










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
On-line version ISSN 2078-676XPrint version ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.40 n.2 Pretoria Jul. 2024
https://doi.org/10.7196/SAJCC.2024.v40i2.1905
RESEARCH
Critical care nurses' orientations to caring for patients and their families at a selected hospital in KwaZulu-Natal
W EmmamallyI; M JugroopII
IPhd; School of Nursing and Public Health, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IIMSN; School of Nursing and Public Health, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND. Caring in a critical care environment may be conceptualised differently compared with other nursing disciplines because of the patient's critical condition and the specialised staffing categories and skills. However, critical care nurses who prioritise caring can meaningfully connect with critically ill patient and their families, resulting in positive healthcare outcomes.
OBJECTIVE. To assess critical care nurses' orientations to caring for critically ill patient and their families.
METHODS. A quantitative, descriptive, cross-sectional study was conducted with 139 purposively sampled critical care nurses working in a tertiary referral hospital in KwaZulu-Natal, South Africa. Data were collected using the Caring Assessment for Caregivers questionnaire, and analysis included descriptive and comparative statistics.
RESULTS. The overall mean score of critical care nurses' orientations to caring was 116.01 (range of 25 - 125). Of the five subscales (dimensions), the dimension of 'Maintaining belief' had the highest mean score of24.25 and the dimension of 'Being with' had the lowest mean score of 22.70 (range 5 - 25).
CONCLUSION. While critical care nurses reported high overall orientations to caring, lower mean scores on the subscale 'Being with' suggest that there are areas for critical care nurses to grow in their role as carers. Further research using qualitative approaches may shed valuable insights into how the critical care environment impacts the caring orientations of critical care nurses.
Keywords: Caring, critical care nurses, patients, families, orientation.
Caring within a critical care environment constitutes patient- and family-focused care tailored to this specialised environment.[1] Caring in a critical care environment specifically involves integrating processes that require nurses' vigilance to meet the biopsychosocial needs of critically ill patients and their families.[2,3] Furthermore, it requires the critical care nurse (CCN) to be both competent and experts in the sophisticated environment of advanced technology, while displaying caring behaviours crucial for achieving positive health outcomes for the patients and their families.[4] These positive patient outcomes include open communication among nurses, families and patients, improved patient and family satisfaction with care, higher survival rates, shorter hospital stays, decreased anxiety of families and optimistic recovery outlooks.[5] According to Emmamally and Brysiewicz,[6] caring for critically ill patients and their families enables nurses to develop respectful, dignified and non-judgmental relationships. This care allows CCNs to understand the cultural differences, beliefs and values among the diverse patients they nurse.[4]
CCNs may face barriers in their work environment that influence their ability to express care.[1] Factors such as insufficient staffing, limited physical resources, high patient acuity and intense workloads result in limited opportunities for CNNs to display caring behaviours towards patients.[7] The preoccupation of CCNs with the technology used in monitoring critically ill patients also limits their chances of developing meaningful relationships with patients and their families. These factors combined may alter CCNs' orientations to caring.[8] In examining CCNs' orientations to caring, we focus on their perceptions or positions regarding the value of caring and the importance of developing caring relationships with critically ill patients and their families. Watson[9] explains that caring behaviours move nurses beyond clinical efficacy, making caring the norm in all therapeutic patient-nurse interactions. Nurses who value caring use each patient interaction to create unique opportunities for connecting and healing for the patient and the family. [9] Thus, CCNs who express high orientations to caring can combine caring behaviours with technical savvy and objective assessment to provide quality care to critically ill patients and their families.[10]
The ongoing dilemma of caring for critically ill patients v. their stabilisation often brings CCNs to moments of reckoning, questioning whether caring for patients and families is negotiable. As such, the study objective was to assess CCNs' orientations to caring for critically ill patients and their families at a selected hospital in KwaZulu-Natal (KZN), South Africa (SA). A secondary objective was to determine the association between CCNs' demographic characteristics and their scores in the dimensions of caring.
Methods
A cross-sectional, descriptive study was conducted in six specialised adult critical care units within a tertiary referral hospital in KZN. These units include cardio-thoracic, medical, surgical, coronary, neurologic and trauma-critical care. The hospital serves a catchment area of ~10 million people from a culturally diverse population in KZN and parts of the Eastern Cape bordering KZN.
