excessive amount is removed coronally, an additional piece may be placed in the residual space, softened with the ultrasonic scaler tip and condensed with pluggers. Alternatively the coronal space can be back filled with heat softened gutta-percha. The Reciproc R25 is suitable for thermo-mechanical compaction of gutta-percha for most canals, while the Reciproc R40 can be used in larger canals.
CONCLUSION
The use of the Reciproc R25 file for thermo-mechanical compaction of gutta-percha in prepared root canal systems has been described. The technique allows clinicians a cost effective method of thermal and vertical compaction.
Conflict of Interest: None declared
References
1. McSpadden J. Self study for the thermatic condensation of gutta-percha. Toledo: Ransom and Randolph; 1980. [ Links ]
2. Malagnino VA, Passariello P. Microseal technique. In: Castelluci A, editor. Endodontics vol.2. 1st ed. Il Tridente, Italy; 2004:730. [ Links ]
3. Yared G.Canal preparation with only one reciprocating instrument without prior hand filing: A new concept. Int Dent -African Ed 2012; 2(2): 78-87. [ Links ]
4. Ye J, Gao Y. Metallurgical characterization of M-Wire nickel-titanium shape memory alloy used for endodontic rotary instruments during low-cycle fatigue. J Endod 2012;38(1):105-7. [ Links ]
5. Al-Hadlaq SM, Aljarbou FA, Al Thumairy RI. Evaluation of cyclic flexural fatigue of M-wire nickel-titanium rotary instruments. J Endod 2010;36(2):305-7. [ Links ]
6. Bartols A. Clinical experiences with Reciproc. Endo(Lond Engl) 2013;7(3):179-87. [ Links ]
7. Zuolo AS, Mello JE Jr, Cunha RS, Zuolo ML, Bueno CE. Efficacy of reciprocating and rotary techniques for removing filling material during root canal retreatment.Int Endod J 2013;46(10):947-53. [ Links ]
8. De-Deus G, Arruda TE, Souza EM, Neves A, Magalháes K, Thuanne E, Fidel R. The ability of the Reciproc R25 instrument to reach the full root canal working length without a glide path. Int Endod J 2013 Oct;46(10):993-8. [ Links ]
9. Lugassy AA, Yee F. Root canal obturation with gutta-percha: a scanning electron microscope comparison of vertical compaction and automated thermatic condensation. J Endod 1982;8:120-5. [ Links ]
10. Benner MD, Peter DD, Grower M, Bemler W. Evaluation of a new thermoplastic gutta-percha obturation technique using 45Ca. J Endod 1981;7:500-8. [ Links ]
11. Harris GZ, Dickey D J, Lemon RR, Luebke RG. Apical seal: McSpadden vs lateral condensation. J Endod 1982;6:273-6. [ Links ]
12. Ishley D J, Eldeeb ME. An in vitro assessment of the quality of apical seal of therrnomechanically obturated canals with and without sealer. J Endod 1983;9:242-5. [ Links ]
13. O'Neil K J, Pitts DL, Harrington GW. Evaluation of the apical seal produced by the McSpadden Compactor and by lateral condensation with a chlorform-softened primary cone. J Endod 1983; 9:190-7. [ Links ]
14. Kersten HW, Fransman R, Thoden van Velzen SK. Thermome-chanical compaction of gutta-percha. II. A comparison with lateral condensation in curved root canals.Int Endod J 1986;19:134-40. [ Links ]
15. Kerekes K, Rowe AHR. Thermo-mechanical compaction of gutta percha root filling. Int Endod J 1982;15:27-35. [ Links ]
16. Gambarini G. Cyclic fatigue of ProFile rotary instruments after prolonged clinical use.Int Endod J 2001;34:386-9. [ Links ]
17. Tagger M, Tamse A, Katz A, Korzen BH. Evaluation of the apical seal produced by a hybrid root canal filling method, combining lateral condensation and thermatic compaction. J Endod 1984;10:299-303. [ Links ]
