










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Primary Health Care & Family Medicine
On-line version ISSN 2071-2936Print version ISSN 2071-2928
Afr. j. prim. health care fam. med. (Online) vol.17 n.1 Cape Town 2025
https://doi.org/10.4102/phcfm.v17i1.4972
ORIGINAL RESEARCH
Assessment of pediatric eye care services in health facilities in the Ashanti region of Ghana
Elizabeth M. Akpakli; Alvin J. Munsamy; Nishanee Rampersad
Discipline of Optometry, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Childhood visual impairment is an important public health concern considering the social, emotional and economic consequences. Lack of access to eye care services contributes to this growing problem. Therefore, integrating primary eye care into existing primary healthcare would facilitate improved access to equitable, effective and affordable eye care services, particularly for children.
AIM: The study assessed the provision of primary paediatric eye care services in health facilities in the Ashanti region of Ghana.
SETTING: The study was conducted at the primary health facilities in the Ashanti region of Ghana.
METHODS: Stratified random sampling was used to select 145 health facilities in this descriptive study. The eye care professionals in these facilities completed a questionnaire concerning primary eye care services for children. Data were analysed using descriptive and inferential statistics.
RESULTS: Eye care services were available in 131 (90%) of the health facilities resourced with essential eye equipment. Refraction services were provided by 129 (98.5%) despite limited coverage by the national health insurance scheme. More than 80% of participants lacked continuing education and 59% had poor awareness of management guideline. Barriers identified included lack of specialised equipment and inadequate resources.
CONCLUSION: The study highlights disparities in the provision of child eye care services among the health facilities in the Ashanti region of Ghana.
CONTRIBUTION: This study provides useful information to inform policy on targeted interventions for child eye care services to ensure accessible, equitable and comprehensive services.
Keywords: visual impairment; provision; primary eye care services; children; health facilities.
Introduction
The World Health Organization (WHO) reports that approximately 19 million children are visually impaired and 1.4 million are blind.1 Children with visual impairment experience social, emotional and economic challenges and are less likely to attend school and attain employment.2 Childhood visual impairment is a critical consideration not only for the number of affected children but also because of the number of years the surviving child must live with the visual impairment.3 Lack of access to eye care services is recognised as an important reason for why people remain or become blind.4 The prevalence of vision impairment in low- and middle-income regions is four times higher than in high-income regions.5 Therefore, there is a need for low- and middle-income countries (LMICs) to provide universal access to eye care, not just for sight threatening conditions but also for conditions that cause functional limitations. Researches globally support the integration of primary eye care into existing primary healthcare (PHC) systems as a viable solution to improving access and reducing avoidable blindness.6,7 In this regard, PHC forms an integral part of the health system in a country and a central point for social and economic development of every community.8 Primary healthcare is designed to be the first level of health service contact for individuals, families and communities and the national health system at large.9 In this model, appropriately trained health personnel can diagnose and manage common eye conditions at the community level and refer more complex cases through an established care pathway.10 The WHO's Global Action Plan for Universal Eye Health (2013-2019) highlights the role of PHC workers in delivering primary eye care and emphasises the need for capacity-building and systems integration. Despite this, literature specific to Ghana remains limited, particularly regarding the availability of paediatric eye care services at the PHC level.
Therefore, the aim of this study was to assess the provision of primary paediatric eye care services in health facilities in the Ashanti region of Ghana. These results will provide valuable insights into the current lack of data and help guide primary eye care planning and policy making for child eye care.
Research methods and design
Study design
The study used a cross-sectional design to assess the provision of eye care services among children in primary health facilities in the Ashanti region of Ghana. The health facilities were visited once, and different cadres of eye care professionals, such as ophthalmologists, optometrists, ophthalmic nurses and opticians, were assisted to complete a semi-structured questionnaire.
Study area and population
The study was conducted in the Ashanti region of Ghana located in the southern part of Ghana. The region has 43 districts and 195 sub-districts. The Ashanti region of Ghana has a well-developed health sector with 530 health facilities comprising Community-Based Health Planning and Services (CHPS) facilities, health centres, clinics, maternity homes, district hospitals and teaching hospitals. Most of these health facilities are operated by the Ghana Health Service (n = 170) and private institutions (n = 281) with the remaining by missions (n = 71) and the Ashanti quasi-government (n = 8). The population comprised eye care professionals from the primary health facilities.
