










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.115 n.5b Pretoria Jun. 2025
https://doi.org/10.7196/samj.2025.v115i5b.3681
EDITORIAL
Designing a universal electronic health record system: Creating a reliable national health database for AI and its application in healthcare in South Africa
M NodikidaI; A HenneyII
ICEO, South African Medical Association, Pretoria, South Africa. mzulungilen@samedical.org
IIDepartment of Computer Science, Faculty of Natural Science, University of the Western Cape, Cape Town, South Africa
Digital technology and artificial intelligence (AI) are transforming industries worldwide, and healthcare is no exception. The application of AI in medicine dates back to the 1950s, with several pilot initiatives reportedly conducted in Africa during the early 1980s.[1]
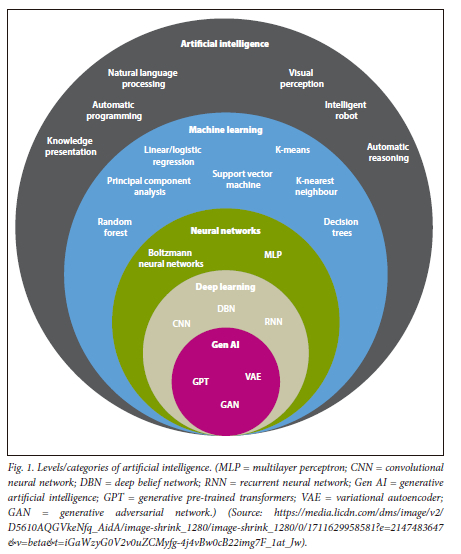
AI refers to a computer system's ability to perform tasks typically associated with human intelligence. These tasks include learning, decision-making, visual perception and speech recognition. Fig. 1 illustrates the different levels and categories of AI.
To effectively leverage AI and emerging technologies in healthcare, AI models require access to training datasets in which outcome variables (e.g. disease onset) are clearly defined. Establishing a centralised technological infrastructure, specifically a universal electronic health record (UEHR) system, for all South Africans is therefore a critical first step. Such a platform would enable the collection and integration of high-quality health data, supporting national healthcare planning and ultimately improving health outcomes.
One of the major challenges in applying AI to healthcare, particularly in low- and middle-income countries, is the lack of large, high-quality clinical datasets required to train advanced models such as deep learning.[2] Limited digitisation and the absence of integrated health records further compound this challenge. The availability of locally generated, representative, and high-quality health data is essential for developing reliable and unbiased AI systems tailored to local contexts.
This editorial outlines the proposed design of a UEHR system for all South Africans. The initiative is led by the South African Medical Association (SAMA) and is inspired by successful global models (Table 1), including those from the Nordic countries and the Taiwan Precision Medicine Initiative. Among these, Taiwan stands out as a global leader, having implemented a fully centralised, cloud-based and citizen-accessible electronic health record system that serves as a benchmark for countries aspiring to digitally transform their healthcare systems.
The first South African (SA) Presidential Health Summit was held in Boksburg on 19 - 20 October 2018, to address the systemic challenges facing the country's health sector.[3] One of the key outcomes of the summit was the recognition of the urgent need for a UEHR system.
Such a system would enable the creation of a comprehensive, up-to-date and continuous electronic medical record, accessible to healthcare professionals and patients across the country. At the time, the health information landscape was reported to be highly fragmented, with 42 disparate systems operating across SA's nine provinces (Fig. 2). Presently, this fragmentation significantly hinders efforts to provide integrated, efficient and patient-centred care, underscoring the necessity of a national UEHR solution.
An electronic health record (EHR), also referred to as an electronic patient record or electronic medical record, consolidates a patient's health information, care requirements and treatment plans into a unified digital format. It provides clinicians with a comprehensive, real-time overview of a patient's medical history, including diagnoses, medications, treatment plans, immunisation records, allergies, radiology images and laboratory test results.[4,5]
In essence, an EHR serves as a digital equivalent of a traditional paper chart or file (as still used in parts of SA), offering a dynamic and accessible record of a patient's healthcare journey.
A key success factor in the Taiwanese model is the interoperability of its national digital health architecture. Taiwan employs fast healthcare interoperability resources (FHIR) combined with application programming interfaces to enable the seamless exchange of health data between disparate healthcare systems and applications. This architecture ensures that health information can be consistently shared, accessed and updated across providers, and is fully integrated into a centralised national health database. Fig. 3 illustrates the Taiwanese model.
