










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
On-line version ISSN 2078-676XPrint version ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.36 n.1 Pretoria Jan./Jul. 2020
https://doi.org/10.7196/sajcc.2020.v36i1.395
RESEARCH
Results from the first audit of an intensive care unit in Botswana
A O MilanI; M CoxII; K MolebatsiIII
IMD, MSc; OrcID 0000-0001-8567-9793; Department of Emergency Medicine, Faculty of Medicine, University of Botswana, Gaborone, Botswana
IIMD; OrcID 0000-0001-7781-1942; Faculty of Medicine and Public Health, University of Sydney, Australia
IIIMA; OrcID 0000-0002-9293-4470 Department of Statistics, Faculty of Social Sciences, University of Botswana, Gaborone, Botswana
ABSTRACT
BACKGROUND: Botswana is an economically stable middle-income country with a developing health system and a large HIV and infectious disease burden. Princess Marina Hospital (PMH) is the largest referral and teaching hospital with a mixed eight-bed intensive care unit (ICU
OBJECTIVES: To conduct an audit of PMH ICU in order to investigate major admission categories and quantify morbidity and mortality figures using a validated scoring system for quality improvement, education and planning purposes
METHODS: PMH medical records and laboratory data were accessed to record demographics, referral patterns, diagnoses, HIV status, Acute Physiologic Assessment and Chronic Health Evaluation (APACHE) II scores and mortality rates
RESULTS: A total of 182 patients >14 years of age were enrolled over a 12-month period from April 2017 - March 2018. Patient's mean age was 42.9 years, males represented 56.6% of the study population and surgical conditions accounted for 46% of diagnostic categories. Sixty percent of the patients were HIV-negative and 12% had no HIV status recorded. The mean APACHE II score was 25 and the mean length of stay in ICU was 10.3 days. Higher APACHE II scores were associated with higher mortality regardless of HIV status. The overall mortality was 42.8% and there was no difference in mortality rates in ICU or at 30 days between HIV-positive and HIV-negative ICU patient groups
CONCLUSIONS: The PMH ICU population is young with a high mean APACHE II score, significant surgical and HIV burdens and a high mortality rate. PMH ICU has significant logistical challenges making comparison with international ICUs challenging, and further research is warranted
Keywords: middle-income country, ICU, APACHE II score, clinical audit, HIV.
The intensive care unit (ICU) is slowly establishing itself in low-middle income countries (LMIC), including in sub-Saharan Africa (sSA). Few studies have been published on ICU services in sSA. However, they reveal multiple challenges, especially in limited bed capacity, infrequent resources and medical personnel.[1-4] Recent articles highlight the paucity of LMICs ICU data and the need for more research.[5,6] Botswana is an upper middle-income country in southern Africa with a population of over 2 million people. Princess Marina Hospital (PMH) in Gaborone, the capital city, is currently the largest publicly funded and university teaching hospital in Botswana with a 24-hour emergency department (ED), 567 inpatient beds and the most complete range of specialty services. PMH ICU is an 8-bed ward managed by specialists 24 hours, 7 days a week, assessing patient eligibility for admission and managing clinical care. These specialists consist of anaesthetists and one intensivist with formal ICU postgraduate training, but are only onsite Monday to Friday during normal working hours. There are no ICU registrars or ICU training programmes in the country; hospital medical officers are infrequently available from the ED to provide clinical support to the ICU. PMH ICU nurse to patient ratio is 1:2 during day shifts and 1:3 during night shifts with no formal ICU or critical care nursing education programmes in the country. PMH ICU has 24-hour access to radiology (X-rays, ultrasound, computed tomography (CT) scan) and basic laboratory investigations. Dietitians, physiotherapists, psychologists, occupational therapists and social workers are available on referral bases, but no clinical pharmacist is available. At the time of this study there were no endorsed official local ICU admission or management guidelines. Botswana has not escaped the large southern African burden of HIV, with a recent UNAIDS estimate of 370 000 adults aged 15 and over living with HIV in Botswana, representing 18.2% of the total population.[7] Botswana was one of the first countries in sSA to initiate HIV interventions, including highly active anti-retroviral treatment (HAART) with a local study showing significant improvements in HIV mortality since these initiatives.[8] A 2015 study of medical admissions to PMH revealed a continued high burden of HIV disease and opportunistic illnesses of tuberculosis (TB) and cryptococcal meningitis.191 To date, no clinical ICU studies have been conducted in Botswana and this PMH audit was initiated to describe demographics, major admission categories and baseline morbidity and mortality data. Morbidity and expected mortality in ICU settings worldwide are measured through scoring systems such as Acute Physiology and Chronic Health Evaluation II (APACHE II), Sequential Organ Failure Assessment (SOFA), Simplified Acute Physiological Score (SAPS) and Organ Dysfunction and Infection (ODIN) score. APACHE II score and SOFA scores are the more widely used scoring systems currently in ICU settings [10-12] A previous attempted audit in PMH ICU in 2011 was abandoned due to various health quality and governance issues, which are well-known issues in many LMICs.[13] Many of these issues are ongoing and limited the authors' initial intentions and planning for this study. Due to frequent logistic issues only APACHE II scoring was able to be recorded in this study. It is hoped that these data will inform clinicians, researchers and health administrators about the burden of critical care illness at PMH and in Botswana.
