










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Science
On-line version ISSN 1996-7489Print version ISSN 0038-2353
S. Afr. j. sci. vol.121 n.5-6 Pretoria May./Jun. 2025
https://doi.org/10.17159/sajs.2025/16682
RESEARCH ARTICLE
Deterioration of sleep and mental health in individuals with insomnia during South Africa's COVID-19 lockdown
Alison BentleyI; Laura C. RodenII, III, IV; Jonathan P. DavyV; Stella lacovidesVI; F. Xavier Gómez-OlivéVII; Karine ScheuermaierVI; Raphaella LewisVIII; Gosia LipinskaVIII; Johanna RocheVI; Candice J. ChristieV; Swantje WellsV; Dale E. RaeIII, IV
IDepartment of Family Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IICentre for Health and Life Sciences, School of Life Sciences, Faculty of Health and Life Sciences, Coventry University, Coventry, UK
IIIHealth through Physical Activity, Lifestyle and Sport Research Centre, Department of Human Biology, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa
IVDivision of Physiological Sciences, Department of Human Biology, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa
VDepartment of Human Kinetics and Ergonomics, Rhodes University, Makhanda, South Africa
VIBrain Function Research Group, School of Physiology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIIMRC/Wits Rural Public Health and Health Transitions Research Unit (Agincourt), School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIIISleep Sciences and Applied Cognitive Science and Experimental Neuropsychology Team (AcSENT), Department of Psychology, University of Cape Town, Cape Town, South Africa
ABSTRACT
Sleep and mental health difficulties have been observed in response to COVID-19 pandemic-induced lockdowns, but few studies have described the impact of lockdown on individuals with self-reported insomnia. The purpose of this study was to compare the impact of lockdown on changes in symptoms of insomnia, depression and anxiety between persons with and without self-identified insomnia. In total, 1048 adult participants from the general South African population took part in this retrospective observational study during Alert Levels 4 and 3 in May and June 2020. They completed an online survey assessing current and past self-reported sleep disorders. Symptom profiles of insomnia (Insomnia Severity Index), depression (Patient Health Questionnaire-2) and anxiety (Generalised Anxiety Disorder 7-item scale) were assessed immediately before and during a 5-week lockdown (March-April 2020). Comparative analyses were conducted between participants who identified a current or previous diagnosis of insomnia (n = 135, Insomnia group, irrespective of whether they had current symptoms or not) and those reporting no sleep disorders (n = 700, No-Insomnia group). Participants who reported multiple sleep disorders were excluded from the analyses (n = 213). Symptoms of insomnia (p < 0.001), depression (p = 0.001) and anxiety (p = 0.001) worsened in all participants during lockdown compared to pre-lockdown measures. Time-by-group interaction effects were observed for all measures (p < 0.001) such that the Insomnia group reported larger increases in insomnia (p < 0.001), depression (p < 0.001) and anxiety (p < 0.001) scores compared to the No-Insomnia group during lockdown. Participants with self-reported insomnia, even if currently asymptomatic, were more vulnerable to worsening insomnia and depressive and anxiety-related symptoms during lockdown compared to those with no insomnia. This highlights vulnerability to mental-health-altering situations in individuals with self-identified insomnia, and thus the necessity to provide mental health support for this patient population.
SIGNIFICANCE:
Individuals who self-identified as insomniacs, even if they had minimal clinical symptoms of insomnia before the COVID-19-associated lockdown, experienced worsening of sleep initiation and maintenance, as well as symptoms of depression and anxiety during lockdown. These findings suggest that these individuals either identify with an insomnia identity or are vulnerable to sleep and mental health difficulties in stressful contexts.
