Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.69 no.7 Johannesburg 2014
CLINICAL REVIEW
Substance abuse: case management and dental treatment
YF SolomonsI; PD MoipolaiII
IBDS (Wits); MDent(Pros)(Wits). Head - Clinical Unit: Department of Prosthodontics, School of Oral Health Sciences, Medunsa Oral Health Centre, University of Limpopo
IIBChD (Leeds,UK); MDent(Pros)(Wits); MEd(Wits). Specialist Prosthodontist. Department of Prosthodontics, School of Oral Health Sciences, Medunsa Oral Health Centre, University of Limpopo
INTRODUCTION
Any patient presenting for dental treatment may be abusing drugs - licit and/or illicit, or may have a history of substance abuse, often coupled with rehabilitative procedures. The media as well as the professional literature is replete with evidence that, globally, the use of illicit drugs is approaching epidemic proportions. Currently, cocktails of both legal and illegal substances are readily available on the street, meaning that there are people from all walks of life and socio-economic category who abuse drugs. This makes it imperative that all oral healthcare (OHC) providers be aware that any patient can be a substance abuser and that these patients can present for dental care at any stage of their abuse.
There is a high burden of dental disease in substance abusers which is further complicated by concomitant emotional/ behavioural/personality issues, the often poor general health of the addict, inadequate nutrition and oral hygiene as well as by the pathological effects of the drugs on the dentition and periodontium. Currently, not only has the drug abuser become more sophisticated but a variety of trends, as well as patterns, of substance abuse are emerging. It is an essential that the dental community remains knowledgeable, educated and informed of developments in global and nationwide healthcare and it is increasingly evident that management of substance abuse is an important component. Ethically, OHC providers are expected to be able to identify any abnormalities within the oral cavity. New drugs are flooding the market before research on accompanying health risks and management can be undertaken, and hence there is a call for intensified vigilance to observe, identify and recognise the oral health complications of substance abuse. In addition to recognising the scope of the problem of substance abuse, OHC workers should be able to respond in a manner that addresses the best interests of patients who may be diagnosed as drug abusers. This response needs to include: understanding the terminology of drug abuse and of the substances often misused and abused; identifying individuals who may be at risk for abuse and managing at-risk patients in the dental setting.
ACRONYM
OHC: oral healthcare
Meth: methamphetamine
MA: methamphetamine
GI: Gastro intestine
TSL: tooth substance loss
UDT: urine drug testing
OTC: over the counter
US FDA : United States Food and Drug Administration
NSAIDs: Non steroidal anti-inflammatory drugs
The focus of this article, then, is to identify for the dental professional the implications of substance abuse, to describe strategies to assist the dental team to recognise substance abusing patients, to discuss how they can assist these patients in managing their addictions and how the necessary treatment to rehabilitate and maintain the patient's oral health can be planned and safely delivered.
This overview will include discussion on the following:
a) The implications of substance abuse on dental treatment
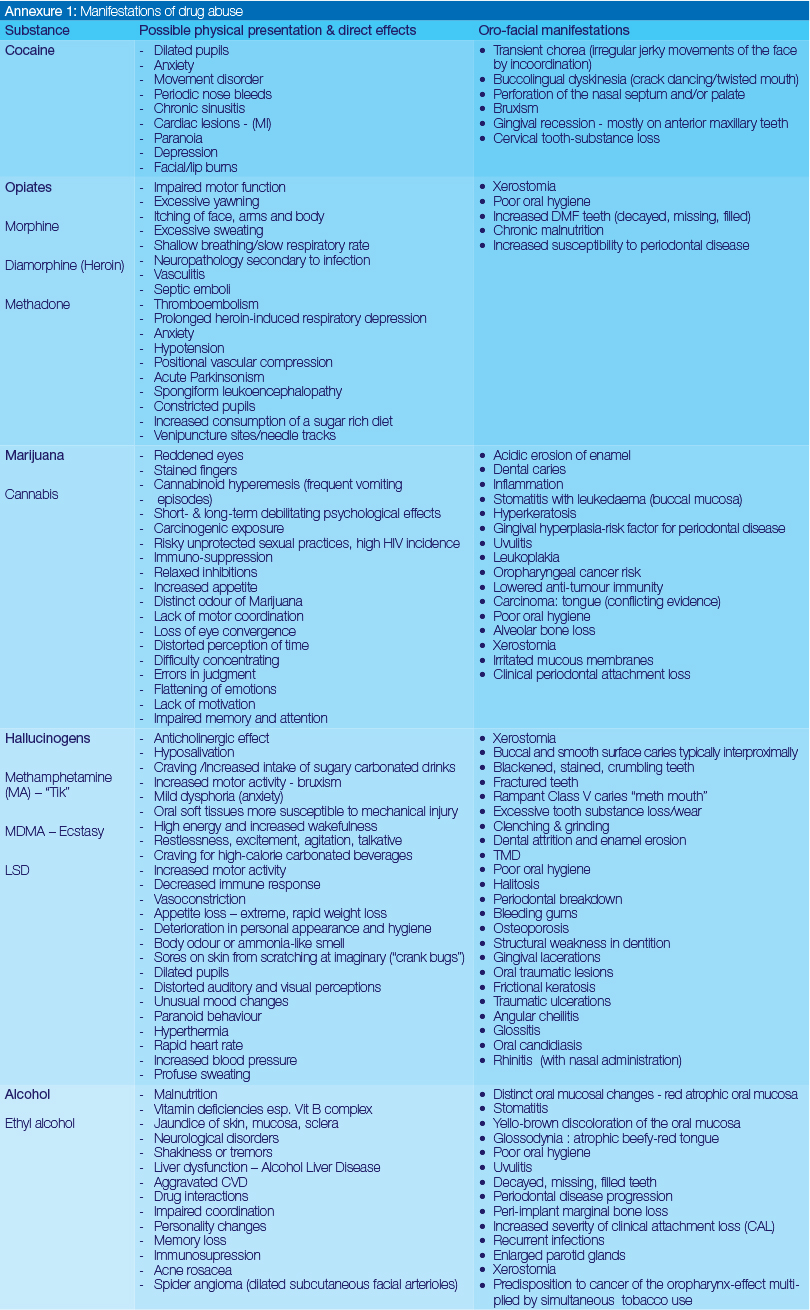
b) A summary and outline of the most commonly abused substances including their 'direct' effects on oral health. Both physical and oral manifestations are listed (see Annexure 1).
c) Identification and recognition of a substance abuser.
d) Challenges and barriers to the dental treatment of a substance abuser.
e) A proposed approach to the dental management of substance abusers.
IMPLICATIONS OF SUBSTANCE ABUSE ON DENTAL TREATMENT
Given that dental comorbidities are a prominent feature of substance abuse and that many drug addicts may be concerned about their dental appearance during the recovery and post-recovery phase, dentists can play a crucial role in the detection of substance abuse and can participate as integral members of a collaborative care team tending to the substance abuser. The use of both licit and illicit drugs has direct (induced by the drug) as well as indirect effects (lifestyle) on oral health and oral pathology.
The adverse impact of substance abuse on oral and systemic health means that dental professionals must be aware of these co-morbidities, be able to recognise pathological changes associated with the abuse of specific substances but, more importantly, need to understand how best to ensure the most efficacious treatment and to avoid possible consequences of contraindicated approaches.1
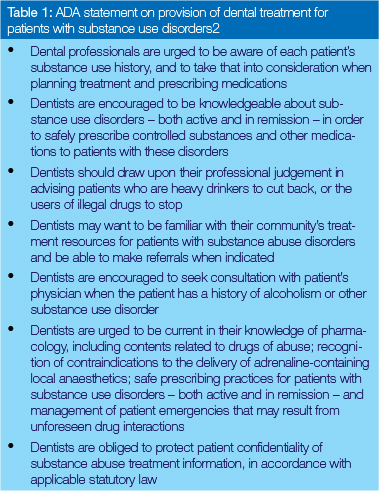
In 2005, the American Dental Association published a statement on the provision of dental treatment for patients with substance abuse disorders. In the absence of such a standardised policy in South Africa, it is highly recommended that all oral health care workers familiarise themselves with this statement.2 See Table 1.
It needs to be recognised that dental professionals do not merely provide oral health care. Their interaction with patients provides a certain platform for becoming aware of the context of the problems as well as the overall interaction of risk factors which have contributed to a substance use disorder. This further enables an understanding that would significantly impact on optimal case management, safe treatment and appropriate referral.
The potential risk factors which contribute to the spectre of substance abuse include genetic and environmental influences (chaotic home life, abusive relationships with family, friends and acquaintances, peer influences, community pressures); duration of substance use; personality (low self-esteem, stress, personal attitudes; unrealised achievements, unmet expectations, depression); availability of drugs; patient's method of drug administration and co-existing mental disorders.2 It has been shown that these factors impact on complex health issues as well as on behavioural patterns that hold significant implications for dental treatment. Long term substance abuse significantly alters the structures and functions of the brain, leading to uncontrollable compulsive and destructive (aggressive) behaviour; however, it remains important to realise that substance abuse is not a moral issue. In fact, the prevailing concept of substance abuse is that of a disease model in which the patient has no control. The case management of the substance abuser is therefore expected to differ from the management of a non-addicted patient.