Objectives
To assess the basic demographic, referral characteristics and major diagnostic categories of the adult critically ill patients admitted to PMH ICU. To determine severity scoring, mortality data and complications of the adult patients admitted to ICU.
Methods
Study setting
The study was conducted at the major teaching and referral hospital for Botswana, PMH which has an eight-bed ICU, utilised for adult and paediatric patients. Adult patients in PMH are identified as patients 14 years and older.
Study population
The study population for this study were all critically ill adult patients admitted between 1 April 2017 and 31 March 2018.
Inclusion/exclusion criteria
All critically ill patients aged >14 years admitted to ICU at PMH were included in the study. Paediatric critically ill and ICU patients with burns were excluded from the study, as APACHE II scoring is not suitable for these types of critically ill patientsJ14,15]
Data collection
Demographic data that included age, gender, referral ward and admission diagnosis were extracted from the ICU notes by the study investigators. The diagnosis written in the patient's file by the ICU admitting doctor or doctor requesting ICU admission was used in this study.
This diagnosis was allocated to a specific category by a consensus of three of the study investigators and required support by clinical judgment as well as appropriate investigations recorded in the patient's file. Investigators extracted laboratory investigations from ICU observation charts, patient files and also from the Integrated Patient Management System (IPMS) of the hospital. If laboratory investigations, including HIV tests were not performed in the ICU admission, they were marked as absent. HIV status of adult patients at PMH was established by the standard HIV rapid test, confirmed by the ELISA test as per HIV national guidelines[16] Severity of the patients' condition was determined using the APACHE II scoring, assessed by two study investigators using the worst value of each parameter measured within the first 24 hours of admission to ICU.[17] In cases of a missing APACHE II parameter, a zero score was recorded. ICU-acquired complications were diagnosed and allocated using a published diagnostic criterion (Appendix 1: http://sajcc.org.za/public/sup/395.docx). Outcome was determined as ICU death rate and 30-day post-ICU discharge death rate, and its relationship with HIV status was studied. ICU death rate and 30-day post-ICU discharge death rate were determined as follows:[18]
To determine if the patient was alive or dead at 30 days, centralised electronic medical records were accessed through a password protected account with specific access approved by the hospital superintendent and ethics committees.
Data analysis
Data were analysed by SPSS version 24 (IBM Corp., USA), Stata version 14.2 (StataCorp., USA) and MedCalc version 19.0.6 (mdcalc.com).
A vtest of independence and Fisher's exact tests were used for univariate analysis. Continuous variables were analysed using the Student's t-test or λ-sample equality median test. A significance level of p<0.05 was used.
Ethical consideration
Permission to conduct the study was obtained from the Office of Research and Development, University of Botswana (ref. no. UBR/RES/ IRB/1738), the Research and Ethics Committee, Ministry of Health (ref. no. HPDME 13/18/1 X (845)), and Research and Ethics Committee, Princess Marina Hospital (ref. no. PMH 5/79(292-2-2017)).
