








Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.69 n.6 Johannesburg 2014
COMMUNIQUE
Coding guidelines for dentists
M Khan
ICD-10 coding remains confusing for some dentists and their personnel. We have recently heard from the administrators that they had to reject R18 000 worth of claims on one day as a result of incorrect ICD-10 coding. This article attempts to provide some clarity on this issue
The biggest misconception about ICD-10
The most common question asked about the system is: "What is the ICD-10 code for this procedure code?" Please note that ICD-10 coding does not work like this. There is no standard or fixed ICD-10 code related to any procedure code
Basic principle of ICD-10 coding
ICD-10 coding is a diagnostic system and dental procedures can be performed as result of various different diagnoses. The dentist must make and document a diagnosis before a treatment plan can be formulated. The diagnosis is then translated nto an ICD-10 code
"What diagnosis led to the treatment being performed?" By answering this question, most of your ICD-10 coding confusion will disappear.
General examinations are, of course, excluded because the diagnosis is not known before the examination. In such instances special codes exist that can be used for this purpose.
Importance of accurate ICD-10 reporting
ICD-10 coding is an integral part of your clinical records and is required in terms of an international agreement to determine disease patterns and to accumulate diagnostic data. We are aware of the fact that this information has not yet properly been analysed but, despite our efforts to object to the system, the lack of analysis does not exempt us from the obligation to submit the data. Given that schemes have the right to reject claims on the basis of inaccurate ICD-10 coding, we would like to empower our members with the requisite information to enable them to claim effectively, regardless of our personal opinions regarding the efficacy of the system.
CASE EXAMPLE 1
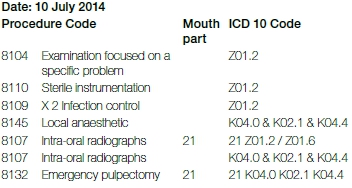
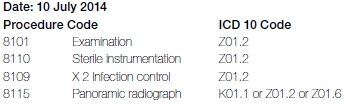
Patient arrives at your practice complaining of tooth ache on tooth 21. You have only a 30-minute appointment available. During the interview you determine that the tooth has been constantly painfull since the previous night. The patient complains that exposure to heat causes extreme pain that persists for a very long time and seeks relief from the pain. The patient agrees that you can take a periapical radiograph of the tooth. The radiograph shows an interproximal carious lesion on the distal of tooth 21, extending deep into the dentine, but not yet into the pulp. The lamina dura in relation to the apex of the root appears to be normal. The tooth responds with a sharp pain following a percussion test. You document the following diagnosis on your records: "21 severe interproximal caries (distal) with an irreversible pulpitis and an acute periapical periodontitis". You explain the diagnosis, the required follow-up procedures and the estimated costs to the patient who agrees to a root canal treatment and further radiographs.
The invoice after treatment is as follows:
Discussion
For the purpose of the examination, the dentist and assistants have to wear gloves and masks and have to use sterilised instrumentation. Since a diagnosis can only be made after a thorough examination has been completed, ICD-10 code "Z01.2 - Dental examination," is appropriate to be reported in relation to all the procedure codes relating to the examination itself. The dentist also has to take a radiograph to confirm the diagnosis. Either "Z01.2 - dental examination" or "Z01.6 - radiographic examination" will be appropriate codes to report for the pre-operative radiograph. After making the diagnosis, the dentist will commence with treatment, starting with the local anaesthetic. Therefore codes "K04.0 - pulpitis", "K02.1 - caries in dentine" and "K04.4 - acute periapical periodontitis" are the applicable diagnostic codes. If the practice management software can only accommodate a single code, "K04.0 - pulpitis" would be the most appropriate as it represents the patient's main complaint and the reason why the emergency root canal is being done in this instance. The same applies to the emergency root canal treatment. A case can also be made that these three ICD-10 codes also apply to any additional radiograph that informs the technical process of root canal treatment. Z01.2 and Z01.6 would however also be appropriate. The selection of an appropriate ICD-10 code is therefore dependent on the dentist's diagnosis leading to the treatment. It is very important from a record keeping perspective that the reported ICD-10 codes should correspond with the documented diagnoses on the patient's record.
CASE EXAMPLE 2
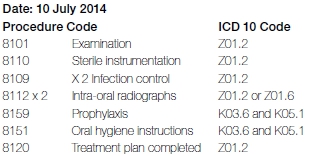
Patient arrives at your practice for his annual check-up. A full mouth examination, which included bitewing radiographs left and right, and a complete periodontal charting,* reveals no new carious lesions and confirms that all the existing restorations are intact. The periodontal probing depth is normal but you found substantial bleeding upon probing which is probably caused by the visually obvious plaque as well as supragingival calculus. You document the following diagnosis on your records: "plaque, calculus and semi-generalised chronic gingivitis". After you explain to the patient the diagnosis, the required follow-up procedures and estimated costs, he agrees to a scale and polish and accepts that he will pay for the oral hygiene instructions. You decided against a professional fluoride treatment because you assessed the patient's future risk for dental caries to be low. Professional fluoride treatment would therefore be inappropriate according to scientific standards.