All these complex issues highlight the fact that significant behavioural and medical issues can present with the substance-abusing patient that may necessitate modifications to the dental treatment plan. Furthermore, patients who use alcohol in excess or patients who abuse mind-altering substances may have problems accepting, receiving and completing dental treatment. In some cases, treatment may need to be deferred, limited in complexity, or sequenced in a different manner. It may be appropriate to first refer the patient to a physician for management of related potential or imminent medical problems or to a counsellor, therapist or substance abuse specialist to assist with managing the dependency as well as the related psychological and behavioural issues. Once the addiction is managed and the concomitant medical issues addressed, oral health treatment may proceed in a routine manner. The awareness of the possibility of relapse remains critically important and demands skills and sensitivities on the part of the dental team that are not usually required when treating non-abusing patients.
EFFECTS OF SUBSTANCE ABUSE
Some substance abusers experience pronounced effects in as little as six months to one year of starting to use the drug, whereas, in a non-user, such manifestations would take several years (along with severe oral neglect) to develop. Tobacco use by substance abusers can also exacerbate the oral health problems.
Physical presentation and oral manifestations of substance abuse
Recognising pathognomonic signs of the possible physical effects and oral manifestations of substance abuse is critical in early detection for this encourages early intervention. Dental professionals should be aware of what to look for in substance abusers in order to aid appropriate case management as well as proper referral.
Annexure 1 lists the physical presentation as well as possible physical and oral manifestations of the most popularly abused substances that are known to cause direct damage to oral and dental tissues.
Some additional substances typically available in South Africa need mention despite the paucity of scientific evidence on their potentially harmful effects on oral health. Nyaope, also known as whoonga or wunga, is a dangerous and highly addictive South African street drug. It is a fine white powder that is usually combined with marijuana (dagga) and smoked. The ingredients of nyaope are not always known, and in fact the recipe may vary from place to place. But one thing is clear, nyaope is a lethal combination of substances, which can include heroin, detergent powder, rat poison, and crushed anti-retroviral drugs (ARVs). Its addictive potential has been likened to that of heroin. It could be assumed that due to the "pronounced effect" of the abuse of this cocktail of substances, we may expect to see severe xerostomia, advanced periodontal disease and rampant caries among other signs and symptoms. The arrival of substances such as nyaope onto the drug market clearly emphasises the fact that future research should incorporate standardised measures and include drug epidemiology and dental public health research techniques to examine their actions and effects more effectively.
IDENTIFICATION AND RECOGNITION OF THE SUBSTANCE ABUSER
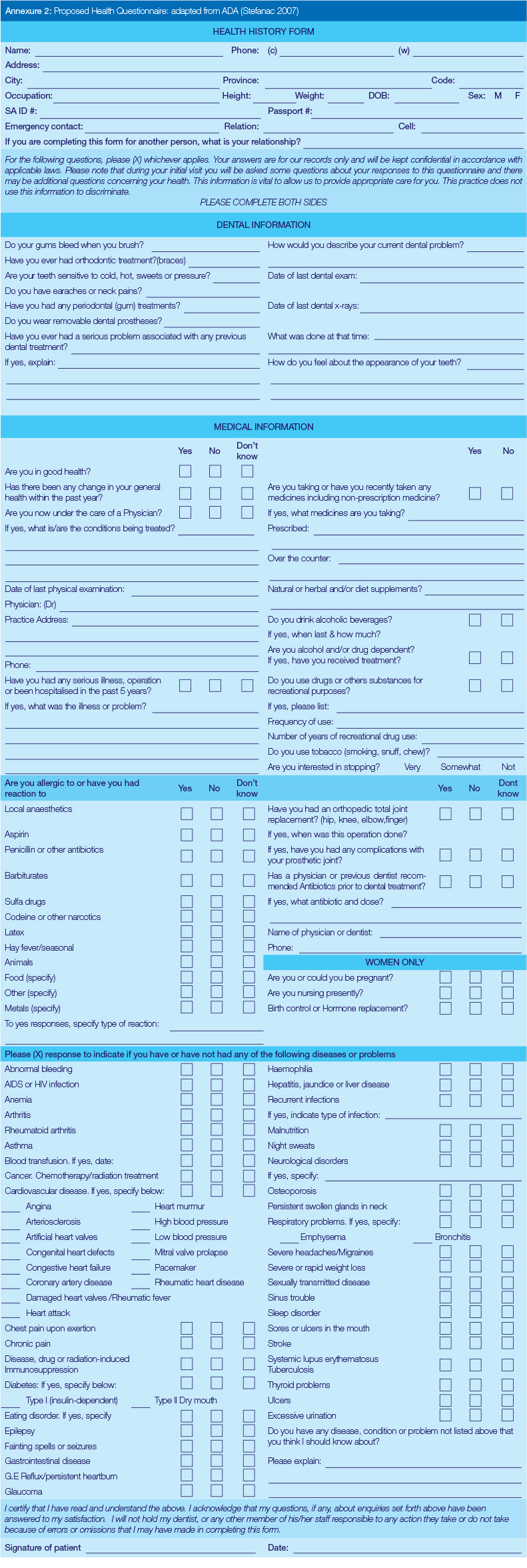
During the dental appointment, the health questionnaire and subsequent verbal interview should pose the relevant questions, allowing for a patient to indicate a previous or existing substance abusing problem (see Annexure 2 - modified ADA health questionnaire). Since it is known that patients can more easily falsify information on a questionnaire than when confronted directly, questions are best pursued verbally during an interview. Additional information can also be obtained from another health practitioner.
Ordinarily, the first essential step before initiating any comprehensive dental intervention is to obtain a thorough medical and oral health history. Of particular relevance in the case of for the substance abuser/abusing patient is the history. It is important to:
- elicit information about associated medical problems which may increase the susceptibility of the patient to a medical emergency
- reveal psychosocial sequelae of addiction
- identify other comorbidities (other diseases currently present)
- identify side-effects of abused substances and/or potential adverse interactions.
The stigma, shame and fear of judgement associated with substance abuse may cause patients to avoid revealing or denying a factual history because of the perceived risk of divulging their condition. For this reason, confidentiality of the interview and of the findings must be re-affirmed.
Following a review of the health history, the patient's general appearance and behaviour should be carefully scrutinised and observed. Generally, patients abusing stimulants may appear irritable, argumentative or overly aggressive, whilst patients abusing depressants may appear drowsy, lethargic and confused. Occasionally, patients may even use their preferred substance prior to their appointment to reduce anxiety in which event it may be best to postpone treatment.
There is merit in informing the patient that the questions pertaining to substance abuse have relevance to the provision of dental treatment. It is also critical to create an environment of mutual trust and confidentiality in order to enable the patient to be more forthcoming so as to obtain complete and accurate information. This has far-reaching implications for the delivery and outcomes of dental treatment which are not only safe and predictable but appropriate to the best short and long-term interest of the patient.3
The signs and symptoms of drug use and addiction vary depending on the drug. It may be difficult to recognise an abuser/addict based on appearance alone. Physical signs that can be helpful in recognising an abuser/addict include blood-shot eyes, changes in the size of the pupils, unusual smells on breath, body or clothing, tremors, burns on lips and fingers, grinding of teeth, clenching of the jaw, and slurred speech. However, absence of these signs does not exclude abuse or addiction. Alteration in behaviour and mood may be more indicative than changes in appearance but may be more difficult to detect. A decline in school and work performance and changes in friends and activities may also be revealing. Patients may miss appointments or be late for appointments and offer inconsistent excuses. There may be a change in their appearance and they may be withdrawn.
The possibility of substance abuse should be a consideration in all patients but especially those who present with frequent vague complaints, multiple pain medication allergies, and regimens with multiple narcotic medications. Polydrug use, either prescription or illicit, is also a possibility, and effective treatment requires prompt recognition.
It is not a given that the typical personality and behavioural changes suggestive of drug abuse will be evident when a substance abuser presents for dental treatment. On the contrary, it is most likely that these patients are generally in good health and well groomed. There may be no outward signs that will indicate substance abuse, making it difficult to identify most abusers or addicts; however, it is equally possible to find clues apparent from obvious signs which may raise suspicion of abuse.