Results
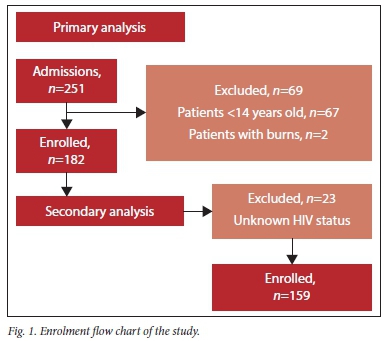
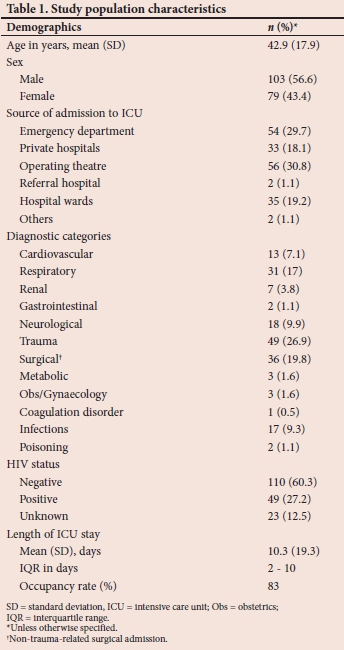
During the study period of 12 months from April 2017 to March 2018, 251 patients were admitted to the ICU at PMH. Of these, 182 adult patients were enrolled into the study database and 69 patients were excluded (Fig. 1). Patients with unknown HIV status were then excluded from further analysis. Table 1 shows the characteristics of the initial study population. The mean (SD) age of the enrolled patients was 42.9 (17.9) years, and males represented 56.6%. Over 60% of all admissions were from operating theatres or emergency departments and the two highest ranked admission diagnostic categories were surgical conditions. The study population was HIV-positive in 27.2% and 12.5% had an unknown HIV status. The incidence of patient complications at PMH ICU in the study period was 20.8%. Bacteraemia was the main complication acquired by patients in ICU, representing 52.6% of all complications recorded, followed by urinary tract infection and ventilator-associated tracheobronchitis in 15.8% and 13.2%, respectively.
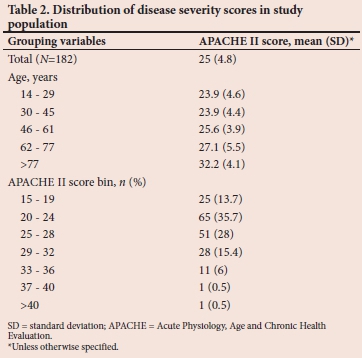
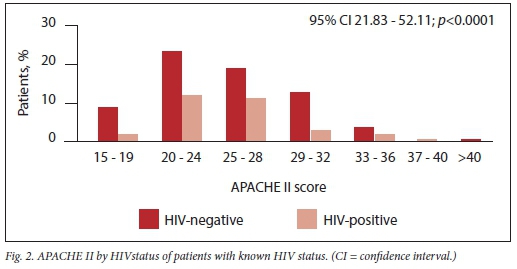
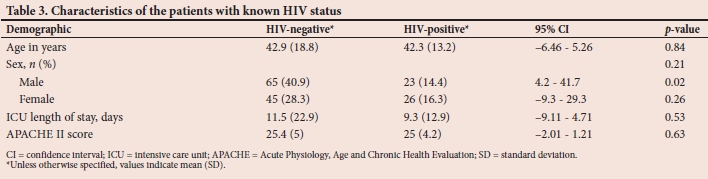
The mean APACHE II score in the first 24 hours of PMH ICU admission was 25; and the highest APACHE II scores were in patients aged over 77 years (Table 2). Once patients with unknown HIV status were excluded from analysis, patient demographics, length of stay and APACHE II scores were again analysed (Table 3). There were fewer HIV-negative patients than HIV-positive patients in both genders; however this was only statistically significant in males (p=0.02). Mean and median APACHE II scores were the same in both groups, but median ICU length of stay was greater in HIV-positive patients, but was not statistically significant (p=0.57). APACHE II scores were further analysed in age groups of HIV-positive and HIV-negative patient groups (Fig. 2). This analysis revealed HIV-negative groups overall had statistically significantly higher APACHE II scores than HIV-positive groups (p<0.0001). APACHE II scores of known HIV status patients who died in ICU are shown in Fig. 3A. Patients with APACHE II scores between 25 and 28 had the highest death rate in ICU, but none of these mortality differences in ICU or at 30 days (Fig. 3B) was statistically significant (p=0.21 and p=0.26, respectively). Overall ICU mortality for these patients was 42.8%.