Sample size and sampling technique
The health facilities were selected using stratified random sampling, where health facilities in each district were considered as the strata and selected for inclusion by simple random sampling. Stratified sampling with equal allocation was applied to select the health facilities from each district. Four health facilities were randomly chosen from each district, resulting in a total of 172 health facilities. At the health facilities, an eye care professional, such as an optometrist, ophthalmic nurse and optician, was then selected randomly to fill the questionnaire. Health facilities that did not provide eye care services were excluded - facilities that do not provide services designed to prevent, diagnose and treat paediatric eye conditions.11 The eye care professionals were eligible for the study if they were working at the facility for at least 3 years prior to the period of data collection.
Data collection
Data collection was over a period of 17 months from March 2023 to July 2024. The questionnaire used for data collection was developed based on validated scales from previous research.12 It was semi-structured, consisting of both open-ended and close-ended questions. The questionnaire was piloted on 16 participants, not included in the final sample, where input for improvement was given. The questionnaire (Appendix A) was modified based on feedback received concerning question format, type, order and flow to suit the study objective. After providing consent, the eye care professionals were assisted, via teaching and research assistants, to fill the paper questionnaire. Data from the completed paper questionnaire were thereafter entered into a Google Form. Data were extracted from the paper questionnaire for the following broad themes, including demographic data, knowledge and skills about child eye services, type of equipment available and cost of eye care services and if these services were covered by the National Health Insurance Scheme (NHIS).
Data analysis
Quantitative data were extracted into Microsoft Excel and analysed with STATA 14. Descriptive statistics, including means, standard deviations (s.d.), percentages and frequency distributions, are used to summarise demographic information and survey responses. The chi-square test was used to test the association between years of professional practice and awareness of guideline. A p-value of less than 0.05 was considered statistically significant.
Ethical considerations
Ethical clearance to conduct this study was obtained from the Kwame Nkrumah University of Science and Technology, Kumasi Committee on Human Research, Publication and Ethics (No. CHRPE/AP/771/22) and the University of KwaZulu-Natal Humanities and Social Sciences Research Ethics Committee (HSSREC) (No. HSSREC/00004574/2022). Gatekeeper permission was also sought from the regional health directorate and the heads of the selected health facilities. Participation was voluntary, and all participants provided informed consent before the study began.
Results
Demographic characteristics
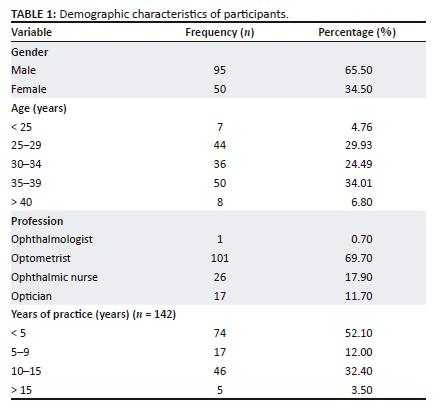
A total of 145 health facilities were assessed where one eye care professional working in each facility was contacted to fill the questionnaire, resulting in 145 eye care professionals. This comprised 95 (65.5%) males and 50 (34.5%) females. The mean age (s.d.) of the participants was 32.5 (6.13) years. The eye care professionals included 101 (69.7%) optometrists, 26 (17.9%) ophthalmic nurses, 17 (11.7%) opticians and 1 (0.7%) ophthalmologist. More than 60% of participants (n = 91) had less than 10 years of practice experience (Table 1).
Range and availability of child eye care services
Table 2 shows the range of services available for children in the health facilities. The majority of facilities provided refraction services (n = 129, 98.5%), followed by binocular vision services (n = 68, 51.9%), low vision services (n = 43, 32.8%), 15 (11.5%) other services such as colour vision test and seven (5.3%) provided surgical services. In instances where eye care services were not available, complex eye conditions were referred to (n = 23), while basic eye conditions were managed (n = 6) at their facilities. The majority of participants reported organising school screenings (n = 113).