For SA to establish an effective EHR system, it is essential to first overcome barriers to interoperability and to develop a robust, integrated digital health ecosystem as the foundation.[6]
The 2018 Presidential Health Summit noted the establishment of an integrated UEHR system as a critical enabler for achieving universal health coverage (UHC) in SA. A universal EHR would provide a single, comprehensive medical record for each patient, across the public and private sectors, accessible nationwide, spanning all nine provinces. As Zharima et al.[6] have noted, this is not an impossible task.
Such a system would allow patients to seamlessly access healthcare at any level - primary, secondary, or tertiary - in both sectors, with their health records readily available and updated in real time at any point of care. Every interaction with the healthcare system, whether in Gauteng or the Eastern Cape provinces, would be captured in a unified, continuous health record.
SA's National Digital Health Strategy (2019 - 2024), now due for review, outlined four top priorities to drive health system transformation:
• digitisation of health systems business processes
• development of a complete EHR to improve patient management
• establishment of an integrated platform and architecture for the health information system
• ensuring interoperability and linkage of existing patient-based information systems.
However, 5 years since its adoption, progress has been limited, particularly in integrating the fragmented EHR systems between provinces in the public sector and those in the private sector.
In response, SAMA proposes a national public-private investment initiative to develop a universal EHR system for all South Africans. This initiative draws inspiration from the Taiwanese model, renowned for its centralised and interoperable architecture, but will be customised to meet SA's unique challenges and context.
As the national representative body for doctors, SAMA believes that strategic investment in the top four priorities of the digital health strategy, particularly in developing an integrated health information architecture, would represent a quantum leap toward achieving UHC.
This proposed UEHR architecture would enable interoperability between the public and private health systems at a national level, allowing for continuity of care and the development of a reliable national data source to support healthcare research and innovation. Ultimately, it would empower SA to implement predictive and precision medicine at scale, contribute meaningfully to improving national health outcomes, and position the country as a leader in addressing major global health challenges.
Conclusion
The implementation of a unified EHR system leveraging FHIR (Fig. 4) will bring about significant improvements to healthcare delivery. Firstly, it will promote seamless continuity of care by allowing healthcare providers across different provinces to access comprehensive and up-to-date patient records. This will ensure consistent, co-ordinated and effective treatment regardless of location.
Secondly, it will reduce redundancy by minimising the duplication of medical tests and procedures, leading to considerable savings in both time and resources. Thirdly, it will enhance clinical outcomes by providing healthcare professionals with accurate and complete patient information, supporting more informed and timely decision-making.
Furthermore, the use of standardised FHIR resources will greatly improve data interoperability, enabling consistent and efficient data exchange across diverse healthcare systems and institutions.
In addition, the integration of AI into this unified system further elevates its capabilities. AI agents can assist clinicians with early disease prediction, accurate detection, timely diagnosis and personalised treatment recommendations. By analysing large volumes of patient data, AI can uncover hidden patterns, identify risks and suggest evidence-based interventions, thereby improving diagnostic accuracy and clinical efficiency. Collectively, these advancements contribute to a more efficient, interoperable and patient-centred healthcare ecosystem.
References
1. Naidoo S, Bottomley D, Naidoo M, Donnelly D, Thaldar DW Artificial intelligence in healthcare: Proposals for policy development in South Africa. S Afr J Bioethics Law 2022;15(1):11-16. https://doi.org/10.7196/SAJBL.2022.v15i1.797 [ Links ]
2. Owoyemi A, Owoyemi J, Osiyemi A, Boyd A. Artificial intelligence for healthcare in Africa. Front Digit Health 2020;2:66. https://doi.org/10.3389/fdgth.2020.00006 [ Links ]
3. National Department of Health, South Africa. Presidential Health Summit Report. Pretoria: Government of South Africa, 2019. [ Links ]
4. Akanbi MO, Ocheke A, Agaba E, et al. Use of electronic health records in sub-Saharan Africa: Progress and challenges. J Med Trop 2012;14(1):1-6. [ Links ]
5. Oluwaseyi T. Electronic patient record (EPR) system in South Africa: Information storage, retrieval and share amongst clinicians. Cape Town: University of the Western Cape, 2006. https://www.sylff.org/wp-content/uploads/2015/03/Tokoshi-SRA-Article-web.pdf (accessed 23 May 2025). [ Links ]
6. Zharima C, Griffiths F, Goudge J. Exploring the barriers and facilitators to implementing electronic health records in a middle-income country: A qualitative study from South Africa. Front Digit Health 2023;5:1207602. https://doi.org/10.3389/fdgth.2023.1207602 [ Links ]

{kind=link}
{kind=link}
{kind=link}
{kind=link}