Discussion
This PMH ICU study population was 57% male with a median age of 43 years. Regional and other African ICU studies show similar demographic findings to these, unlike in high-income ICU settings.[19-22] PMH operating theatre and emergency department accounted for over 60% of ICU admissions; with trauma and non-trauma related surgical conditions accounting for over 46% of all diagnostic categories. As PMH is the major surgical referral hospital for the entire country, and the
southern African region has a well-known high trauma burden, these factors could explain the higher surgical related burden compared with other regional ICUs.[23] The mean APACHE II score in our study was 25 and the majority of patients had scores between 20 and 28, comparable to European and US studies.[10,24] These high scores in PMH indicate poor patient physiological reserves and suggest advanced and perhaps delayed clinical presentations to this unit. The length of ICU stay was 10.3 days, similar to a regional adult ICU study length of stay of 11.8 days.[25] Other South African studies have shown disparate results[26, 27] reflecting differing predominance of HIV-positive patients or surgical populations. In the secondary analysis of the 159 patients with known HIV status, HIV-negative patients had statistically significant higher APACHE II scores than HIV-positive patients. This unexpected result could be explained by admitting doctors using stricter ICU admission criteria for HIV-positive patients. Lack of official ICU admission guidelines at the time of this study would have also impacted this finding. Ongoing research incorporating important HIV-related data such as viral load, CD4+ cell counts and HAART medication use compared with ICU outcomes is needed in this area. Mortality in the ICU increased exponentially in both groups of patients for each five-point increase in APACHE II score, with peak scores between 25 and 28. The exponential fall after the peak score can be explained by small numbers in these groups. This finding is similar to a US study where mortality at different APACHE II scores was comparable.[17] The 42.8% ICU mortality of the 159 patients whose HIV status was known is very high but similar to a small PMH ICU survey in 2015 where the mortality rate among surgical ICU patients (HIV status not recorded) was 46%.[28] Other studies carried out in the region[29-31] have reported similar results. However, international ICU mortality rates range between 8 and 18%.[32,33] There was no statistical significance in 30-day mortality rates in either group of patients with HIV known status; however, there are limited studies with which to compare our results. Akgün et al.[32] reported a statistically significant difference in 30-day mortality between HIV-infected (19%) v. non-infected patients (11%).
Study limitations
As this is the first clinical audit of an ICU in Botswana there were a number of limitations affecting data collection and interpretation. Firstly, it should be noted that based on the description of PMH ICU most of the basic international requirements for a tertiary ICU are not met[34,35] and the ICU does not comply with many of the recommendations for resource-limited settings.[5] The mixed nature of PMH ICU also makes international comparisons challenging, as many international ICU studies do not include patients aged between 14 and 18 years, as in our study. The frequent absence of onsite ICU physicians, significant lack of ICU medical, nursing and allied health staff impacts negatively on ICU expertise and reliability of results. These factors also make comparison of data with developed ICU centres difficult. This study records a small sample size of adult patients admitted to a small single mixed ICU in Botswana, not reflecting all critically ill patients in the country. Currently a government arrangement exists that when PMH ICU is full, patients requiring ICU care can be transferred to private sector ICUs in Botswana and their management costs paid by the Ministry of Health. There were two private ICUs in Gaborone at the time of this study. These patients were not included in the audit, but account for 18% of patients admitted to PMH ICU from private sector ICUs. PMH has no formal ICU electronic record database or international diagnostic coding system, leading to little opportunity to follow up on patients' outcomes including confirmed diagnoses. This study utilised the admission diagnosis only, which is frequently unreliable or incomplete as ICU diagnoses are regularly adjusted when new results are available during the patient's admission. HIV patients were not sub-categorised into those on HAART or those resistant to HAART which has pathophysiology implications to APACHE scores and mortality. Logistical issues including restricted access to pathological testing, any culture media for central venous catheter tip and respiratory secretion cultures, severely impacted diagnostic accuracy in this study. In a high HIV prevalence setting such as Botswana, the unavailability of 24-hour HIV testing, CD4+ cell counts and further microbiological support also limits diagnostic accuracy and assessment of HIV-positive patients in this ICU.