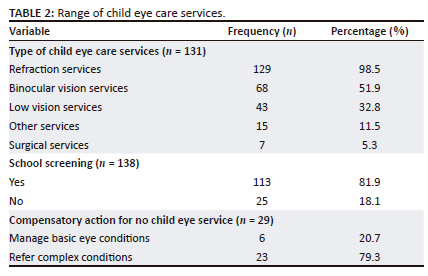
Figure 1 shows the availability of child eye care services in their health facilities as reported by participants (n = 144) and range of eye care services. Of these, more than 90% provided eye care services for children (n = 131), while the remaining (n = 13) did not provide any services for children.
Resources for child eye services
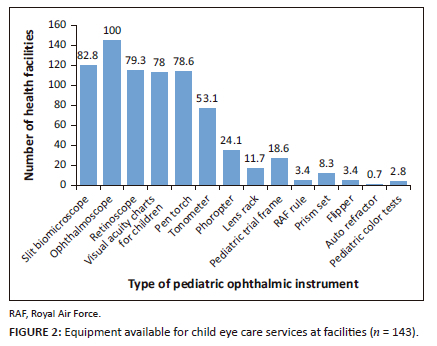
Figure 2 presents the availability of equipment necessary for the provision of eye care services for children in the different health facilities. All participants reported that an ophthalmoscope was available. As shown in Figure 2, a high proportion of the facilities also had slit lamp biomicroscopes (82.8%), retinoscopes (79.3%), pen torches (78.6%), visual acuity charts for children (78%) and tonometers (53.1%), while a lower proportion of facilities had phoropters (24.1%), paediatric trial frames (18.6%), lens rack (11.7%), prism set (8.3%), Royal Air Force (RAF) rules (3.4%), flippers (3.4%), paediatric colour charts (2.8%) and autorefractors (0.7%).
Knowledge and skills about child eye services
As shown in Table 3, 22 (15.2%) participants indicated that they had additional training in child eye care services, of only nine were for management of child conditions, six for low vision and rehabilitation services and three for paediatric dispensing. Participants (84.8%) who lacked additional training stated different reasons for this, including lack of finances (10.42%), lack of interest (15.6%), lack of opportunity (53.12%), few years in practice and paediatrics not included in job description (20.8%).
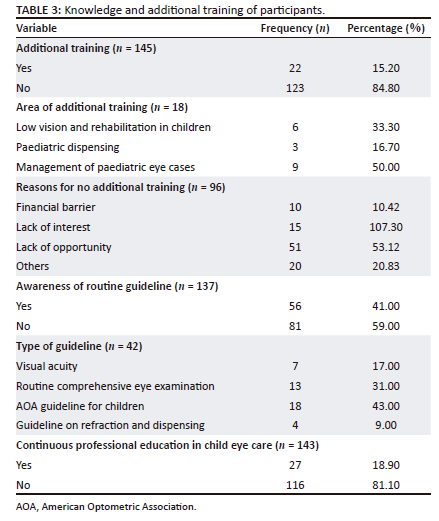
Approximately 40% of participants were aware of guidelines for the management of eye conditions in children (Table 3). When asked about the type of guideline, the American Optometric Association (AOA) guideline was most commonly reported (n = 18), followed by a routine comprehensive eye examination guideline (n = 13), visual acuity guideline (n = 7) and refraction and dispensing guideline for children (n = 4). Less than 20% of participants engaged with continuous professional educational activities related to child eye services (Table 3).
There was no significant association found between the two groups by experience greater or less than 10 years and awareness of guideline 
Sponsorship of child eye services
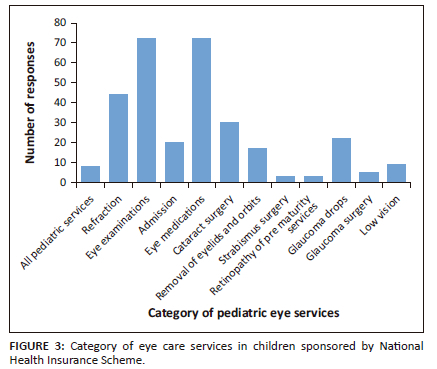
The majority of participants noted that the NHIS does not sponsor child eye care services (n = 107, 74.8%). For those who indicated NHIS coverage, eye examinations and eye medication were most commonly mentioned, while other services and fees including refraction, cataract surgery and payment for admission were also mentioned, as shown in Figure 3.