Population, sample and sampling
Purposive sampling was used to identify the study population. We included 151 professional nurses with either a nursing diploma or degree, with or without a specialisation in critical care nursing, who had been working in any of the six critical care units for at least 12 months. The sample size of 139 nurses was calculated based on the statistical parameters, where the proportion assumption was 0.8 and the confidence interval 1.96. To account for potential attrition, approximately six more participants were added to the sample, resulting in a minimum sample size of 145 CCNs.
Data collection instrument
Respondents completed a demographic questionnaire of five characteristics and the Caring Assessment for Caregivers' (CACG) Questionnaire developed by Steele-Moses et al.[11] Permission to use the questionnaire was obtained from the developers by the researchers. The CACG questionnaire consists of five subscales, also referred to as the dimensions of caring, with five scaled items in each of the five dimensions, designed to determine a caregiver's orientation to caring. The dimensions of caring include: Dimension One (Maintaining belief), Dimension Two (Knowing), Dimension Three (Being with), Dimension Four (Doing for) and Dimension Five (Enabling). These dimensions describe how nurses provide care, emphasising the importance of being emotionally present and connected with their patients.[11]
Each item of the dimensions is ranked on a Likert scale ranging from 1 to 5, where 1 represents low caring behaviour situated to the left side of the scale and 5 represents high caring behaviour positioned on the right side of the scale.[11] The total score per dimension ranges from 5 - 25, with the instrument total score ranging from 25 - 125. The higher the score, the higher the caring orientation of the caregiver.[12]
The content validity index for the dimensions ranges from 0.70 - 0.93, while the content validity index of the instrument is acceptable at 0.84.[11] In this study, content validity was determined by aligning the objectives of the study to the dimensions of the CACG questionnaire. A specialist CCN with international and national critical care experience established the face validity of the questionnaire.
Internal consistency of the CACG for the study was established through Cronbach's Alpha. The CACG questionnaire was piloted with CCNs working in the critical care units. The results of the pilot study were not included in the main study, and there were no changes made to the CACG. The value for Cronbach's Alpha for the CACG was α = 0.98, showing excellent internal consistency. A similar overall internal consistency of 0.939 was obtained by Steele-Moses et al. The reliability scale for the five dimensions ranged from 0.77 - 0.80.
Recruitment and data collection
Recruitment and data collection occurred between October and December 2021. The plan for recruitment of respondents and data collection followed the guidelines for data collection during COVID-19 (level 2) outlined by the ethics committee of the University of KwaZulu-Natal (BREC/00002770/2021 and the Department of Health (DoH) in KZN (NHRD REF: KZ_202109_005). The guidelines specified options for electronic data collection or mandatory protocols of social distancing and the use of protective personal equipment for contact data collection. The guidelines sought to protect the rights and safety of participants during the pandemic.
The researcher arranged a meeting with the nursing service manager of the selected hospital to discuss the study, obtain approval and seek input on the hospital management's preferred methods for participant recruitment and data collection. The researcher presented the options of electronic surveys using Survey Monkey or the traditional method of recruiting participants through staff meetings and handing out questionnaires to willing participants. The management preferred the traditional method of handing out questionnaires, influenced by the decline in COVID-19 statistics and increased healthcare worker vaccination compliance in KZN.
As part of recruitment, posters with information about the study were posted on all bulletin boards of the critical care units, making the CCNs aware of the study. Additionally, hospital management permitted the researcher to liaise with the unit managers of each critical care unit to meet with both day and night CCN staff, introduce the study and invite them to participate.
Following the recruitment meeting, the researcher handed out information and consent sheets to CCNs who consented to participate, and a locker was secured in each of the six units where completed questionnaires were deposited. The researcher collected the questionnaires from the lockers.
Data management and analysis
Data were transferred from the survey forms into an SPSS spreadsheet and analysed using SPSS version 27 (IBM, USA). Descriptive statistics of frequencies, percentages and means were used to summarise the data on demographics and responses to items of the CACG. The Pearson χ2 test was used to establish any associations between the respondents' computed scores of the five dimensions and their demographic characteristics. Significance was set at p<0.05.