Conclusions and recommendations
This is the first prospective audit of adult ICU patients in Botswana, revealing a young population presenting with high mean APACHE II scores and significant surgical and HIV burdens. On secondary analysis, HIV-negative patients had higher APACHE scores than HIV-positive patients; however HIV status did not have any impact in ICU mortality or 30-day mortality rates. High (> 20) APACHE II scores at 24 hours were associated with higher inpatient ICU and 30-day mortality regardless of the HIV status of the patients.
We advocate for more ICU resources, research, training and education in Botswana. An electronic registry of all ICU patients is urgently required to provide support for diagnosis, management and logistics. This ICU database should use internationally validated quality indicators and with risk stratification tools to provide clinicians and health policy makers information, ensuring that the most appropriate care is given to the most critical patients in Botswana.
Declaration. None.
Acknowledgements. The authors acknowledge the support of Mrs Irelys L. Rosabal Benitez, computer science specialist, and Mr Joseph Joseph, medical librarian at University of Botswana. The authors express thanks to Dr Lesego Gabaitiri for their contributions with the design and the statistics, as well as Dr Jack Mkubwa, Dr Aurelio R. Fernandez, and Dr Carlos Medina Merino in their roles as fellow investigators in this study.
Author contributions. AOM: data collection, data analysis and interpretation of results as well as manuscript drafting. MC: interpretation of results, manuscript drafting and critical revision for important intellectual content. KM: assisted with study design and statistical analysis. Funding. This study was awarded with a research grant from University of Botswana with project number R1162.
Conflicts of interest. None.
References
1. Haniffa R, Pubudu De Silva A, de Azevedo L, et al. Improving ICU services in resource-limited settings: Perceptions of ICU workers from low-middle, and high-income countries. J Crit Care 2018;44:352-356. https://doi.org/10.1016/jjcrc.2017.12.007 [ Links ]
2. Joynt GM, Gopalan PD, Argent AA, et al. The Critical Care Society of Southern Africa consensus statement on ICU triage and rationing (ConICTri). S Afr Med J 2019;109(8b):613-629. https://doi.org/10.7196/samj.2019.v109i8b.13947 [ Links ]
3. Amaefule KE, Dahiru IL, Sule UM, et al. Trauma intensive care in a terror-ravaged, resource-constrained setting: Are we prepared for the emerging challenge? Afr J Emerg Med 2019;9(Suppl):S32-S37. https://doi.org/10.1016/j.afjem.2018.12.007 [ Links ]
4. Dünser MW, Towey RM, Amito J. Intensive care medicine in rural sub-Saharan Africa. Anaesthesia 2017;72(2):181-189. https://doi.org/10.1111/anae.13710 [ Links ]
5. Diaz JV, Elisabeth DR, Papali A, Adhikari NK, Ferreira JC. Global Critical Care: Moving forward in resource-limited settings. Ann Glob Health 2019;85(1):1-11. https://doi.org/10.5334/aogh.2413 [ Links ]
6. Malelelo-Ndou H, Ramathuba DU, Netshisaulu KG. Challenges experienced by health care professionals working in resource-poor intensive care settings in the Limpopo province of South Africa. Curationis 2019;42(1):1-8. https://doi.org/10.4102/curationis.v42i1.1921 [ Links ]
7. Joint United Nations Programme on HIV/AIDS. Country Factsheets Botswana. Geneva: UNAIDS, 2017. http://www.unaids.org/en/regionscountries/countries/botswana (accessed 27 Mach 2019) [ Links ]
8. Farahani M, Price N, El-Halabi S, et al. Trends and determinants of survival for over 200 000 patients on antiretroviral treatment in the Botswana National Program: 2002-2013. AIDS 2016;30(3):477-485. https://doi.org/10.1097/qad.0000000000000921 [ Links ]