Challenges and barriers to eye care services in children
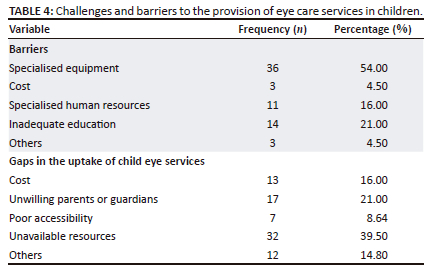
Table 4 shows that the barriers to the provision of eye care services for children included specialised equipment as the main barrier while inadequate public education, specialised human resources and cost were lesser barriers. Barriers to the uptake of child eye care services included unavailable human and physical resources as the major barriers to uptake, while delays in seeking treatment by parents and guardians, cost of services and poor accessibility to eye clinics because of distance were considered as minor barriers.
Discussion
The study sought to report on the provision of primary eye care services among children in health facilities in the Ashanti region of Ghana. Overall, eye services for children were available in the region, with refraction services being the most common and provided mostly by optometrists working in these health facilities. Despite this, most eye care professionals indicated not having additional training and managed basic conditions while referring complex conditions for further management. In this study, most of the eye care professionals were males aligning with workforce trends reported in a similar study in Southern Ethiopia.13 There were more optometrists and ophthalmic nurses in the sample suggesting that these eye care professionals served as the providers of primary eye care services in the communities. A recent study14 noted a similar trend and stated that optometrists and ophthalmic nurses are vital role players in providing primary eye care services. Furthermore, the eye care workforce in the Ashanti region of Ghana is relatively young, considering that most participants had less than 10 years of professional experience.
Range and availability of child eye care services
Early detection and intervention for eye conditions among children are crucial for improving global child health outcomes. In this study, there was a high level of provision of child eye care services, as more than 90% of participants reported providing these services. This finding is encouraging and aligns with efforts aimed at prioritisation of avoidable childhood blindness considering the profound impact of visual impairment in children.12 However, the absence of child eye care services in some of the health facilities suggests an inequity of services in some communities underscoring the need for the ministry of health to intervene and implement interventions to ensure that eye care services are available and accessible in all health facilities. A structured referral system was used in health facilities that lacked child eye care services where complex eye conditions were referred, ensuring that affected children received advanced care. This approach has also been used previously where community nurses identify people with vision impairment and advise on non-optical interventions, make referrals and facilitate access to advanced low vision services.15 It demonstrates the importance of referral systems to bridge service delivery gaps that may exist to ensure that the appropriate services are assessed and afforded.
Majority of participants reported organising school screening activities that are an essential and effective strategy for the early detection and management of eye conditions in school children. Such strategies aim to reduce the impact of visual problems and improve academic performance in children, particularly in LMICs.16 Almost all health facilities provided refraction services indicating that detection and correction of refractive error is widely available. This can be attributed to the high number of optometrists in the districts unlike in a study in Zambia where refractive error correction services were limited.17 The provision of eye care services for refractive error is crucial, as uncorrected refractive error (URE) is a readily treatable cause of visual impairment globally.18 Binocular vision services were the second most common type of child eye care services and support a previous study that highlighted the availability of such services in Ghana.19 The provision of binocular vision services helps detect and effectively manage ocular problems, indirectly improving academic performance among children. Low vision services, such as assessments and provision of assistive devices, were available at approximately one-third of the health facilities, which is concerning given the increasing prevalence of vision impairment worldwide. This gap in the provision of low vision services is well known, as it is one of the most underprovided services globally, especially in Africa.15 Early identification and treatment of eye conditions among children are crucial for their visual and cognitive development; hence, it is recommended that policymakers prioritise provision of low vision services by improving funding for equipment and staff training. The focus on refraction services, while critical, suggests an imbalance in service provision. Therefore, it is recommended that eye care professionals undergo additional training and that health facilities be better equipped to offer comprehensive primary eye care services for children.