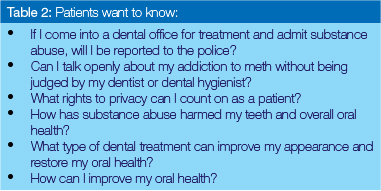
Evidence-based dental literature reported that hard core abusers generally do not seek oral health care and neither are they self-reporting on dental needs. OHC providers are likely to see the young woman or businessman who is abusing or addicted to designer or prescription drugs. Table 2 lists specific concerns such a substance abuser is likely to have:
Clinical, especially visual observation, is of critical importance during assessment of any patient, more so if there is any suspicion raised by either oral or physical signs and symptoms which cannot be justified from the patient's medical or dental history.1 This would mean to vigilantly LOOK, SEE, SMELL and LISTEN whilst being cognisant of both the direct (drug induced) as well as indirect (life-style) consequences of commonly abused illicit substances on oral health.1 The signs and symptoms of substance use and abuse vary depending on the substance. Annexure 1 records most signs that are helpful in recognising a substance abuser.
The first suspicion raised by some of the observations listed and by indications of oral findings should be regarded with circumspection and prompt the OHC provider to enquire from the patient about the possibility of abuse and to discuss specific concerns. When queries are made, they should be intentionally couched in a non-confrontational manner. The tone of voice as well as body language must be neutral, age-appropriate and have a sensitivity about the scale of harm to which the patient may have subjected him/herself, which is often as a result of dire life circumstances.
Table 3 lists tips to OHC professionals on addressing substance abusers.

THE GERIATRIC ALCOHOLIC PATIENT
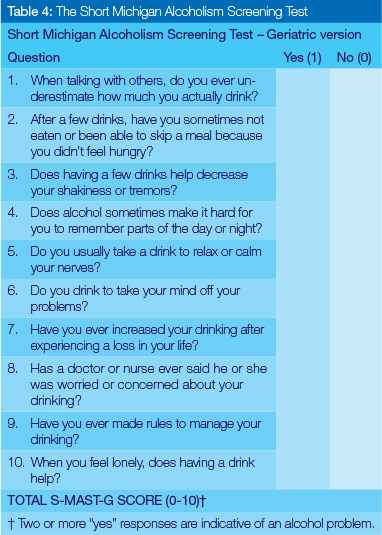
Alcoholism is a psychiatric condition which OHC providers must treat as a specific disease without moral implications. Alcohol abuse often occurs in individuals who are financially solvent and lead reasonably normal lives. Many patients try to mask the addiction, but the alert clinician often can detect the signs and symptoms of substance abuse.4 A comprehensive health questionnaire with follow-up questions usually provides an opportunity for the dentist to inquire about past and current use of alcohol and other mood-altering substances. In addition, if patients reveal the use of multiple and/or expired medications, pharmacy and dental provider shopping, conceal the smell of alcohol by the use of mints or perfume, and exhibit impaired coordination, the dentist should consider more focused screening tests. Based on the results of a preliminary health history, the dentist can screen further for alcoholism or alcohol abuse using either the Short Michigan Alcoholism Screening Test-Geriatric Version 5 (Table 4) or the CAGE Questionnaire.6 These tests can indicate individuals in need of treatment for alcohol abuse. A recent study suggested that most patients do not object to alcohol screening and alcohol counselling by dentists.7 This report also suggested that dentists should not be concerned about adverse patient attitudes toward counselling for behavioral change.
CHALLENGES IN THE DENTAL MANAGEMENT OF SUBSTANCE ABUSERS
The dental practitioner may face many frustrations and challenges in the management of the patient who abuses alcohol or other substances. Both the active and the recovering substance abuser typically bring many fears and some measure of guilt to the dental setting. The recovering user may have fear of uncontrolled pain or an underlying anxiety of relapsing into the substance habit. The provision of dental treatment may be compromised by the prevailing dental and oral conditions. Additionally, the risk of relapse is high and this needs to be factored in during the provision of dental treatment. Access to dental services is important for the recovering substance abuser to decrease the risk of relapse due to dental pain. Added to the biologic and restorative challenges that present are the financial and socioeconomic trials the substance abuser may have to deal with, wherein his/her primary goal is to secure the preferred substance of abuse instead of addressing the existing dental and oral damage. It is critical that dental treatment of substance abusers and of those undergoing detoxification incorporates careful pain relief, good local anaesthetic techniques and an understanding clinician to allow a positive experience which will not reinforce any dental anxiety.
Pain control and management
The management of pain is often a daunting task, and may lead to elements of mutual mistrust between the drug abuser and dental practitioner. It is often reported that, as a routine, substance abusers associate the quality of dental care with the degree of effective pain management. They may also have special needs in relation to receiving dental care.
Anecdotally, they may be dentally anxious and have low pain tolerance requiring careful pain relief and a good rapport with the dentist.3 It has been reported that they may also feel mistreated and view delayed provision of dental care, regardless of the reasons, as intentional mistreatment. A factor that may compound this perception is when the dental care providers are not knowledgeable about substance abuse and the recommended treatment protocols.
It is advised that patients who are high on certain drugs, such as MA, should not receive any dental treatment for at least six hours after the last 'hit'. The plasma half-life of MA ranges from 8 to 30 hours and intoxication from it is reported to last for up to 24 hours.3 There is an increased risk of myocardial ischaemia and cardiac dysrhythmias in patients "high" on the drug. Local anaesthetics with adrenaline must not be used while the patient is "high" as these may potentiate the response of sympathetically innervated organs to sympathomimetic amines. This potentiation could result in a hypertensive crisis, cerebral vascular accident, or a myocardial infarction. Administration of general anaesthesia or sedation may be associated with sudden death in MA and cocaine users. Illicit drugs, such as MA, may potentiate the respiratory depressant effect of opioid drugs.11
If a dental patient presents with signs of recent illicit drug use, it is advised that treatment in the dental operatory should consist of supportive measures only. The patient's vital signs must be monitored as the heart rate and blood pressure can be elevated. In a patient experiencing toxicity from MA, the dentist should seek immediate medical attention for the patient. Rapid breathing (tachypnoea) precedes respiratory depression during MA toxicity so the patient should be administered 100% oxygen treatment. If the patient experiences cardiovascular collapse, cardiopulmonary resuscitation will be required. Patients may exhibit acute paranoid psychosis and may become violent. In this case, care must be taken to keep the patient calm and to ensure the safety of the patient and the dental team.8
Commonly used over-the-counter analgesics are routinely employed in many dental situations. These may however, increase bleeding tendency. In urgent cases requiring a reduction in inflammation and swelling, corticosteroids may be used to avert nerve damage. However, their potential to cause adrenal crisis and elevation of blood glucose levels should always be anticipated.9 Adequate pre- and post- operative pain management is a priority to effectively manage the substance abuser's dental/oral problems.
Where local anaesthesia is needed for the delivery of dental treatment for patients who are substance abusers, a product without a vasoconstrictor should be used.10 The degree of severity of the presenting dental condition may necessitate the selection of a stronger and more effective opioid analgesic. Dentists must be knowledgeable about the pharmacological effects, duration of action, and half-life of opioids in order to prescribe or to administer the correct medication for effective pain management. Combining analgesics with different modes of action is said to provide greater analgesic efficacy than therapy utilising a single agent. Combining an NSAID (naproxen, mybulen, dicloflenac, celebrex, ibuprofen) and acetaminophen can be as effective for some moderate to severe pain. Oxycontin is said to offer advantages through a dual delivery mechanism, characterised by an enhanced immediate release phase followed by sustained delivery to prolong the duration of action.9 In patients who may have the potential to abuse or are abusing prescription analgesics, alternative strategies for limiting postoperative pain include administering prophylactic NSAID analgesics (that is, ibuprofen 400-600mg preoperatively) and the long-acting local anaesthetic bupivacaine to provide prolonged analgesia. In addition, full therapeutic doses of peripherally acting analgesic agents, such as ibuprofen and naproxen, are as effective as opioids for many patients who undergo minor dental surgical procedures, e.g. dental impaction surgery, that cause moderate to severe pain.9 Moreover, these patients typically take NSAIDs for between four and six days. Therefore, there is evidence that non-opioid analgesic agents should be considered the first line of therapy for the routine management of acute postoperative dental-related pain.11
Cocaine users may experience convulsions with the use of lignocaine.12 Intrapocket application of gingival retraction cord and a vasoconstrictor such as Oraqix gel (lignocaine and prilocaine) is also reported to have the potential to increase the risks due to the absorption of significant amounts of vasoconstrictors. It may therefore be advisable for the dentist to consult with the patient's physician or drug abuse specialist to outline a treatment plan that allows for conscious sedation for major dental procedures.12
The use of long- acting local anaesthetics in endodontic procedures should be considered in order to reduce the overall amount of anaesthetic used. These could delay the onset, and reduce the intensity of post - operative pain. It is advised that acetaminophen should be limited to less than 2.5g daily in dental patients with a history of substance abuse and having compromised hepatic function.11 The reduction proposed by the manufacturers of the recommended daily maximum dose of acetaminophen for healthy individuals might also indicate the need for a revision of this regimen.