9. Tlhakanelo JT, Tshikuka JG, Molefi M, Magafu MG, Masupe T, Matchaba-Hove R. HIV hospital admissions attributable to specific opportunistic infections and factors associated with them at a Botswana referral hospital. World J AIDS 2015;5(3):175-181. https://doi.org/10.4236/wja.2015.53020 [ Links ]
10. Cetin K, Irfan S, Seval I, et al. Mortality of adult intensive care units in Turkey using the APACHE II and SOFA systems (outcome assessment in Turkish intensive care units). Arch Med Sci 2018;14(3):510-515. https://doi.org/10.5114/aoms.2016.59709 [ Links ]
11. Iwona PG, Szymon B, Piotr L, Anna P, Mariusz P. Predictive value of the APACHE II, SAPS II, SOFA and GCS scoring systems in patients with severe purulent bacterial meningitis. Anaesthesiol Intensive Ther 2016;48(3):175-179. https://doi.org/10.5603/ait.a2016.0030 [ Links ]
12. Lee Y, Kim SJ, Kim YS, et al. The usefulness of the SOFA and APACHE II scoring systems for the early prediction of mortality in patients with dapsone poisoning. Hum Exp Toxicol 2019;38(3):280-287. https://doi.org/10.1177/0960327118806647 [ Links ]
13. Kediegile G, Madzimbamuto FD. Obstacles faced when conducting a clinical audit in Botswana. S Afr J Anaesth Analg 2014;20(2):127-131. [ Links ]
14. Sherif E. Prognostic indicators in acute burned patients - a review. J Acute Dis 2015;4(2):85-90. https://doi.org/10.1016/s2221-6189(15)30014-7 [ Links ]
15. Sheppard NN, Hemington-Gorse S, Shelley OP, Philp B, Dziewulski P. Prognostic scoring systems in burns: A review. Burns 2011;37(8):1288-1295. https://doi.org/10.1016/j.burns.2011.07.0173 [ Links ]
16. Ministry of Health. Handbook of the Botswana 2016 integrated HIV clinical care guidelines 2016. https://www.moh.gov.bw/Pubhcations/Handbook_HIV_treatment_guidelines.pdf (accessed 02 November 2016). [ Links ]
17. Knaus WA, Draper EA, Wagner DP, Jack E Z. APACHE II: A severity of disease classification system. Crit Care Med 1985;13(10):818-829. https://doi.org/10.1097/00003246-198510000-00009 [ Links ]
18. Basic statistical data used in acute care facilities. 1-34. www.jblearning.com/samples/0763750344/45561_CH01.pdf (accessed 20 January 2017). [ Links ]
19. Dunser MW, Towey RM, Amito J, Mer M. Intensive care medicine in rural sub-Saharan Africa. Anaesthesia 2017;72:181-189. [ Links ]
20. Prin M, Itaye T, Clark S, et al. Critical Care in a tertiary hospital in Malawi. World J Surgery 2016;40(11):2635-2642. [ Links ]
21. Anesi GL, Gabler NB, Allorto NL, et al. Intensive care unit capacity strain and outcomes of critical illness in a resource-limited setting: A 2-hospital study in South Africa. J Intens Care Med 2018: 0885066618815804. https://doi.org/10.1177/0885066618815804 [ Links ]
22. Gordon K, Allorto N, Wise R. Analysis of referrals and triage patterns in a South African metropolitan adult intensive care service. S Afr Med J 2015;105(6):491-495. https://doi.org/10.7196/samj.9007 [ Links ]
23. Smith ZA, Ayele Y, Mcdonald P. Outcomes in critical care delivery at Jimma University Specialised Hospital, Ethiopia. Anaesth Intens Care 2013;41(3):363-368. https://doi.org/10.1177/0310057x1304100314 [ Links ]
24. Sadaka F, Ethmane Abou El Maali C, Cytron MA, Fowler K, Javaux VM, O'Brien J. Predicting mortality of patients with sepsis: A comparison of APACHE II and APACHE III scoring systems. J Clin Med Res 2017;9(11):907-910. https://doi.org/10.14740/jocmr3083w [ Links ]
25. Sulieman H, El-Mahdi W, Awadelkareem M, et al. Characteristics of critically-ill patients at two tertiary care hospitals in Sudan. Sultan Qaboos Univ Med J 2018;18(2):190. https://doi.org/10.18295/squmj.2018.18.02.011 [ Links ]
26. Mkoko P, Raine R. HIV-positive patients in the intensive care unit: A retrospective audit. S Afr Med J 2017;107(10):877. https://doi.org/10.7196/samj.2017.v107i10.12298 [ Links ]