Resources for child eye services
The role of human and physical resources is crucial for delivering accessible and high-quality eye care services. In general, most health facilities had basic diagnostic equipment that are necessary to provide eye care services. Ophthalmoscopes, which enable examining the ocular health, were available at all health facilities as has been reported previously.20 This availability and the use of ophthalmoscope are essential for accurate diagnosis and management of various posterior ocular conditions. A high proportion of health facilities were also equipped with slit lamp biomicroscopes and retinoscopes, which are also critical for ocular health and refraction procedures, respectively. A recent study21 in the Pacific also noted a similar finding among mid-level eye care workers concerning accessibility of slit lamp biomicroscopes and retinoscopes. Additionally, other tools including pen torches and visual acuity charts specific for children were widely available similar to findings in a study in Oman.22 Taken together, the availability of these equipment supports the examination and diagnostic processes involved in child eye care services. Fewer facilities had tonometers indicating a potential gap in assessment of intraocular pressure in children that is important for diagnosing glaucoma. The inadequate availability of tonometers could delay diagnosis of paediatric glaucoma, increasing the likelihood of irreversible optic nerve damage and visual impairment. This study noted limited availability of advanced tools, such as phoropters, paediatric trial frame, lens racks, prism sets, RAF rules, flippers, paediatric colour charts and autorefractors, which are needed to effectively assess and manage a wide range of visual functions and refractive errors in children. This lack of additional equipment for providing comprehensive eye care services for children creates potential barriers to the availability of good-quality primary eye care services. Overall, the disparity regarding equipment in some of the health facilities underscores the need for improved resource distribution and increased funding to enhance eye care service delivery and achieve universal eye coverage in the Ashanti region of Ghana.
Knowledge and skills of eye care professionals about child eye services
Engaging in competency-based and continuous education is crucial to improve patient care and provide sustainable high-quality eye care. Less than 20% of participants had additional training in child eye care services, highlighting a significant gap in specialised paediatric eye care and provision of its services. Similar results have been found in studies involving primary eye care providers in another African country.13 The lack of additional training for child eye care may lead to inefficient services, and staff should be encouraged to engage in courses, workshops and webinars focused on paediatric eye care to expand and update their knowledge and skills. The major reasons noted for lack of additional training were lack of opportunity and lack of interest. Lack of opportunity may be because of limited access to training programmes and resources. Without adequate resources, even motivated professionals may struggle to receive the necessary education and hands-on experience. Preference for other specialties and perceived low priority may cause lack of interest in child eye care. This aligns with a previous study23 that noted child eye care not being a priority in many African healthcare systems. Hence, it is essential to expand child eye care training programmes and integrate them into existing health education systems. Funding for infrastructure and scholarships should be also increased to improve access to specialised training. Additionally, raising awareness about the importance of child eye care through continuing professional development initiatives may help generate greater interest in this field.
One in every four participants was aware of guidelines for managing eye conditions in children. The varying guidelines followed in these facilities may lead to inconsistent diagnostic and treatment outcomes for eye conditions among children. To address the adoption and use of varying guidelines, it is recommended that all eye care providers in these health facilities undergo training using a standardised evidence-based curriculum for child eye care services. Furthermore, mechanisms should be implemented, following the training, to monitor adherence to the principles and guidelines contained in the curriculum. It is concerning to note that less than 20% of participants engaged in continuing professional education activities related to child eye services, as such activities help eye care professionals remain updated to provide evidence-based care. In Tanzania, PHC staff displayed improved knowledge in eye care after undergoing periodic training programmes.24 In this study, there was no association between years of experience and awareness of management guidelines for child eye conditions. In contrast, a study suggests that awareness and familiarity with eye examination guidelines improves with age and experience.25
Sponsorship of child eye services
Health insurance schemes are recognised as a useful tool to finance provision of healthcare services in developing countries with the potential to increase utilisation of these services, better protect against health expenses and address issues of equity.26 Most of the participants reported that the NHIS does not sponsor child eye care services reflecting a knowledge gap among these eye care professionals as eye care services are covered by the NHIS in Ghana.26 Hence, there is a need to improve awareness about NHIS policies and benefits concerning eye care services among eye care professionals and patients. Additionally, regular audits of NHIS implementation should be conducted in health facilities to assess compliance and identify inconsistencies. Eye examinations and medications were noted as common benefits of the NHIS consistent with a previous finding that the NHIS in Ghana covers some eye care services, but not spectacles and optical devices.27 The limited coverage for refractive and cataract surgery services is concerning because such services are necessary to curb the common treatable causes of visual impairment, particularly among children in LMICs. Therefore, there is a need for better engagement of policymakers on the public health and economic benefits of covering refractive and cataract surgery services in Ghana.