Keywords: insomnia diagnosis, depressive symptoms, anxiety symptoms, vulnerability, lockdown
Introduction
The COVID-19 pandemic led to many changes in countries across the globe, including the introduction of 'lockdowns' aimed at limiting the spread of viral infection. South Africa's first hard lockdown (Alert Level 5) lasted 5 weeks (27 March-30 April 2020). Except for essential workers, people were allowed to leave home only for medical treatment or essential services during this period. Work activities were modified to occur at home, and exercise was limited to the home environment. Alert Level 4 lasted the month of May 2020 and was characterised by a restricted exercise period between 6:00 and 9:00. Individuals could walk, jog or cycle individually during this time, but national parks, where people typically exercise, remained closed during this time. Alert Level 3 was implemented in June 2020 and represented an easing of these restrictions. The lockdown periods provided a unique opportunity to examine the impact of changes in enforced routine-oriented behaviours on sleep disorders and sleep parameters on a background of limited data describing the frequency of sleep disorders in the South African population.
Several studies in South Africa and worldwide1-3 showed lockdown-induced increases in sleep duration, a delay in sleep timing and increases in symptoms of insomnia, depression and anxiety4. The general increases in anxiety and depressive symptoms that occurred during lockdown, described in many countries across the globe5-7 including South Africa4,8, are presumed to be contributing factors to pandemic-related sleep difficulties. Stress is a well-described trigger for acute insomnia.9 People who have previously experienced stress-induced insomnia may have an increase in sleep reactivity, described as a vulnerability to future insomnia with other stressful events.10 The additional stress induced by lockdown measures may therefore worsen the sleep of patients with insomnia, even if not currently symptomatic, more than those with no insomnia.
Other reasons for worsened insomnia could include changes in sleep patterns induced by lockdowns. Extensions and delays in bedtime and wake-up time, as reported in individuals with the disorder previously4, may worsen sleep efficiency with longer times spent awake in bed2. Sleep extension is a key perpetuating factor for chronic insomnia11, and sleep restriction is a key component of cognitive behavioural therapy for the treatment of insomnia12. Thus, multiple factors may induce worsened sleep during lockdown in people with pre-existing insomnia compared to those without insomnia. Very few studies have investigated how these sleep and psychological changes in response to lockdown impacted people who had insomnia before lockdown.
Thus, our first aim was to report on the frequency of sleep disorders in South African adults who responded to a nationwide survey of lifestyle changes in response to the COVID-19 lockdown. Our second aim was to compare lockdown-induced changes in sleep and symptoms of insomnia, depression and anxiety between persons who identified as having insomnia and those who did not. We hypothesised that participants with self-reported insomnia would be impacted more severely by the pandemic-induced lockdown than those without insomnia.
Materials and methods
Study design and setting
We present a sub-analysis of data collected as part of a larger observational study4 designed to assess routine-oriented lifestyle behaviours (work, sleep, physical activity, screen time, meal timing, caffeine and alcohol consumption) as well as symptoms of depression, anxiety and insomnia in South African adults before and during the 5-week COVID-19 pandemic national Alert Level 5 lockdown.
The online survey was distributed during Alert Levels 4 and 3 between 12 May and 15 June 2020 through formal academic mailing lists and professional and personal social media networks of the research staff, with participants being further encouraged to pass on the survey through their own networks. The full sampling strategy of this study has been described previously.4 Most (90%) of the participants were enrolled between 15 and 31 May 2020 during Alert Level 4. Respondents were required to answer questions for two time points: before lockdown (defined as the 3 months before lockdown, i.e. January, February and March 2020) and during lockdown (defined as the 5 weeks of Level 5 lockdown, i.e. 27 March to 30 April 2020).
Participants
Persons older than 18 years of age with a primary place of residence in South Africa before and during the period of COVID-19 lockdown were eligible to participate in the parent study.4 All participants (n = 1048) gave informed consent before completing the survey. Ethical clearance was obtained from the Rhodes University Human Ethics Committee (review reference 2020-1459-3468) and the Department of Psychology Ethics Committee at the University of Cape Town (PSY2020-014). Given the paucity of data on sleep disorders among South Africans, data from all participants in the parent study were used to report on the prevalence of sleep disorders (Aim 1). For Aim 2, we compared those participants who self-identified as suffering from insomnia but did not report suffering from any other sleep disorder (Insomnia group, n = 135) to those who did not report suffering from any sleep disorder (No-Insomnia group, n = 700). For this set of analyses, we excluded all participants with other or multiple sleep disorders (n = 213).