Unrelieved or unremitting pain can be a relapse trigger and therefore adequate pain control is a necessity in the recovering chemically dependent patient. New modalities, such as co-analgesia with low-dose ketamine in the opioid-addicted, have been shown to work effectively. In the post-dental surgical patient with chemical dependency, agents with less psychoactive activity than their drugs of abuse, such as extended-release morphine (MS Contin) have been tried with variable success.9
Substance abusers, e.g. those using MA, cocaine and heroin, prescription pain medication etc., may claim to be allergic to codeine in an attempt to obtain a stronger drug such as morphine or hydrocodone. In these cases, NSAIDs can be prescribed.11 When addicts seek dental care between drug binges the usual analgesic medications (i.e. NSAIDs or narcotic combinations) can be used. Analgesics that cause CNS depression are not contraindicated unless other depressants are being used by the patient at the same time. Consultation with the patient's physician may be required to balance the need for pain relief with the risk for drug interactions.10 Some patients may use their abuse substance of choice to reduce their anxiety related to their dental appointment. It is important to acknowledge the patient's anxiety and to offer other means of reducing it, including behavioural methods.
Xerostomia
The cause of xerostomia induced by substance abuse is uncertain. In the case of MA use, it has been postulated that it may be due to activation of alpha adrenergic receptors in the vasculature of salivary glands, causing vasoconstriction and a reduction in salivary flow.13 An alternative suggestion is the stimulation by MA of inhibitory alpha 2 adrenoreceptors in the salivary nuclei which may also decrease the salivary flow rate.14 It is also postulated that some illicit drugs may alter the composition of saliva, leading to xerostomic effects intraorally. Dehydration related to substance abuse-induced elevation of metabolism and increase in physical activity may also contribute to xerostomia. Most substance abusers report feeling thirsty most of the time.15
The risk of dental caries, tooth substance loss/wear and periodontal disease is considerably increased by xerostomia, with an increased number and severity of carious lesions caused by poor oral hygiene and a high intake of refined carbohydrates and high cariogenic foodstuffs. The long term prognosis of dental rehabilitation measures in such patients would be considerably guarded.
Patients with substance abuse-induced xerostomia should be advised to drink 8-10 glasses of water per day and to avoid any beverages that have a diuretic effect such as caffeine, tobacco, and alcohol. The relief derived from salivary substitutes, oral moisturisers, and artificial saliva, though beneficial, is often inadequate. This may be due to the substitutes not exhibiting the correct viscosity to give most patients adequate relief. The substitutes are often not superior to the use of water and their effect is often short-lived because they are not retained in the oral cavity for very long.
Substance abuse-induced xerostomia can also be managed by pharmacological stimulation of the salivary glands. Agents such as pilocarpine HCl (Salagen) and cevimeline HCL (Evoxac) have been advocated for the treatment of hyposalivation in patients with Sjogren's syndrome. These stimulate smooth muscle and exocrine secretions thus enhancing the production of saliva from major and minor salivary glands.17 Increased production of saliva from minor salivary glands may be especially important for protection against oral disease because minor salivary glands produce most of the secretory IgA, a powerful component of the oral cavity's immunological defence system.
Patients with substance abuse-induced xerostomia should be carefully evaluated and the patient's physician should be consulted to determine if there are any contraindications before prescribing pilocarpine.16 Caution should be exercised in patients with hypertension, pulmonary or renal disease, cardiac dysrrhythmia or hypersensitivity to pilocarpine. Increased salivary flow is often reported to not necessarily be accompanied by improvement of symptoms. There are other pharmacological sialogogues, such as bethanachol chloride, bromhexine, anethole trithione and Interferon Alfa which have been shown to stimulate salivary flow but these need further clinical evaluation.
Caries risk and non-carious tooth surface loss
Caries development in substance abusers usually presents in a distinctive pattern resembling that observed in early childhood caries; specifically, the carious lesions are located on the buccal smooth surfaces of the teeth and the interproximal surfaces of the anterior teeth. A description typically related to MA users is teeth that are "blackened, stained, rotting, crumbling, or falling apart." Often, the teeth are in such disrepair that they are unsalvageable and must be extracted. Caries associated with chronic MA use, while rampant, is somewhat different from that seen in other disorders, such as cocaine or narcotic abuse or post-irradiation therapy for cancer. Similar to the pattern of caries associated with these other conditions, the caries occurs more frequently in the cervical region. However, the pattern of progression of the carious lesions is more similar to that seen with Sjogren's syndrome, wherein the carious lesions progress more slowly and go through periods of arrest instead of rampantly progressing.17 The reasons for this pattern, although unclear, seem to be that some of the MA users actually practice some personal oral hygiene from time to time and therefore can slightly control the progressive rate of tooth decay.
One proposed cause of rampant caries - hyposalivation -minimises the normal protective capacities of the saliva and increases the risk of caries and demineralisation risk.14 Because of the xerostomia resulting from the action of the drug on saliva production, along with dehydration related to elevated metabolism and increased physical activity, substance abusers report consuming large quantities of carbonated sugary soft drinks. Xerostomia also lowers salivary pH and promotes plaque and calculus accumulation, with resultant increase in caries incidence. Additional risk factors include: poor oral hygiene, the acidic composition of the substance abused (e.g. MA, heroin, cocaine), increased acidity in the oral cavity, GI regurgitation or vomiting and the drug's capacity for increasing motor activity, such as excessive chewing, tooth grinding and clenching. All contribute to the destruction of a compromised dentition, thus increasing the number and severity of the carious lesions. These risk factors predispose substance abusers to extensive caries.18,19
The dental disease evident in the mouths of substance abusers may also be attributed to methadone use as this is commonly prescribed for oral ingestion for short-term detoxification and long-term maintenance of opiate-dependent patients. The aim is to encourage users to switch from injecting the drug to administering it orally. The sugar content may be as much as 50% m v-1 and some users hold the medication in the mouth.20 It has also been noted that those substance abusers who inject the drug may crave refined carbohydrates, either in an effort to counteract the xerostomia, to increase the 'high' or for unexplained reasons. Refined sugar is often used as a diluent for injected drugs, and addicts are reported to yearn for it and to routinely ingest it at the time of drug injec-tion.21 In the general population, caries commonly affects the posterior teeth, therefore when adult patients present to the dental setting with rampant anterior lesions, it should be seen as a red flag for substance abuse, especially MA.
When making a differential diagnosis of non-carious tooth surface loss versus carious lesions, several parameters must be considered, including the distribution of the lesions within the dentition, aspects of the tooth involved, the disparity of the presence of the lesion on the facial and lingual surfaces, the specific sites in the dentition and their location relative to major salivary gland openings, the extent and size of the lesions on the surface of the tooth versus their depth (as detected clinically, radiographically, or post-excavation). Failing to identify the causative etiology could lead to a incorrect diagnosis that could in turn adversely affect treatment planning and misdirect a specified prevention proto-col.22 The rampant destruction that often occurs, coupled with late presentation for dental intervention, often results with a dentition that is beyond salvaging. In most cases, the treatment of choice is clearance of all non-salvageable dental units and provision of removable prostheses.
Soft tissue/mucosal/cutaneous damage
Oral mucosal ulceration is common in cocaine users. Oral effects of cocaine are related to administration of the drug via nasal inhalation, smoking and direct smearing on the oral mucosa, especially the gingivae. Rubbing the drug directly onto the gingivae has been reported to occasionally result in the development of grossly inflamed, profusely bleeding gingivae associated with epithelial desquamation.23 Such an environment would make provision of dental care very challenging. Cocaine has a vasoconstrictive effect that causes ulceration and atrophy of the tissues. Regular use of cocaine is reported to have several orofacial effects, such as perforation of the nasal septum and palate and gingival lesions. Certain habits and behaviours adopted by these patients, such as using instruments like pens and pencils to remove nasal crustings, may also increase the risk of nasal perforations. Nasal septum perforation is a frequently reported complication, observed in approximately 5% of cocaine snorters. The perforation reduces nasal support and results in a broad, flat nose, the so-called saddle nose deformity.12 The majority of the patients with cocaine-induced palatal necrosis are female (72%), despite the fact that more men than women use the drug.12 With cocaine abuse, there are also increased nasal and sinus problems that manifest as congestion, stuffiness, discharge, and occasional pain. The presence of massive plaque formation, calculus deposits, and material alba is routinely seen.22
Morphine is known to exert an inhibitory effect on the phagocytosis of Candida by macrophages, which together with salivary gland hypofunction may predispose to oral candidosis in substance- abusing patients. The concomitant smoking of cannabis and/or cocaine may be an additional aetiological factor in the onset of mucosal dysplasia. These substances contain many carcinogens that are postulated to render the epithelium more susceptible to exogenous carcinogens.24
The provision of dental restorations in an oral cavity with extensive periodontal, mucosal and cutaneous damage is challenging, if not impossible. It thus means that only emergency intervention can be undertaken prior to the management of the soft tissue lesions.