Challenges and barriers to child eye services
Barriers to accessing child eye care services children are wide ranging and encompass factors that hinder children from obtaining these services leading to negative consequences.28 The lack of specialised equipment, high cost of services, limited specialised human resources and inadequate public education were noted as barriers to the provision of child eye services in this study. Inadequate specialised equipment and limited human resources significantly affect the provision of child eye care services in developing countries as has been noted in a study in Swaziland.29 To overcome this, the ministry of health, private sectors and non-governmental organisations should collaborate and work more efficiently towards providing essential ophthalmic instruments and staff in the health facilities to enhance service provision. High cost of services was noted as a barrier to accessing service, and this was also noted in the present study. To address this, NHIS should expand its coverage to make eye care services more affordable for poor families, and private sponsors should be contacted to organise free community eye screening programmes to help identify eye problems for prompt interventions. Similarly, gaps concerning the uptake of these services included cost of services, unwillingness of parents to seek prompt interventions, poor accessibility because of long distances to eye clinics and unavailable human and physical resources. Delayed presentation because of parental attitude and distance can cause further deterioration and potentially lead to visual impairment in children. Consequently, community education programmes to raise and improve awareness about the importance of early detection and prompt intervention for eye conditions are necessary. Additionally, it is recommended that community outreach activities be organised in underserved populations to improve access to eye care services in an effort to reduce the burden of avoidable visual impairment.
Limitations
The results of this study reflect the provision of child eye care services in health facilities from only one region of Ghana and therefore cannot be generalised to the whole country. Additionally, the exclusion of facilities that do not provide eye care services could have introduced a selection bias consequently preventing generalisation of the study findings. Furthermore, this study used a survey with data being self-reported and could have introduced recall bias. Additionally, this cross-sectional study does not provide an in-depth understanding of the participants' responses. Therefore, future studies should use qualitative methods of data collection such as interviews and focus groups to investigate provision of primary eye care services among children in these health facilities.
Conclusion
Child eye care services were available in the Ashanti region of Ghana, with refractive services being the most common with notable gaps being in low vision provision. Disparities need to be addressed to ensure that equitable and comprehensive child eye care services are available to reduce the prevalence of avoidable visual impairment beyond refractive error. Few participants had further training and knowledge of paediatric eye care guidelines suggesting that targeted interventions are needed to improve knowledge, skills and quality of child eye care services. The limited NHIS coverage for child eye care services presents a significant barrier, and expanding the scope of NHIS and improving awareness of covered services are critical towards achieving equitable and sustainable child eye care services. Understanding and addressing the barriers to the provision and uptake of child eye care services are essential for improving accessibility and equity, which can potentially reduce the burden of avoidable visual impairment in children.
Acknowledgements
The authors would like to express their thanks to the University of KwaZulu-Natal for allowing them to do their research. They are also grateful to all eye care professional who contributed their knowledge and expertise to the completion of this research. This article is partially based on E.M.A.'s thesis entitled 'Assessment of pediatric eye care services in health facilities in the Ashanti region of Ghana' towards the degree of Doctor of Philosophy in Optometry at the College of Health Sciences, University of KwaZulu-Natal, South Africa with supervisors Prof. A.J. Munsamy and Dr N. Rampersad.