Survey
Full details of the survey (including demographic, medical history, work, sleep and physical activity questions) have been published previously.4 Customised questions about sleep disorders were asked: 'Do you suffer from, or have you been diagnosed with any of the following sleep-related disorders or conditions? Select all that apply'. Possible sleep disorders were listed as insomnia, obstructive sleep apnoea, central sleep apnoea, snoring, narcolepsy, restless legs syndrome, periodic limb movement disorder, sleep-related rhythmic movement disorder, bruxism, circadian rhythm disorders, parasomnias and others. Participants who indicated that they either currently suffer from insomnia or have been diagnosed with it in the past, formed the Insomnia group. Similarly, we asked, 'Do you suffer from or have you been diagnosed with any of the following chronic conditions (current or past)? Select all that apply'. Amongst disorders listed (such as asthma, heart disease and cancer), participants could select depression and anxiety. Participants, thus, could indicate that they currently experienced, or were previously diagnosed with, depression and/or anxiety. In addition, participants were asked to detail their usual bedtimes, wake-up times, total sleep times and use of sleep medications.
Symptoms of insomnia, depression and anxiety were assessed using the Insomnia Severity Index (ISI)13, the Patient Health Questionnaire-2 (PHQ-2)14 and the Generalised Anxiety Disorder 7-item (GAD-7) scale15, respectively. The ISI was used to measure symptoms. It consists of seven items that assess the perceived severity of difficulties initiating sleep, staying asleep and early morning awakenings; satisfaction with the current sleep pattern; interference with daily functioning; noticeability of impairment attributed to the sleep problem; and degree of distress or concern caused by the sleep problem. Scores range from 0 to 28, with higher scores indicating a higher degree of insomnia severity. Scores of 0-7 indicate 'No clinically significant insomnia', 8-14 'Subthreshold insomnia', 15-21 'Clinical insomnia (moderate severity)' and 22-28 'Clinical insomnia (severe)'.16
The PHQ-2 was used to assess the frequency of depressed mood and anhedonia. Scores range from 0 to 6, with higher scores indicating greater levels of depression and scores of 4 or more indicating the likelihood of a depressive disorder.14 The GAD-7 scale was included to screen for generalised anxiety disorder. Scores range from 0 to 21, with higher scores indicating greater levels of anxiety.15
Data and statistical analyses
Data are presented as the mean with standard deviation (SD), median with interquartile range (IQR) or frequency (percentage). The Shapiro-Wilk test was used to assess normality. We created an ISI clinical category (>15 points) by combining ISI severity categories of moderate (15-21 points) and severe clinical insomnia (22-28 points) due to small numbers in the severe category. The total ISI scores, individual items within the ISI, GAD-7 scores and PHQ-2 scores were treated as non-parametric data and analysed accordingly. Between-group comparisons were made using an independent f-test, Mann-Whitney U test, Chi-squared test or Fisher's exact test. Post-hoc comparisons of categorical data were done using Fisher's exact test, correcting for multiple comparisons. Comparisons between the before and during lockdown time points were made using mixed-effects linear regression models, Wilcoxon signed-rank test, McNemar's test or Bowker's test of symmetry. In addition to our primary analyses, we explored worsened and improved insomnia symptoms in the Insomnia and No-Insomnia groups to examine how lockdown changed the profile of symptoms within each group. We conducted this analysis using Fisher's exact test. Data were analysed using Stata v15.1 (StataCorp, Texas, USA) and GraphPad Prism v5.02 (Graphpad.com). Statistical significance was accepted at p < 0.05.
Results
Frequency of self-reported sleep disorders In all participants
Of the 1048 participants, 348 (33.2%) indicated that they suffered from a sleep disorder. Figure 1 displays the percentage of the various self-reported sleep disorders in this study. Insomnia was the most common sleep disorder reported (n = 197; 18.8% of the 1048 participants), with 135 participants (12.9% of the 1048) reporting insomnia as the only sleep disorder.