Ethical considerations
Data recruitment and collection occurred once ethical approval was obtained from the Biomedical Research Ethics Committee (BREC/00002770/2021) and permission from the DoH KZN (NHRD REF: KZ_202109_005). The hospital management also gave permission and facilitated the study. The study adhered to the Nuremberg Code and the Declaration of Helsinki to protect the respondents. All respondents provided informed consent after the study had been explained to them, including the assurance of their right to withdraw without reprisal from the study if they felt uncomfortable. Participants were guaranteed anonymity as no names were used and all data were treated confidentially.
Results
Demographic profile
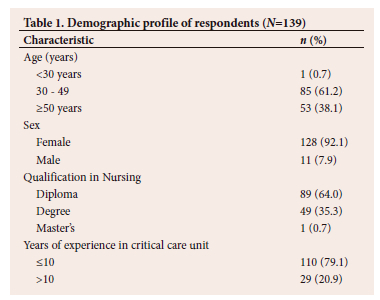
Of the 145 CCNs sampled for the study, 139 responded, giving a response rate of 95.6%. The percentages of CCNs in the age groups of <30, 30 - 49 and >50 years were 0.7% (n=1), 61.2% (n=85) and 38.1% (n=53), respectively. One hundred and twenty-eight (92.1%) of the respondents were female, 64.0% (n=89) had a Diploma in Nursing and the majority of the respondents (79.1%; n=110) had <10 years of critical care experience (Table 1).
The mean total score for the orientation of caring was 110.0 (standard deviation (SD) 7.5). To identify the dimensions of caring most and least important to the respondents, we calculated the mean total scores for each of the five dimensions. The dimension Maintaining belief had the highest mean score (24.3) and the dimension 'Being with had the lowest mean score (22.70).
In examining the association of demographic characteristics and the mean scores of each of the five dimensions, we found a significant negative association between age and the dimension 'Being with' (r=-0.182, p=0.032). Likewise, sex had a positive association with the dimension 'Maintaining belief (p=0.015). The results further indicated the association between sex and the dimension 'Being with was weak but positive and significant (r=0.251, p=0.003) (Table 2).
Discussion
Caring in a critical care unit requires patient-focused and specialised care within a work-intensive and technologically focused environment,[2,13] the same characteristics that influence how caring unfolds within a critical care environment.[1]
The researchers highlight the favourable response rate of the current study (96.0%), indicating that CCNs willingly participated in a study on caring despite facing the physical and psychological challenges of working during the COVID-19 pandemic. As in most nursing studies, there was variability in the age of the respondents and a predominance of female nurses. Of note, in a study focusing on caring, women are often regarded as carers, with the societal expectations of caring aligning more with women rather than men.[14,15] In the current study, the majority (72.7%) of the participants had >10 years of work experience. This is a positive finding as a study on nurses' perceptions of caring in Iran identified that nurses with more years of experience may perform with considerable competence and skills in many of the caring behaviours.[16]
Despite the challenges of a labour-intensive critical care environment, the findings of the current study revealed that CNNs had high orientations to caring (mean 116, range 25 - 125). The findings of high caring orientations among CCNs were also observed in the study by Peacock-Johnson,[12] where the mean total score of caring using the CACG was 107.15.
The trend of a high overall orientation to caring identified in this study also permeated the five dimensions of caring, with the dimension of 'Maintaining belief having the highest mean score of 24.25. 'Maintaining belief in caring implies an essential belief in individuals and their ability to endure life events and transitions and come out with purpose.[17] The authors add that fundamental to maintaining beliefs is the nurses' ability to bolster the hope and faith of patients and their families. A study in the Middle East concluded that the factors of type of nursing assignment, limited time and poor management support of CCNs can significantly influence caring behaviours associated with maintaining beliefs.[18] In interpreting the positive results obtained in the current study, it is also important to consider which factors expressed by Modic et al.[18] could impact the caring behaviours of the respondents in this study. The dimension of caring 'Being with' had the lowest orientation to caring (mean 22.70). This dimension focuses on caring behaviours consistent with nurses' being physically and emotionally present with the patients and their families. The finding almost mimics the results of a study conducted by Joonbakhsh and Pashaee,[19] where the analysis revealed a mean score of 22.75. The finding is also congruent with the conclusions of Peacock-Johnson's[12] study, which investigated nurses' orientations to caring using a relationship-based model. The study revealed that the nurses' low orientations in the dimension of 'Being with' reflects how nurses are unable to spend time at patients' bedsides because of competing demands for their time.