The invoice after treatment is as follows:
Discussion
Refer to Case Example 1 for an explanation of the use of code Z01.2 in relation to the examination, infection control, as well as sterilised instrumentation. Also refer to Case Example 1 for an explanation of the use of ICD-10 codes in relation to radiographs. The diagnosis of calculus is the main reason for the scaling and polishing in Case Example 2. It should be remembered that gingivitis caused by plaque, can be cured through self-care practices of the patient. Obviously, this will require appropriate oral hygiene instructions to be given to the patient which may have to be followed up. A diagnosis of plaque or gingivitis, without a diagnosis of calculus or extrinsic staining, certainly does not warrant professional tooth cleaning. It is the calculus that the patient cannot remove that vindicates a decision to perform a scaling and polishing. The appropriate ICD-10 code is therefore "K03.6 - accretions (deposits) on teeth". The chronic gingivitis (K05.1) is only a secondary diagnosis in this instance. The same applies to the oral hygiene instructions (8151) for this case specifically. It should be noted that if the oral hygiene instructions were given for a different reason, such as to correct harmful brushing techniques, causing abrasion, then the ICD-10 code for abrasion would have applied. The reporting of procedure code 8120 when completing a treatment plan with the ICD-10 code being Z01.2.
CASE EXAMPLE 3
Patient arrives at your practice with a complaint of not being able to open his mouth. He complains of pain in the region of his wisdom teeth. An intra-oral examination reveals pain upon palpation on the retromolar pads. The 38 and 48 are partially erupted and present with a pericoronitis. The patient agrees to a panoramic radiograph which reveals that all four wisdom teeth are impacted. You document the following diagnosis on your records: "18,28,38,48 impacted horizontally; pericoronitis 38 and 48". You decide that it is indicated for the impacted teeth to be removed but the procedure is outside your field of expertise. After a discussion with the patient you mutually agree to referral to a maxillo-facial and oral surgeon. You write a prescription for medication to relieve the pain and infection. You report "K05.2 - Acute periodontitis" on the prescription as the diagnosis.
The invoice after treatment is as follows:
Discussion
Refer to Case Example 1 for an explanation of the use of Code Z01.2 in relation to the examination, infection control as well as the sterilised instrumentation. It can be argued that the panoramic radiograph was taken based on a clinically substantiated diagnosis of impacted teeth. Therefore K01.1 applies. However, the options of Z01.2 or Z01.6 may also be correct. If the diagnosis could not be confirmed before the radiograph was taken then the correct ICD-10 code should either be Z01.2 or Z01.6. Also note that the reason for the prescription was the pericoronitis and not the impactions, therefore the correct ICD-10 code to report on the prescription is K05.2 - Acute periodontitis"..
CASE EXAMPLE 4
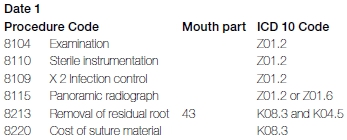
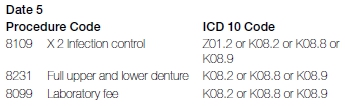
A 68 year-old patient requests a new denture as the existing plate no longer fits. She complains of a tender area in the 43 region. After obtaining informed consent and financial informed consent for the diagnostic procedures an intra-oral examination and a panoramic radiograph reveals generalised bone resorption due to the historic tooth loss and reveals a retained root 43. You document the following diagnosis on your records according to HPCSA requirements: "43 retained root with a chronic periapical periodontitis; illfitting denture due to bone resorption of the edentulous arch". Following receiving an explanation of the problems, the patient provides informed consent and financial informed consent for you to remove the retained root today and to continue with the denture at a later stage.
The invoice after treatment is as follows:
The subsequent invoices are as follows:
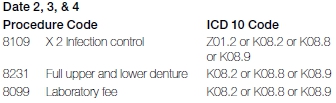
The accounts submitted to the medical aid fund administrator the completed denture:
Discussion
Refer to Case Example 1 for an explanation of the use of code Z01.2 in relation to the examination and infection control as well as the sterilised instrumentation. It should be noted that multiple options exist for the later treatment visits. Z01.2 will however be valid because an examination is needed before every step. The ICD-10 code that should be reported for the removal of the retained root is K08.3 but has a secondary diagnosis of chronic periapical periodontitis (K04.5). The sutures are used because an incision was required.
Additional comments
When reporting trauma, please do not forget to report the Cause Code.
The External Cause Codes (ECC):
These are required to be submitted with all primary ICD 10 CODES beginning with an S or a T
An ECC code can NEVER be used on its own or in the primary position.
Examples:
S02.51 FRACTURE OF TOOTH, OPEN
S02.50 FRACTURE OF TOOTH, CLOSED
The following External Cause codes could be used to describe how the fracture occurred, but an external cause code must be submitted.
V28.20 Motorcycle rider injured in no collision transport accident, unspecified motorcycle rider, no traffic accident, whilst while engaged in sports activity
V18.50 Pedal cyclist injured in no collision transport accident, passenger, traffic accident, while engaged in sports activity
W04.31 Fall while being carried or supported by other persons, sports and athletics area, while engaged in leisure activity
We hope that these examples will provide you with some assistance as to the correct use of ICD-10 codes. Should you require any further clarity, please do not hesitate to contact Dr Mehroon Khan at the SADA Head Office for assistance.
* periodontal charting/screening is a prerequisite to claim an 8101.
