










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.103 n.4 Pretoria Apr. 2013
EDITORIALS
Africa's roads - the deadliest in the world
M PedenI; O KobusingyeII; M E MononoIII
ICo-ordinator, Unintentional Injury Prevention, Department of Violence and Injury Prevention and Disability, World Health Organization, 20 Avenue Appia, Geneva, Switzerland
IIResearch Fellow, School of Public Health, Makerere University, Kampala, Uganda, and Research Fellow, University of South Africa, Johannesburg, South Africa
IIITechnical Officer, Violence and Injury Prevention and Disability, World Health Organization Regional Office for Africa, Cité du Djoué, Brazzaville, Democratic Republic of Congo
The World Health Organization (WHO) released the Global Status Report on Road Safety 2013: Supporting a Decade of Action[1] in March 2013, in Geneva, Switzerland. The report presents 2010 data for 182 participating countries and provides a baseline for monitoring the Decade of Action for Road Safety (2011 - 2020) declared by the United Nations General Assembly through resolution 64/255 in 2010.[2] The goal of the Decade is to reduce the increasing trend in road traffic deaths, and to save an estimated 5 million lives over the period.
The report shows that about 1.24 million road traffic deaths occurred throughout the world in 2010, indicating a plateau since the publication of the first status report in 2009.[3] Middle-income countries have the highest annual road traffic fatality rate at 20.1/100 000, compared with 8.7 and 18.3/100 000 in high- and low-income countries, respectively. Half of the world's road traffic deaths occur among so-called 'vulnerable road users' - pedestrians (22%), cyclists (5%) and motorcyclists (23%).
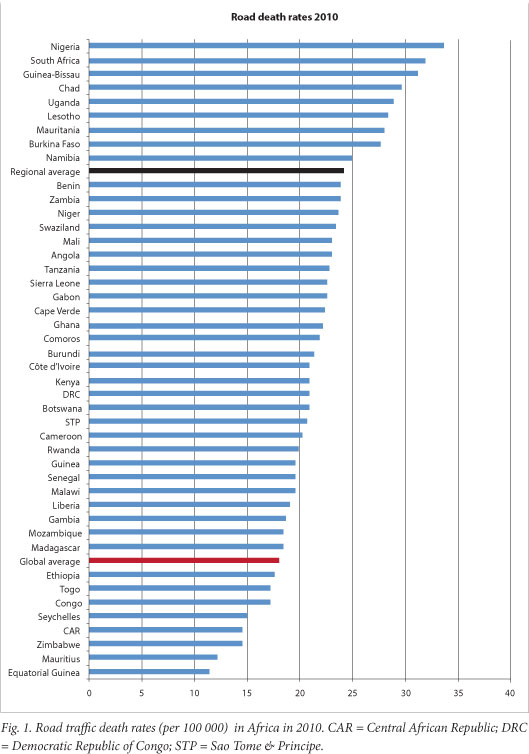
Forty-four of the 46 countries that make up the WHO African Region participated in the survey, covering 95.1% of the region's population. Data show that, despite Africa being the least motorised of the world's 6 regions (it only has 2% of the world's registered vehicles), the risk of dying as a result of a road traffic collision is highest in the African Region at 24.1/100 000 population (the global rate is 18/100 000).
Nigeria and South Africa have the highest road traffic death rates (33.7 and 31.9/100 000, respectively) and, together with the Democratic Republic of Congo, Ethiopia, Kenya, Tanzania and Uganda, account for 64% of all road traffic deaths in the region (Fig. 1).
The majority of the people killed on Africa's roads are young breadwinners - 62% are aged between 15 and 44 years - and 3 out of every 4 deaths are of males. Vulnerable road users - pedestrians, cyclists and riders of motorised two- and three-wheelers -constitute more than half (52%) of those killed on the roads, with pedestrians alone accounting for 37%.
Alongside these stark figures, it is clear that many African countries are beginning to take road safety more seriously. Almost all countries have a lead agency; however, only 12 countries have funded programmes with targets set for reductions in deaths and injuries. These lead agencies are tasked with addressing infrastructural, vehicular and road user legislative issues.