Associations of the dimensions of caring and the demographic characteristics of respondents showed a weak, negative association between age and the dimension of 'Being with' with younger nurses having a higher caring orientation than older nurses. Although older CCNs are more skilled and productive, they are more vulnerable to compassion fatigue in the critical care environment because of repeated exposure to traumatic events.[20] Previously, there was a focus on the biomedical model in teaching and learning, whereas currently there is a shift towards relational models.[12] Relational models transform the healthcare environment to facilitate relationship-based care, therapeutic nurse-patient relationships and patient-centred care that enables dignity with patient values and preferences. This could account for the difference in caring behaviours between older and younger nurses.[21]
There was a positive association between the demographic characteristic of sex and the dimension of 'Maintaining belief, with female nurses having a higher caring orientation than their male counterparts. A recent study by Shalaby et al.[1] revealed contrasting findings showing no significant associations between caring behaviours and the demographic characteristics of age and sex.
Study limitations and recommendations
The respondents were from one hospital in KZN and therefore the results may not be generalised to CCNs working in other hospital settings with dissimilar conditions to those of the tertiary hospital used in this study. Another limitation was that demographic data collection did not include the variable of a critical care qualification. The results on this variable would have brought to light significant associations between a critical care qualification and nurses' orientations to caring. The study found that critical care nurses had a low orientation to caring in being emotionally and physically present with patients and families. It would be interesting to conduct a mixed methods study where a qualitative arm would provide possible explanations for this result. There is also a concomitant need for care modules specifically designed to focus on building relational and therapeutic skills of nurses for both undergraduate and postgraduate critical care modules, using simulations and reflective sessions as teaching aids and methodologies. There could be comparative studies in state-funded v. private sector hospitals, with the important conclusions revealing how resources impact the caring orientation of nurses.
Conclusion
A significant and recurring result in studies using the CACG is the low scores obtained in the dimension 'Being with' The result highlights a global concern that CCNs place less value on physically interacting and emotionally connecting with critically ill patients and their families. The respondents reported a high overall orientation to caring aligned with the results of other studies using the same questionnaire. The study was conducted at a time when critical care nurses were reeling from the demands and helplessness of the COVID-19 pandemic and revealed positive results on the commitment of CCNs to caring for patients at families. Perhaps this study gives added meaning to the phrase, 'caring against all odds'.
Declaration. We declare that this article is our original work and take full responsibility for its content and authenticity.
Acknowledgements. We acknowledge the respondents of this study for their participation.
Author contributions. Both authors contributed to the article's conception, design and writing. MJ contributed to data collection and data analysis.
Funding. None.
Data availability statement. The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Conflicts of interest. None.
References
1. Shalaby S, Janbi N, Mohammed K, Al-harthi K. Assessing the caring behaviors of critical care nurses. J Nurs Educ Pract 2018;8(10):77-85. https://doi.org/10.5430/jnep.v8n10p77 [ Links ]
2. Castro-Palaganas E. Caring and nursing research: What nurses do best. Philipp J Nurs 2022;90(1):1-2. https://www.researchgate.net/publication/343384210_Editorial_Caring_and_Nursing_Research_What_Nurses_Do_Best [ Links ]