Predisposition to periodontal disease
The periodontal soft tissues of substance abusers, especially those abusing MA and cocaine,17 usually demonstrate signs of periodontal disease and chronic marginal gingivitis, demonstrated by inflamed free margin of the gingiva that appear cherry red, oedematous, glistening, with loss of the entire stippling contour that bleeds easily upon touch.25 The inflamed gingival tissues appear swollen and hypertrophied, resulting in the formation of multiple pseudo-periodontal pockets. The pattern of the presenting periodontal disease is typically one of adult periodontitis, although acute necrotising gingivitis has also been reported. It seems that the effects on the periodontium are due to a high rate of plaque accumulation, resulting from neglect and xerostomia, and may be exacerbated by the immuno-suppressive effects of opioids and potentially altered microbial profiles resulting in fungal infections. Dental plaque and materia alba are often found on most of the dentition, a sign of neglected oral hygiene. Other symptoms include bleeding gums, bad odour and taste in the mouth, loose teeth, abscessed teeth, and frequent toothaches.23
The periodontal disease would need to be managed and stabilised before any definitive restorative intervention can be undertaken. In this regard, patient compliance with the proposed dental treatment and appointments is crucial for a positive outcome and the required cooperation is usually a challenge with substance abusers.
Temporomandibular disorders (TMD) including bruxism, clenching and grinding
Long term use of most illicit drugs may lead to signs and symptoms of TMD, with substance abusers reporting symptoms that are often seen in patients suffering from TMDs. Robinson, Acquah and Gibson19 reported that drug addicts recounted a range of traumatic episodes including grinding associated with tooth wear, damage to the oral soft tissues and symptoms of temporomandibular joint disorders. The use of stimulants has also been associated with bruxism and excessive tooth wear in the past.26
Bruxism and TSL are common in chronic substance abusers whose extremely high energy and neuromuscular activity can cause parafunctional jaw movement and activity.26 Bruxism and muscle trismus can aggravate the effects and progress of periodontal disease and produce symptoms of TMD, such as tenderness in the joints and masseter muscles.15 This in combination with damage to the intrinsic structure of the dentition caused by most of the illicit drugs would predispose to excessive TSL and tooth fractures.
McGrath and Chan15 noted that 75% of study participants reported that after taking such drugs they 'felt like chewing something', with 52% reporting that they noted they had a habit of clenching or grinding their teeth. Amphetamine-like drugs are reported to have the ability to produce choreiform motor activity that may involve facial and masticatory muscles and result in unusual patterns of tooth wear.27 Hyper-irritability, a common feature among illicit drug users, leads to grinding and/or clenching of teeth. Combined with the presence of erosive acids and the lack of neutralising action due to reduced salivary flow, grinding/clenching promotes loss of softened decalcified tissues from the occlusal surfaces of the teeth and the formation of distinctive wear facets typical of the dentitions of substance abusing patients.22
Diet
Substance abusers usually have unhealthy diets as a consequence of their chaotic lifestyles. They often report poor or suppressed appetites, altered taste and smell sensation, as well as a craving for sugar, which they consume in huge amounts.15 Maintaining good dietary habits is not a priority for substance abusers, whose normal primary goal is to secure the next 'hit' in order to maintain the drug "high". Additionally, opiate abusers reported that they could not appreciate the taste of food, 'making ordinary meals taste like cardboard'. A typical diet is reported to consist of high sugary foods such as sugar, biscuits, ice cream, confectionary, doughnuts etc. These provide the energy for substance abusers to pursue their full-time occupation of drug use. Their food choices are limited to quick and easy foods which are also easy to consume on the go, but provide little nutritional value19 and are highly cariogenic. The responsibility of maintaining a nutritional diet that is not highly cariogenic lies with the recovering or recovered substance abuser but the patient must be supported by appropriate diet counselling and dental health education as part of the dental treatment.
Substance abuse rehabilitation plan/strategy
Substance-use interventions are clinically relevant for dentists, owing to the substantial effects of tobacco, alcohol and illicit drugs on oral health.28 Treatment that involves accountability and support will require a lifetime of work. Substance abuse treatment should not only focus on the medical and psychological management of the patient, but needs to include oral and dental treatment that may be necessary. Attention also needs to be placed on the medicaments that are used for the management of the substance abuse, as they may also have potentially damaging effects on the dental and oral tissues. Timing and alignment of the dental intervention is important, to ensure the effectiveness of the rehabilitation strategy.28
Substance abusers may not be able to take full control of their lives and health until they are able to enter a place of safety, which in most cases is a drug treatment and rehabilitation unit. Removing the need to take drugs may help them to focus more on their health. The facilities available, the attention received, and the support of staff and fellow substance abusers can bolster self-esteem and motivate self-care. It follows that patients who are in rehabilitation should be given easy access to dental care. Indeed, if dental treatment plays a role in the reconstruction of a non-drug using identity it will contribute to their recovery from drug use.29 Patients with substance abuse-related caries may have a high degree of patient "fallout"/drop-out - they may come into a dentist's office for one visit but then not return for further treatment. Great benefit will be derived by giving increased encouragement and support for compliance with oral health procedures and dental care provision. The most important consideration should be restoring the patient's health.29
Within the appropriate scope of some dental practices, and in conjunction with substance abuse treating specialists, dentists may want to consider using urine drug testing (UDT) to document adherence to the rehabilitation plan or to aid in the diagnosis of drug addiction or diversion. In considering the use of UDT, dentists should refer to more specific guidelines.11 Drug tests may be useful in practices with high rates of at-risk patients. In most other practices, however, there may be little opportunity or incentive for dentists to conduct UDT as a proactive step. Substance-use interventions are clinically relevant for dentists, owing to the substantial effects of use of tobacco, alcohol and illicit drugs on oral health.28
Dentists will recognise the importance of screening for substance use, but they may lack the clinical training and focused practice-based systems that could facilitate intervention. They may also be willing to address substance use among patients, including use of alcohol and illicit drugs in addition to tobacco, if barriers are reduced through changes in reimbursement, education and systems-level support.28 Instructions concerning referral to a substance abuse program or, in the case of the patient who may require more immediate treatment, to the emergency department are important aspects at the time of discharge from the dental office.6
Health factors complicating treatment
Adverse effects of substance use that are relevant to dentistry include the risk of the development of abscesses at injection sites, viral hepatitis, human immunodeficiency virus disease, endocarditis, anaesthesia complications, increased post-operative bleeding, delayed soft tissue healing, cardiac complications, hepatic and renal episodes.19,23,30
There are evidence-based studies that confirm the occurrence of hepatitis C in substance abusers.19.23,30 Many drug abusers can also be alcoholics with hepatic impairment. The resulting compromise in the hepatic function requires extra caution with the use of amide-type anesthetics like lignocaine and prilocaine, both of which are metabolised in the liver. Therefore, these patients require the standard amount of local anesthetic for each treated site. It is advisable to treat only one quadrant at a time to minimise the total dose.
Dental management of the geriatric alcoholic patient
Alcoholic patients may present severe management problems for the dentist especially during the uncontrolled phases of the disorder. These individuals are frequently poor at keeping appointments, cooperating with treatment plans and completing courses of treatment. The alcoholic patient is more likely to attend for emergency treatment than for routine examination.31 This is a situation that is liable to get worse rather than better as the proportion of the cost of dental treatment borne by patients increases. In view of the serious sequelae of chronic alcoholism it is important that the dentist is aware of the general and oral effects of the disorder.32
It is incorrect to assume that the alcoholic patient cannot be treated by the general dentist. Anxiety levels often are elevated in elderly alcoholic patients,33 and they may drink alcohol before the appointment to alleviate anxiety. Pretreatment relaxation techniques should be a consideration in the management of these patients. Close monitoring of the patient's health status during treatment can result in successful dental therapy without undue stress for the patient.32
Preventive dental education and maintenance of good oral health are important, particularly given the research findings which suggest that oral microflora may contribute to the development of intraoral carcinoma. The consequences of using over-the-counter (OTC) medications for postoperative pain and infection may be problematic. Alcohol is present in many OTC drugs, including mouthwashes, liquid analgesic preparations, liquid vitamin preparations, and liquid sleep-enhancing medications. The small amount of alcohol ingested through these medications possibly could trigger a relapse in a recovering alcoholic. Therefore, extreme care must be taken when prescribing for this group. In the active alcoholic patient, use of these medications in combination with alcohol greatly enhances their effects.34
Surgery for the alcoholic patient is complicated by problems with anesthesia, postoperative bleeding and wound healing. The alcoholic patient usually has increased tolerance for drugs and anesthetics, therefore the use of lower dosages for surgical procedures may be appropriate. Delayed blood clotting, wound healing, and osteomyelitis are often reported after routine oral and periodontal surgical procedures. A preoperative antibiotic regimen should be considered routinely.