27. Pillai J, Yazicioglu C, Moeng S, et al. Prevalence and patterns of infection in critically ill trauma patients admitted to the trauma ICU, South Africa. J Infect Dev Countries 2015;9(7):736-742.https://doi.org/10.3855/jidc.5865 [ Links ]
28. Abstracts of the 44th Annual Meeting Surgical Research Society of Southern Africa. S Afr J Surgery 2016;54:172-223. [ Links ]
29. Jared T, Bryce H, Clement K, et al. The burden of surgical diseases on critical care services at a tertiary referral hospital in sub-Saharan Africa. Trop Doct 2013;43(1):27-29. https://doi.org/10.1177/0049475513480773 [ Links ]
30. Kedir SBA, Bayisa T, Wuletaw T. Admission patterns and outcomes in the medical intensive care unit of St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia. Ethiop Med J 2017;55(1):19-26. [ Links ]
31. Sendagire C, Lipnick MS, Kizito S, et al. Feasibility of the modified sequential organ function assessment score in a resource-constrained setting: A prospective observational study. BMC Anesthesiol 2017;17(1):12. https://doi.org/10.1186/s12871-017-0304-8 [ Links ]
32. Akgün KM, Tate JP, Pisani M, et al. Medical ICU admission diagnoses and outcomes in human immunodeficiency virus-infected and virus-uninfected veterans in the combination antiretroviral era. Crit Care Med 2013;41(6):1458-1467. https://doi.org/10.1097/ccm.0b013e31827caa46 [ Links ]
33. Adhikari NK, Fowler RA, Bhagwanjee S, Rubenfeld GD. Critical care and the global burden of critical illness in adults. Lancet 2010;376(9749):1339-1346. https://doi.org/10.1016/s0140-6736(10)60446-1 [ Links ]
34. Valentin A, Ferdinande P. ESICM working group on quality improvement,. Recommendations on basic requirements for intensive care units: structural and organizational aspects. Intens Care Med 2011;37(10):1575-1587. https://doi.org/10.1007/s00134-011-2300-7 [ Links ]
35. Marshall JC, Bosco L, Adhikari NK, et al. What is an intensive care unit? A report of the task force of the World Federation of Societies of Intensive and Critical Care Medicine. J Crit Care 2017;37:270-276. https://doi.org/10.1016/j.jcrc.2016.07.015. [ Links ]
36. Craven DE, Hjalmarson KI. Ventilator-associated tracheobronchitis and pneumonia: Thinking outside the box. Clin infect Dis 2010;51(Suppl 1):S59-S66. https://doi.org/10.1086/653051 [ Links ]
37. Laupland KB, Zygun DA, Davies HD, et al. Incidence and risk factors for acquiring nosocomial urinary tract infection in the critically ill. J Crit Care 2002;17(1):50-57. https://doi.org/10.1053/jcrc.2002.33029 [ Links ]
38. Cullum N, Deeks JJ, Fletcher AW, Sheldon TA, Song F. Preventing and treating pressure sores. Qual Health Care 1995;4(4):289-297. https://doi.org/10.1136/qshc.4.4.289 [ Links ]
39. Daniel B, Padmaja P, Young D, Booth MG, Smith A. Sepsis caused by bloodstream infection in patients in the intensive care unit: the impact of inactive empiric antimicrobial therapy on outcome. J Hosp Infect 2017. https://doi.org/10.1016/j.jhin.2017.09.031 [ Links ]
40. Gammon RB, Shin MS, Buchalter SE. Pulmonary barotrauma in mechanical ventilation: Patterns and risk factors. Chest 1992;102(2):568-572. https://doi.org/10.1378/chest.102.2.568 [ Links ]
 Correspondence:
Correspondence:
A O Milan
aortizmilan@gmail.com
Accepted 18 December 2019
Contribution of study
This study is the first published audit for an intensive care unit in Botswana. The findings are especially relevant for the development of critical care capacity in the country during the current COVID-19 pandemic. We advocate for the establishment of an ICU registry in the country to allow ongoing accurate research in the field of critical care medicine and to improve healthcare for all critically ill patients in Botswana.

{kind=link}
{kind=link}