This article is based on data from a larger study. A related article focusing on the perspectives of district health directors regarding the integration of primary eye care services for children has been published in African Vision and Eye Health, Volume 84(1), Article a1053, https://doi.org/10.4102/aveh.v84i1.1053. The present article addresses a distinct research question, focusing on the availability, resources, and professional capacity for delivering pediatric eye care services within primary health facilities.
Competing interests
The authors declare that they have no financial or personal relationship(s) that may have inappropriately influenced them in writing this article.
Authors' contributions
E.M.K. contributed towards the conceptualisation, methodology, data collection, formal analysis and writing of the manuscript. A.J.M. and N.R. assisted with supervision, project administration, review and editing, conceptualisation and methodology.
Funding information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability
The datasets generated and analysed during this study are not publicly available because of confidentiality but can be obtained from the corresponding author E.M.K. upon reasonable request.
Disclaimer
The views and opinions expressed in this article are those of the authors and are the product of professional research. It does not necessarily reflect the official policy or position of any affiliated institution, funder, agency or that of the publisher. The authors are responsible for this article's results, findings and content.
References
1. Amiebenomo OM, Achugwo DC, Abah I. Parental knowledge and attitude to children's eye care services. Niger J Paediatr. 2016;43:215. https://doi.org/10.4314/njp.v43i3.11 [ Links ]
2. Ramai D, Elliott R, Goldin S, et al. A cross-sectional study of pediatric eye care perceptions in Ghana, Honduras, and India. J Epidemiol Glob Health. 2015;5:133-142. https://doi.org/10.1016/j.jegh.2014.06.004 [ Links ]
3. Decarlo DK, McGwin G, Bixler ML, et al. Impact of pediatric vision impairment on daily life: Results of focus groups. Optom Vis Sci. 2012;89:1409-1416. https://doi.org/10.1097/OPX.0b013e318264f1dc [ Links ]
4. Aghaji A, Burchett HED, Oguego N, et al. Primary health care facility readiness to implement primary eye care in Nigeria: Equipment, infrastructure, service delivery and health management information systems. BMC Health Serv Res. 2021;21:1-11. https://doi.org/10.1186/s12913-021-07359-3 [ Links ]
5. Bourne RRA, Flaxman SR, Braithwaite T, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: A systematic review and meta-analysis. Lancet Glob Health. 2017;5:e888-e897. https://doi.org/10.1016/S2214-109X(17)30293-0 [ Links ]
6. Christian BiN, Shomuyiwa DO, Christian NG, et al. Integrating eye care into primary healthcare in Nigeria: Challenges of the primary healthcare workforce. Public Health Chall. 2024;3:e191. https://doi.org/10.1002/puh2.191 [ Links ]
7. Kadam YP. Integrating primary health care with primary eye care boon or bane. IHOPE J Ophthalmol. 2023;2:14-16. https://doi.org/10.25259/IHOPEJO_35_2022 [ Links ]
8. Druetz T. Integrated primary health care in low- and middle-income countries: A double challenge. BMC Med Ethics. 2018;19(Suppl 1):48. https://doi.org/10.1186/s12910-018-0288-z [ Links ]
9. Uzochukwu BSC, Onwujekwe OE, Ezumah N. the District Health System in Enugu State, Nigeria: An analysis of policy development and implementation. Afr J Health Econ. 2014;03:01-14. https://doi.org/10.35202/ajhe.2014.3203 [ Links ]
10. Du Toit R, Faal HB, Etya'Ale D, et al. Evidence for integrating eye health into primary health care in Africa: A health systems strengthening approach. BMC Health Serv Res. 2013;13:1-15. https://doi.org/10.1186/1472-6963-13-102 [ Links ]
11. Mafwiri M, Malik AN. Primary eye health care: What do young children need? Community Eye Health. 2021;34:84-85. [ Links ]