The airway should be protected during surgical procedures because the gag and cough reflexes may be depressed in the alcoholic patient. Intravenous sedation and nitrous oxide should be avoided because of the potential for cardiovascular or respiratory depressive events and for initiating relapse in the recovering alcoholic. It is advisable that postoperative pain medication should not be given in both the active and recovering alcoholic patient. If required, a minimal amount should be prescribed and the medication controlled by a reliable family member or friend to reduce the chance for abuse by the patient.31,32
The US FDA has estimated that of the most commonly prescribed drugs, more than 50% have at least one ingredient that could react with alcohol. Enhancement of the toxic effects of some drugs is also a possibility. Alcohol inhibits the absorption and enhances the breakdown of penicillin within the stomach for up to three hours after intake. NSAIDs promote gastric bleeding when combined with ethanol and can cause gastric and oesophageal hemorrhage. Medications that may interact with alcohol should carry a warning about possible adverse effects of the combination and appropriate recommendations for modifying alcohol use should be provided. It is likely, however, that the active alcoholic will ignore these warnings. The reactions with aspirin and metronidazole are significant. Peripherally acting analgesics are the most effective drugs to use for the relief of dental pain.35
BARRIERS TO THE PROVISION OF ORAL HEALTH CARE
Drug seeking behaviour
Substance abusers can be quite adept at seeking ways to sustain their habit. Behaviours can include a drug addict choosing to retain an unrestorable tooth as a means to obtain prescription for potent analgesics.23 Occasionally they may contact the dental professional at an inopportune time for a prescription claiming to be allergic to non-narcotic agents and request specific narcotics for pain relief. Warning signs of possible abuse of prescription drugs include the use of more than the recommended dosage of medication and then the requesting of repeat scripts, complaining of vague symptoms to get more medication, lack of interest in treatment options other than medications, seeing several physicians and/or pharmacies and/or dentists to gather yet more medication.1 Often the drug requested is more potent than the dental procedure requires. In such instances, in order to maintain vigilance and control, the patient must be carefully confronted with the suspicion of substance abuse, references must be carefully checked and the minimum amount of medication prescribed.2 Such behaviour may also be observed in the recovering drug addict, not only in the active drug abuse patient. It is therefore important that dentists are well versed in noticing signs of drug abuse so as not to become enablers of the problem.
OHC Practitioner Scepticism
Another barrier may be the scepticism of dental practitioners about these patients committing to treatment and their reliability to keep appointments, as they are reported to constantly miss dental appointments.36
Behavioural change, although difficult, is not impossible. However, in their dedication to the oral health of these patients, dentists may in effect coerce the patient into commitments that he/she cannot or will not keep. Feeling incapable of achieving unrealistic goals, the practitioner may quit trying, discharging all responsibility to the patient, who in effect is unstable and has an altered psychological mind-set.
Associated psychological factors and perceptions
Substance abusing dental patients may experience an inordinate degree of anxiety over dental treatment, a fear of dental needles and a low pain tolerance. When patients display visible psychological distress, they must be approached with caution, allowing the opportunity to explore whether the underlying problem is dental anxiety or a dental phobia, symptomatic of a psychological disturbance.37 When dealing with a nervous patient, consideration should be given to explaining the processes involved and allowing the patient to present their oral symptoms and concerns about themselves. A good chair-side manner and excellent team approach makes the encounter less frightening for these individuals.38 Moulton39 suggests that good therapy starts with good history -taking, establishing the basis for good communication and confidence building. An attempt should be made to determine whether the distress is due to dental anxiety or other more deep-seated psychological causes40 as the pain may be a somatic representation of a psychical pain.41 Where it is apparent that other aspects of the patient's life affects their need for, or ability to accept treatment, counselling skills on the part of the OHC provider become critical for the effective management of the patient and the presenting condition. The agenda may differ from the one apparently presenting, and an attempt should be made to be explore the possibility of both overt and covert agendas.41 Treatment may be compromised without this understanding.
Behavioural management strategies should form part of a comprehensive plan to manage the recovering or active drug addict.38 One reported strategy of constantly talking to patients during active dental treatment will keep the patients' minds off what is being done and encourages them to maintain appointments and to comply with oral hygiene and dietary instructions. An integrated approach may be adopted which may include:
- education of the dental team on the use of counselling skills; patient-centred counselling where closeness and empathy is provided by the clinician to encourage the patient to divulge delicate material;
- possible referral to other healthcare providers (psychologists; counsellor etc.);
- utilisation of various models such as
- the Egan model - a method that provides a structure for counselling that is to follow
- psychodynamic counselling - whereby the dentist is enabled to adapt to the patient's needs, reformulating the way they relate to the patient and allowing the patient to return from a childlike to an adult state
- cognitive behavioural therapy (CBT) - this uses the view of human experience involving the four interactive elements of cognition, emotion, behaviour and physiology. CBT helps clients break out of negative chain reactions.42 It also helps patients recognise that their beliefs and thinking styles are pathological and that they contribute to addictive behaviour. CBT teaches people skills for coping with difficult and stressful situations, cravings and feelings that in the past would have forced them to their abuse substance of choice.
Another barrier is the perception of the patient that there is difficulty in getting a dentist to deliver treatment. Patients report being alienated by OHC providers and their fear of being treated differently causes them to hide their substance abuse history.
Other barriers identified by substance abusers include their preoccupation with avoiding withdrawal, homelessness, prolonged bingeing, waiting lists for drug treatment and low self-esteem.19
CASE MANAGEMENT OF THE SUBSTANCE ABUSING PATIENT
Diagnosis and treatment planning when faced with a substance abuser is complex, potentially encompassing the entire field of dentistry and some of medicine as well, especially when decisions have to be made on the prognosis of the proposed interventions. Often the prognosis is so clouded by a myriad of issues that the treatment finally adopted is a compromise. For instance, a complete clearance and provision of full removable dentures may be the preferred choice but may not be justified at that time for the patient. This may then necessitate giving/leaving the patient with an incomplete and debilitated natural dentition and instituting 'patchwork' dentistry - i.e. the application of add-on and wraparound direct restorations, and or various types of shell crowns in an attempt to forestall the inevitable. It should be noted that patchwork dentistry does not justify the provision of poor quality restorations. Good quality patchwork can prolong the useful life of a terminal dentition and postpone total clearance. This application requires that cost-benefit ratio must be considered, i.e. (i) is the time and money to be invested justified in light of the prognosis? and (ii) the patient must know, understand and accept this treatment approach for what it is - a temporary holding action.43
Managing the drug addicted or substance abusing dental patient is different from treating the non-addicted patient due to differences related to the emotional/behavioural/personality issues of the addict, the often poor general health and poor nutrition, on-going problems of oral hygiene and the effects of drugs on the oral mucosa, gingiva and dentition.1 Due to the complex social and clinical aspects of managing the health problems of substance abusers, a different/nuanced approach to their dental management must be considered. This differs from the 'traditional/normative' approach, which tends to focus primarily on morphological and technical aspects as determinants of treatment need.
OHC providers see a broad proportion of the population and have regular contact with people who may not otherwise seek oral health care.28 There is strong evidence that even brief interventions in primary health care settings can produce significant and sustained reductions in tobacco use and alcohol consumption.44,45,46
The most important factor in treating the oral effects of substance abuse is for the patient to stop using the drug. Continued use of the substance of abuse will comprise the prognosis of well - intended therapy. Moreover, financial difficulties that result from abuse of alcohol and other illicit substances will make it difficult for the patient to afford dental treatment making complete dentectomy the most appropriate treatment option.18 Chronic substance abuse can result in psychosis and paranoia that can last for years after the illicit drug use is stopped. Thus, the OHC team must determine how well the patient is able to participate in his/ her dental care. If the patient is able to participate, there are treatments that can improve salivary flow and reduce development and progression of caries. Meticulous oral hygiene with minimally abrasive fluoridated dentifrices and irrigation devices is desired. Frequent oral hygiene instruction and prophylaxis is mandatory. The patient's nutrition must improve with an emphasis on decreasing the consumption of refined carbohydrates. Referral to a dietician may have merit. Frequent application of concentrated fluorides delivered either as a direct brush-on or by custom-made trays can prevent the rapid progression of caries.10,47 Non-prescription fluoride rinses are inadequate. Sodium fluoride (5000 ppm) is preferred over stannous fluoride for several reasons.47 Stannous fluoride has an unpleasant metallic taste, may cause burning sensations in patients with xerostomia, and may stain enamel.
TREATMENT AND MANAGEMENT STRATEGIES
In recognition of the move towards the provision of evidence based treatment, the adoption of the sociodental approach is proposed.48 This is aimed at ensuring safe and effective clinical practice in the prosthodontic rehabilitation of substance abusers. It is mainly directed towards limiting restorative interventions to the minimum necessary.48 In contemporary clinical practice, patients increasingly assume an active role in determining their actual treatment needs, by stating their expectations and desires.
A phased approach to managing the oral healthcare needs of the substance abuser should be considered, with the emphasis placed on a medical approach to the dental intervention. This approach is focused on managing the underlying disease. Normative systems for determination of prosthodontic treatment-needs usually disregard social aspects. Little or no value is given to how oral conditions affect the daily lives of patients or whether they can change behaviour to facilitate a real health gain.49 Dental management of substance abusers cannot be done in an isolated manner. It has to be delivered in conjunction with other healthcare providers - a multi-health team approach which is part of the drug rehabilitation strategy.