3. Limbu S, Kongsuwan W, Yodchai K. Lived experiences of intensive care nurses in caring for critically ill patients. Nurs Crit Care 2018;24(1):9-14. https://doi.org/10.1111/nicc.12349 [ Links ]
4. Bagherian B, Sabzevari S, Mirzaei T, Ravarya A. Meaning of caring from critical care nurses perspective: A phenomenological study. J Intensive Crit Care 2017;03(3:33).1-9. https://doi.org/10.21767/2471-8505.100092 [ Links ]
5. Wei H, Watson J. Healthcare interprofessional team members' perspectives on human caring: A directed content analysis study. Int J Nurs Sci 2019;6(1):17-23. https://doi.org/10.1016/j.ijnss.2018.12.001 [ Links ]
6. Emmamally W, Brysiewicz P. Families' perceptions of support from healthcare professionals in the three emergency departments in KwaZulu-Natal, South Africa. IJANS 2019;10:55-60. https://doi.org/10.1016/j.ijans.2019.01.004 [ Links ]
7. Salimi S, Azimpour A. Determinants of nurses' caring behaviors (DNCB): Preliminary validation of a scale. J Caring Sci 2013;2(4):269-278. [ Links ]
8. Lofty Abdel-Aziz A, Sayed Ahmed SE, Abd El-Hakeem YG. Family needs of critically ill patients admitted to the intensive care unit, comparison of nurses and family perception. Am J Nurs Sci 2017;6(4):333-346. https://doi.org/10.11648/j.ajns.20170604.18 [ Links ]
9. Watson J. Unitary caring science: Philosophy and praxis of nursing. University Press of Colorado; 2018. [ Links ]
10. Ahmed FR, Saifan A R, Dias JM, Subu MA, Masadeh R, AbuRuz ME. Level and predictors ofcaring behaviours of critical care nurses. BMC Nurs 2022;21,341:1-8. https://doi.org/10.1186/s12912-022-01125-41-8 [ Links ]
11. Steele-Moses S, Koloroutis M, Ydarraga DM. Testing a "Caring Assessment for Care Givers" Instrument. Creat Nurs 2011;17(1):43-50. https://doi.org/10.1891/1078-4535.17.1.43 [ Links ]
12. Peacock-Johnson AJ. Nurses' perception of caring using a relationship-based care model. J Comp Nurs Res Care 2018;3(128):1-5. https://doi.org/10.33790/jcnrc1100128 [ Links ]
13. Enns C, Sawatzky J. Emergency nurses' perspectives: Factors affecting caring. J Emerg Nurs 106;42(3):240-245. https://doi.org/10.1016/j.jen.2015.12.003 [ Links ]
14. Barrett-Landau S, Henle S. Men in nursing: Their influence in a female dominated career. J Leadersh Instr 2014;13(2):10-13. https://api.semanticscholar.org/CorpusID:44974873 [ Links ]
15. W Zhang, Liu Y-L. Demonstration of caring by males in clinical practice: A literature review. Int J Nurs Sci 2016;3(3):323-327. https://doi.org/10.1016/j.ijnss.2016.07.006 [ Links ]
16. Rostami S, Esmaeali R, Jafari H, Cherati, J. Perception of futile care and caring behaviors of nurses in intensive care units. Nurs Ethics 2017;26(1):248-255. https://doi.org/10.1177/0969733017703694 [ Links ]
17. Mårtensson S, Hodges E, Knutsson S, et al. Caring behavior coding scheme based on Swanson's Theory of caring - development and testing among undergraduate nursing students. Scand J Caring Sci 2020;35(4):1123-1133. https://doi.org/10.1111/scs.12927 [ Links ]
18. Modic M, Siedlecki S, Griffin M, Fitzpatrick J. Caring behaviors: Perceptions of acute-care nurses and hospitalised patients with diabetes. Int J Hum Caring 2016;20(3):160-164. https://doi.org/10.20467/1091-5710-20.3.160 [ Links ]
19. Zamanzadeh V, Shohani M, Palmeh T. Nursing students' perception of instructors' caring behaviors in tabriz university of medical sciences. J Caring Sci 2015;4(1):55-62. https://doi.org/10.5681/jcs.2015.006 [ Links ]
20. Ndlovu E, Filmater C, Jordaan J, Heyns T. Professional quality of life of nurses in critical care units: Influence of demographic characteristics. S Afr J Crit Care 2022;38(1):39-43. https://doi.org/10.7196/sajcc.2022.v38i1.517 [ Links ]
21. Noveno N. Nurses and their caring behaviours: A study summary of the International Caring Behavior Index for Nurses deduced from different voices. COJ Nurs Healthcare 2018;1(5):99-103. https://doi.org/10.31031/cojnh.2018.01.000522 [ Links ]
 Correspondence:
Correspondence:
W Emmamally
Emmamally@ukzn.ac.za
Received 31 January 2024
Accepted 10 June 2024
Contribution of the study
The study aims to highlight the orientations of critical care nurses to different areas of caring. In so doing management can provide specific support to nurses to strengthen their caring abilities

{kind=link}