12. Gilbert C, Foster A. Childhood blindness in context of VISION 2020: The right to sight: A global initiative to eliminate avoidable blindness. Bull World Health Organ. 2001;79:227-232. [ Links ]
13. Kentayiso TW, Nkoane NL, Matlhaba KL. Primary eye care service provision ability of mid-level healthcare providers in southern Ethiopia. Afr Vis Eye Health. 2024;83:931. https://doi.org/10.4102/aveh.v83i1.931 [ Links ]
14. Alhrizi KHA, Mohammed M, Alkhalaf H, et al. The important role of optometrist and qualified nursing in primary healthcare for eye care. J. Posit Psychol Wellbeing. 2022;6:473-478. [ Links ]
15. Chiang PPC, Keeffe JE. Improving access to low vision services. Community Eye Health J. 2012;25:15. [ Links ]
16. Opare A, Abdullahi LH, Minnies D, et al. School vision screening programmes in reducing uncorrected refractive error among children in Low and Middle-Income countries-LMIC (systematic review). Adv Ophthalmol Vis Syst. 2020;10:91-105. https://doi.org/10.15406/aovs.2020.10.00392 [ Links ]
17. Kapatamoyo E, Sialubanje C, Muma KI, et al. Availability of refractive error correction services in selected Zambian hospitals: A cross-sectional quantitative study. BMJ Open. 2023;13:e070297. https://doi.org/10.1136/bmjopen-2022-070297 [ Links ]
18. Resnikoff S, Jonas JB, Friedman D, et al. Myopia - A 21st century public health issue. Investig Ophthalmol Vis Sci. 2019;60:Mi-Mii. https://doi.org/10.1167/iovs.18-25983 [ Links ]
19. Opoku-Baah C, Mohammed AK, Afari C, et al. The management of binocular vision anomalies by eye care facilities in the accra and kumasi metropolises (Ghana). Int J Innov Appl Stud. 2014;9:1401-1408. [ Links ]
20. Patel D, Mercer E, Mason I. Ophthal ophthalmic equipment survey 2010: Preliminary results. Community Eye Health J. 2010;23:22-25. [ Links ]
21. Tousignant B, Pearce MG, Julie B, et al. State of the eye health system in the Pacific: Is medical technology available and used by mid-level eye care workers? Rural Remote Health. 2020;20:239-245. https://doi.org/10.22605/RRH5109 [ Links ]
22. Khandekar R, Mohammed AJ. Health facilities for primary eye care in Sultanate of Oman: Primary eye care study 2000. Sultan Qaboos Univ Med J. 2006;6:21-26. https://doi.org/10.18295/2075-0528.2614 [ Links ]
23. Alrasheed SH, Elmadina AEM. Effect of binocular vision problems on childhood academic performance and teachers' perspective. Pak J Ophthalmol. 2020;36:162-167. https://doi.org/10.36351/pjo.v36i2.896 [ Links ]
24. Mafwiri MM, Jolley E, Hunter J, et al. Mixed methods evaluation of a primary eye care training programme for primary health workers in Morogoro Tanzania. BMC Nurs. 2016;15:1-10. https://doi.org/10.1186/s12912-016-0163-5 [ Links ]
25. Moustafa GA, Liebman DL, Kabarriti G, et al. Primary care provider familiarity and compliance with preferred practice patterns for comprehensive eye examinations. Am J Ophthalmol. 2023;247:127-136. https://doi.org/10.1016/j.ajo.2022.10.003 [ Links ]
26. Gobah FK, Zhang L. The National Health Insurance Scheme in Ghana: Prospects and challenges: A cross-sectional evidence. Glob J Health Sci. 2011;3:90-101. https://doi.org/10.5539/gjhs.v3n2p90 [ Links ]
27. Wiafe B. On our own feet: Preparing for the donor to leave. Community Eye Health J. 2013;26:45-46. [ Links ]
28. Borrel A, Dabideen R, Mekonen Y, et al. Child eye health in Africa. The status and way forward. The African Child Policy Forum. Cape Town: ORBIS Africa; 2013. [ Links ]
29. Sukati VN, Moodley VR, Mashige KP. A situational analysis of eye care services in swaziland. J Public Health Afr. 2018;9:167-173. https://doi.org/10.4081/jphia.2018.892 [ Links ]
 Correspondence:
Correspondence:
Elizabeth Akpakli
elizabethakpakli@gmail.com
Received: 11 Mar. 2025
Accepted: 07 July 2025
Published: 16 Sept. 2025
Appendix A: Questionnaire for eye care professionals