Shared decision making
Shared decision means educating the patients about their problems and making them partners in determining the appropriate course and the specific elements of a proposed treatment plan.
Dental professionals are most-often concerned with the technical aspects of dental treatment and the risk for treatment outcomes while patients place a higher value on symptomatic relief of oral disease.50 Furthermore, patient perceptions of oral health and disease are strongly related to an acceptance of the proposed treatment, and their subsequent compliance is dictated by their psychological and economic preferences.
Whilst the autonomy of the patient in the decision-making-process is an important legal and ethical requirement, the desire of an individual patient for knowledge and for discussions of treatment options is highly variable and difficult to predict. Some patients do not desire an active role in making decisions regarding their health and treatment. A screening tool to determine the depth of desire for information could be useful to determine specific needs, and to assist with customizing the treatment discussion.51
The most fundamental dental relationship involves just two parties - the dentist and the patient. However, in managing complex cases, a number of relationships may need to be considered to participate in treatment planning decisions (Figure 1).52

The clinical application of a socio-dental approach in prosthodontic management of the substance abusing patient
Substance-abusing patients have many problems and associated diagnoses, often interrelated and complex, which require analysis before treatment can begin. The concerns with which OHC practitioners struggle most are:
a) intervention or no intervention?, b) the extent of intervention; c) the most appropriate option; d) the sequence of intervention; e) patient's awareness of the extent of the problem and f) prognostic factors.
Prosthodontic care, as a rule, allows multiple treatment choices. Multidimensional aspects of needs assessment and determination, involving both the clinician and the patient, must guide clinical decisions, and can be summarised as follows:
1. Patient's chief complaint: assessment of present dental status, self-perceived needs and susceptibilities, priorities for care, perception of symptoms, and feelings of threat of disease, as well as a professional identification and judicious assessment of normative needs.
2. Patient's desires and expectations: assessment of patient's expected outcomes and patient's beliefs about potential risks and benefits of treatment.
3. Patient's preferences: evaluation of patient's previous concepts and beliefs about prosthodontic alternatives, and attitudes in response to proposed treatment plans; if necessary, unrealistic thoughts may be changed by a through professional orientation.
4. Impact of intervention on quality of life of the patient: evaluation of the potential influence of treatment on daily activities and interference with social environment.
5. The likelihood of a favorable prognosis for the individual patient: the probability of success and long-term survival of treatment.
6. Patient's ability in maintaining a healthy oral condition after treatment: involves individual's potential for increased dental health care, promoted and supported by appropriate dental health education.
7. Viability of other treatment alternatives: assessment of effectiveness and safety of different intervention approaches.
8. Patient's capacity to handle the stress associated with all stages of treatment, mainly with extensive and invasive approaches.
9. The availability of resources : financial, personnel, technical support, and professional skills to perform the proposed treatment plan (in some cases referral is advised).
These determinant factors should always be considered as playing an important role in a successful prognosis. More aggressive care levels may be selected only if a strong supporting rationale takes into account these determinants in diagnosis and treatment planning. The dental practitioner must be able to integrate all phases of treatment and coordinate all the various disciplines in order to ensure proper sequencing and continuity of care and treatment. An effective dental treatment plan is a general and comprehensive plan, involving the patient first, directed towards goals established with and for that individual patient.
Fundamental skills would involve developing treatment objectives, separating treatment into phases, presenting the treatment plan, sequencing procedures, consulting with other practitioners as multi-disciplinary liaisons dictate, obtaining informed consent and then documenting the treatment plan. Much material is presented in the dental literature, guidelines which must be modified by the circumstances of each individual patient,48,49,50,51,52
Figure 2 represents a simplified treatment planning process in dentistry (modified from Stefanac, 2007).52


Guidelines for sequencing dental treatment
A functional treatment plan must be considered to be dynamic, not static, evolving in response to changes in the patient's oral or general health. Although the order in which the treatment should proceed may vary, some general guidelines can be followed initially to sequence procedures. The resulting list of procedures addresses the patient's most severe problems first and concludes with those of less consequence (Figure 3).
Success in the effective accomplishment of disease control is achieved through the active control of modified contributory risk factors and a decrease in caries susceptibility. The utilisation of transitional restorations has several benefits for the patient and clinician, including quickly increasing self-esteem; providing immediate motivation by improving dental aesthetics and oral health; reduction and control of pain; assessing patient's caries risk with a view of reducing that risk; provision of restorations utilising dental materials with a high cariostatic potential.
Re-evaluation stages are necessary to monitor disease stabilisation; patient motivation and compliance prior to further active intervention. It also provides an opportunity to finalise the choice of the materials intended to be utilised during the restorative and rehabilitative phases. The patient's host response will also play a key role in this decision.
CONCLUDING REMARKS
Despite increased awareness about the disease of addiction, the number of patients with a history of substance abuse has been consistently increasing. Being presented with complex problems that defy our attempts at simplification is becoming the norm. With the pending health care reforms in South Africa, it is expected that all health care professionals, including dentists, will be treating more patients with substance abuse issues. Hence, there will be an increased need to have effective screening processes in the dental office. Also, given the correlation between oral and general health status, increased attention should be accorded to oral health concerns among substance abusers. Dental and substance abuse problems should be regarded as associated co-morbidities, requiring the development of treatment plans which address both the substance abuse as well as the potential and resultant oral health problems.
Understanding the risk of interactions between the drugs which OHC practitioners use or are likely to prescribe and the substances some patients consume, along with the potential risk of patients being or becoming addicted to prescribed pain medications, OHC practitioners have a legal and ethical responsibility to be increasingly aware of substance abuse issues. Furthermore, as dentists frequently develop long-term relationships with patients, they are in a unique position to assist in national public health efforts to screen for substance abuse and to help affected patients to access available resources. Awareness among the care providers has to be continual to ensure a sound foundation of knowledge on the topic.
Knowledge and recognition of the oral and dental conditions manifested by abused substances is necessary in order to both properly diagnose and treat (or sometimes delay treatment) in an efficient manner without doing harm to the substance abusing patient. Success in the treatment of complex cases usually depends greatly on a well thoughtout plan and meticulous execution of that plan. As there are few shortcuts in taking on the challenge of such treatment plans, OHC practitioners must be prepared to devote extra time and effort. The risks are greater, and the additional time required for a successful outcome often makes for comparatively modest monetary rewards. The satisfaction to be gained from a successful intervention as well as the patient's gratitude and appreciation over the ensuing years are priceless and make all the extra effort worthwhile.
Finally, the authors support the recommendation of the 1995 Institute of Medicine Report, "Dental Education at the Crossroads", that there is a need for the development of a dental healthcare delivery system that focuses on patient centered care and recommends an education system in which "patients' preferences and their social, economic and emotional circumstances are sensitively considered". It is common knowledge that the undergraduate dental curriculum pays inadequate attention to this significant social disease and its management. Considering the global increase in substance abuse as well as the harm caused, a call needs to be made to not only mainstream addictive disorders and substance abuse into dental care but, imperatively, for the inclusion of and emphasis on this subject matter in the undergraduate dental curriculum. Programmes designed to improve the oral health of substance abusers need to be developed and implemented in a manner amenable to the varying social circumstances of this marginalized group of the community.