In brief, the status of road safety in Africa is as follows:
- Thirty-one countries conduct road safety audits on new roads, but only 17 conduct such audits on all existing roads.
- Ten countries have policies to separate road users as a way of protecting vulnerable road users.
- Eleven countries have national policies that support investment in safe public transportation.
- Only one country, South Africa, complies with the UN Forum on the Harmonization of Vehicle Standards.
Eleven countries have comprehensive urban speed limits of <50 km/h. Nine countries have a blood alcohol level of <0.05 g/dl for drivers. Fourteen countries have a comprehensive motorcycle helmet law and a helmet standard.
Eighteen countries have a seatbelt law that applies to all occupants, but only 12 countries have a child restraint law. No countries have comprehensive laws on all five major risk/protective factors. Road traffic crashes and their consequences are estimated to cost African governments between 0.8% and 9% of their GDP.
In addition, most countries in the region suffer limited capacity in the following key areas with regard to managing road traffic crash survivors: communication, appropriate transportation, human resources, adequately equipped health facilities, and trauma service management. The following indicators point to these inadequacies:
- One in three countries has no national emergency access telephone number.
- Five countries have no ambulance services at all.
- In 23 countries with an ambulance service, experts estimate that less than 10% of seriously injured patients benefit from ambulance evacuation.
- While just over 50% of countries have emergency medicine training programmes for doctors, only one-third have formal postgraduate training for nurses.
Clearly, Africa has a long way to go if the goals of the Decade of Action as well as those set by the African Union to reduce deaths by 50% by 2020[4] are to be attained. In order to make substantial gains, the focus in Africa over this decade should be on making the roads safer for vulnerable users by separating traffic and providing safe public transportation; enacting and enforcing laws that protect all road users; and improving the post-crash response for all persons who survive a road traffic crash from the pre-hospital phase through to rehabilitation and reintegration back into society.
We encourage readers of the SAMJ to download their own copy of the Global Status Report on Road Safety 2013 and the accompanying fact sheet for the Africa region[5] from http://who.int/violence_injury_prevention/road_safety_status/2013, and to use these data to advocate for action in their own countries.
1. World Health Organization. Global Status Report on Road Safety 2013: Supporting a Decade of Action. Geneva: WHO, 2013. http://who.int/violence_injury_prevention/road_safety_status/2013 (accessed 6 March 2013). [ Links ]
2. Improving Global Road Safety (UN General Assembly resolution A/RES/64/255). New York: United Nations, 10 May 2010. http://www.who.int/entity/violence_injury_prevention/publications/road_traffic/UN_GA_resolution-54-255-en.pdf (accessed 6 March 2013). [ Links ]
3. World Health Organization. Global Status Report on Road Safety: Time for Action. Geneva: WHO, 2009. http://www.who.int/violence_injury_prevention/road_safety_status/2009/en/index.html (accessed 6 March 2013). [ Links ]
4. Declaration of the African Ministers Responsible for Transport and Infrastructure on Transport and the Millennium Development Goals (MDGs). Addis Ababa, Ethiopia, African Union, 6 April 2005. http://www.un.org/special-rep/ohrlls/lldc/2089509607declaration_of_african_transport_ministers.pdf (accessed 6 March 2013). [ Links ]
5. World Health Organization. Road Safety in the WHO African Region: The Facts 2013. Brazzaville, Democratic Republic of Congo: WHO, 2013. http://who.int/violence_injury_prevention/road_safety_status/2013 (accessed 6 March 2013). [ Links ]
Funding. The Global Status Report on Road Safety 2013 was made possible through funding from Bloomberg Philanthropies.
Disclaimer. Drs Peden and Monono are staff members of the World Health Organization, they alone are responsible for the views expressed in this publication, and they do not necessarily represent the decisions or policies of the WHO. Dr Kobusingye is a Research Fellow at Makerere University, School of Public Health, Kampala, Uganda, and at the University of South Africa.
Competing interests. None declared.
 Corresponding author: M Peden (pedenm@who. int)
Corresponding author: M Peden (pedenm@who. int)