Recommendations for finding help and support for substance abuse and drug addiction:
Drug help centres for possible referrals:
Narcotics Anonymous: 083 900 6962; www.na.org.za
outh African National Council on Alcoholism & Drug Dependence (SANCA):
SANCA National Directorate: 08614 SANCA, 08614 72622 sancanational.org/index.php/component/content/article/10-portfolios/12-research.html
SANCA centres (31) contact details:
http://sancanational.org/index.php/database.html
Tharagay Treatment Centre: 021 762 2425
Drug Rehab S.A: www.drugrehabsa.co.za
Narconon: www.narconon.org/drug-abuse/parents-get-help.html
12 Step Programs:
Alcoholics Anonymous: www.aa.org.za
Narcotics anonymous: www.na.org.za
Cocaine anonymous: www.ca.org.za
Searchlight Intervention East London, South Africa:
071 544 825, www.facebook.com/loveadonai
References
1. Reimer L, Holmes R. Under the influence: informing oral health care providers about substance abuse. J Evid Base Dent Pract 2014; 14S:[127-135]. [ Links ]
2. Fung EYK, Giannini PJ. Implications of drug dependence on dental management. Gen Dent 2010; May/June: 236-41. [ Links ]
3. Ratcliff J S, Collins G B. Dental management of the recovered chemically dependent patient. J Am Dent Assoc 1987; 114: 601-3. [ Links ]
4. Ross RK, Bernstein L, Trent L, et al. A prospective study of risk factors for traumatic deaths in a retirement community. Prevent Med. 1990; 19(3):323-34. [ Links ]
5. Friedlander AH, Norman DC. Geriatric alcoholism : pathophysiology and dental implications. JADA 2006; 137:330-8. [ Links ]
6. Bullock K. Dental care of patients with substance abuse. Dent Clin N America 1999; 43(3):513-26. [ Links ]
7. Miller PM, Ravenel MC, Shealy AE, et al. Alcohol screening in dental patients: the prevalence of hazardous drinking and patients' attitudes about screening and advice. J Am Dent Assoc. 2006; 137(12):1692-8. [ Links ]
8. Hamamoto DT, Rhodus NL. Methamphetamine abuse and dentistry. Oral Diseases 2009; 15, 27-37. [ Links ]
9. Hussain F, Frare R.W, Py Berrios K L. Dental management of patients with a history of substance abuse with special consideration for addicted pregnant women and addicted dental care providers 2013-03-www.oralhealthgroup.com - accessed May 2014 [ Links ]
10. American Dental Association. Methamphetamine use: meth mouth. www.ada.org/prof/resources/topics/methmouth.asp -accessed Jan 29 2014. [ Links ]
11. Denisco RC, Kenna GA, O'Neil MG, Kulich RJ, Moore PA, Kane WT, Mehta NR, Hersh EV, Katz NP. Prevention of prescription opioid abuse: the role of the dentist. J Amer Dent Assoc 2011; 142(7):800-10 - accessed June 2014. [ Links ]
12. Brand HS, Gonggrijp S, Blanksma CJ. Cocaine and oral health. Brit Dent J 2008; 204(7): 365-9. [ Links ]
13. Shaner JW Caries associated with MA abuse. J Mich Dent Assoc. 2002; 84(8): 42-7. [ Links ]
14. Saini T, Edwards PC, Kimmes NS, Carroll LR, Shaner JW, Dowd FJ. Aetiology of xerostomia and dental caries among methamphetamine abusers. Oral Health Prev Dent 2005; 3(3):189-95. [ Links ]
15. McGrath C, Chan B. Oral health sensations associated with illicit drug abuse. Br Dent J 2005; 198(3):159-62. [ Links ]
16. Rhodus NL. Oral pilocarpine HCl stimulates labial (minor) salivary gland flow in patients with Sjogren's syndrome. Oral Dis 1997; 3: 93-8. [ Links ]
17.Rhodus NL, Little JW. Methamphetamine abuse and "Meth Mouth." Northwest Dent 2005; 84(5):29-37. [ Links ]
18. Klasser G, Epstein J. Methamphetamine and its impact on dental care. J Can Dent Assoc 2005; 71(10):759-62. [ Links ]
19. Robinson PG, Acquah S, Gibson B. Drug users: oral health-related attitudes and behaviours. Br Dent J. 2005; 198(4): 219-24. [ Links ]
20. Sheedy JJ. Methadone and caries. Case reports. Aus Dent J 1996; 41: 367- 9. [ Links ]
21. Scheutz F. Five year evaluation of a dental care delivery system for drug addicts in Denmark. Community Dent Oral Epidemiol 1986b; 12: 29-34. [ Links ]
22. Bassiouny MA. Dental erosion due to abuse of illicit drugs and acidic carbonated beverages. Gen Dent 2013; March/April: 38-44. [ Links ]
23. Rees TD, 1992: Oral effects of drug abuse. Crit Revs Oral Bio & Med 3:163-84. [ Links ]
24. Titsas A, Ferguson MM. Impact of opioid use on dentistry. Austr Dent J 2002;47(2): 94-8. [ Links ]
25. Rosenbaum CH. Did you treat an addict today? Int Dent J 1981; 31: 30-2. [ Links ]
26. Curtis EK. Meth mouth: a review of methamphetamine abuse and its oral manifestations. Gen Dent 2006; 54(2):125-9. [ Links ]
27. Milosevic A, Agrawal N, Redfearn P, Mair L. The occurrence of toothwear in users of ecstasy (3,4-methylenedioxymethamphetamine). Community Dent Oral Epidemiol 1999; 27: 283-7. [ Links ]
28. McNeely J, Wright S, Matthews AG, Rotrosen J, Shelley D, Buchholz MP, Curro FA. Substance-use screening and interventions in dental practices survey of practice-based research network dentists regarding current practices, policies and barriers. J Amer Dent Assoc 2013; 144(6):627-638 - downloaded June 30, 2014. [ Links ]
29. Ettore B. A study of voluntary drug agencies: their roles in the treatment and rehabilitation field. Br J Addiction 1987; 82: 681-9. [ Links ]
30. Scheutz F. Five-year evaluation of a dental care delivery system for drug addicts in Denmark. Commun Dent Oral Epidemiol 1984; 12: 29-34. [ Links ]
31. Dunkley RP, Carson RM. Dental requirements of the hospitalized alcoholic. J Am Dent Assoc 1968; 76(4):800-3. [ Links ]
32. Christen AG. Dentistry and the alcoholic patient. Dent Clin North Amer 1983; 27(2):341-61. [ Links ]
33. Hajat S, Haines A, Bulpitt C, et al. Patterns and determinants of alcohol consumption in people aged 75 years and older: results from the MRC trial of assessment and management of older people in the community. Age Ageing 2004; 33(2):170-7. [ Links ]
34. Johnson RB. Identification and treatment of the geriatric alcoholic dental patient. Parkell Online Learning Center (2011) - (http://cdeworld.com/courses/4514-Identification_and_treatment_of_the_geriatric_alcoholic_dental_patient#sthash.fc53NuVa.dpuf - accessed May 2014) [ Links ]
35. Seymour RA. Dental pharmacology problems in the elderly. Dent Update 1983; 15(9): 375-81. [ Links ]
36. Turkylimans I. Oral manifestation of "meth mouth": a case report. J Contemp Dent Prac 2010; 11 (1): 1-7. [ Links ]
37. Freeman R, Lamey P-J. Clinical and theoretical observations on atypical facial pain. Psychoanal Psychother 2000; 14: 23-6. [ Links ]
38. Smith S, Norton K. Counseling skills for doctors. Buckinghamshire: Open University Press, 1999: 50-62. [ Links ]
39. Moulton R E. Emotional factors in non-organic temporo-mandibular joint pain. Dent Clin N America 1966; 609-19. [ Links ]
40. Freeman R E. Dental Anxiety: A multifactorial aetiology. Br Dent J 1985; 159: 406-8. [ Links ]
41. Broom B. Somatic illness and the patients other story. Free Assoc. Books, London 1997. Chapter 1. Seeing and not seeing. Chapter 4. Diagnosis and engaging the patient. [ Links ]
42. Hoad-Reddick. How relevant is counselling in relation to dentistry? Brit Dent J 2004; 197(1): 9-14. [ Links ]
43. Dunitz M. Strategies in Dental Diagnosis and Treatment Planning, 2nd Ed. London: Taylor and Francis e-Library, 2004: 236-47. [ Links ]
44. Solberg L, Maciosek M, Edwards N, Khanchandani H, Goodman M. Repeated tobacco-use screening and intervention in clinical practice: health impact and cost effectiveness. Am J Prev Med 2006; 31(1):62-71. [ Links ]
45. Fiore MC, Jaen CR, Baker TB, et al. Treating tobacco use and dependence: 2008 update-U.S. Public Health Service Clinical Practice Guideline Executive Summary. Respir Care 2008; 53(9): 1217-22. [ Links ]
46. Whitlock EP, Polen MR, Green CA, Orleans T, Klein J. U.S. Preventive Services Task Force. Behavioural counselling interventions in primary care to reduce risky/harmful alcohol use by adults: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2004; 140(7):557-68. [ Links ]
47.Donaldson M, Goodchild JH. Oral health of the MA abuser. AM J Health Syst Pharm 2006; 63(21):2078-82. [ Links ]
48. Bowley J. Minimal intervention prosthodontics: current knowledge and societal implications. Med Princ Pract 2002; 11 (Suppl 1)22-31. [ Links ]
49. Leles CR, Frere M. A socio-dental approach in prosthodontic treatment decision-making. J Appl Oral Sci 2004; 12 (2) : 127-32. [ Links ]
50. Kay EJ, Nuttal NM, Kwill-Jones R. Restorative treatment thresholds and agreement in treatment decision-making. Community Dent Oral Epidemiol 1992; 20(5): 265 - 8. [ Links ]
51. Johnson BR, Schwartz A, Goldberg J, Koerber A. A chairside aid for shared decision-making in dentistry: A randomised controlled trial. J Dental Educ 2006 70 (2) : 133-41 [ Links ]
52. Stefanac SJ. Treatment Planning in Dentistry, 2nd Edition. Mosby Elsevier, 2007. [ Links ]
 Correspondence:
Correspondence:
YF Solomons:
Department of Prosthodontics
School of Oral Health Sciences P.O Box D12
Medunsa Campus, 0204
South Africa
Tel: +27 12 521 4815
Fax: +27 12 521 3638
Email: yvette.solomons@ul.co.za