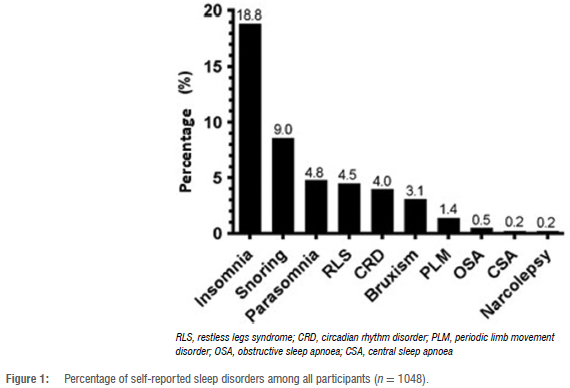
Nearly three-quarters of people with a sleep disorder reported having only one sleep disorder (n = 246, 70.7%), a fifth reported having two sleep disorders (n = 70, 20.1%) and 7.2% (n = 25), 1.4% (n = 5), 0.3% (n = 1) and 0.3% (n = 1) reported three, four, five or six sleep disorders,
respectively. The most commonly co-occurring sleep disorders were insomnia and snoring (n = 23, 2.2%), insomnia and parasomnia (n = 19, 1.8%), insomnia and restless legs syndrome (n = 17, 1.6%), insomnia and a circadian-related disorder (n = 17, 1.6%), snoring and restless legs syndrome (n = 12, 1.1%), a circadian-related sleep disorder and parasomnia (n = 12, 1.1%) and insomnia and bruxism (n = 11, 1.0%). Only 3% (n = 31) of participants used medication to sleep, including amitriptyline, clobazam, zolpidem, zopiclone, quetiapine and melatonin.
Changes in self-reported insomnia symptoms in all participants
The ISI scores among the whole sample worsened during lockdown compared to before lockdown. The total ISI score increased from a median of 4 (IQR: 2-8) before lockdown to 10 (4-15) during lockdown (p < 0.001). The distribution of the proportions of the population in each of the three ISI severity categories was different before lockdown compared to during lockdown (Figure 2, p < 0.001). Post-hoc analyses showed that there were significantly more participants in the subthreshold (p < 0.001) and clinical insomnia (p < 0.001) categories during lockdown compared to before lockdown. Correspondingly, fewer people were categorised as having no clinically significant insomnia during lockdown than before lockdown (p < 0.001).
Comparisons between the Insomnia and No-Insomnia groups
The general characteristics of these two groups before lockdown are presented in Table 1. Compared to the No-Insomnia group, participants in the Insomnia group were significantly more likely to be women (p = 0.023), to report chronic medical conditions (p < 0.001) and have higher insomnia (p < 0.001), depressive (p = 0.002) and anxiety (p < 0.001) scores. The Insomnia group also included more individuals who self-reported a history of depression (p < 0.001) and anxiety (p < 0.001), and a greater proportion of participants in the Insomnia group (n = 19/135, 14.1%) were taking medication to sleep compared to those in the No-Insomnia group (n = 14/700, 2.0%, p < 0.001). The mean total sleep time of those participants in the Insomnia group on sleep-promoting medication (n = 19, 7.0 ± 1.3 h) was not different from those who were taking other medications (n = 31; 7.0 ± 0.8 h) or those who did not supply any information on medication use (n = 85; 7.1 ± 1.1 h, p = 0.965).
Finally, there were no differences between the Insomnia and No-Insomnia groups for self-reported alcohol or caffeine consumption and exercise levels.
The sleep characteristics of both groups before and during lockdown are shown in Table 2. There was a main effect of time for all variables, indicating that the participants went to bed later, woke up later, spent more time in bed and increased total sleep time during lockdown compared to before lockdown. There was no group main effect for any of the variables, but there was a time-by-group interaction effect for wake-up time (p = 0.038) and total sleep time (p = 0.042). Specifically, the delay in wake-up time during lockdown was greater in the Insomnia group (±2.1 h) compared to the No-Insomnia group (±1.75 h), and only the No-Insomnia group had significantly increased total sleep time (±22 min) during lockdown compared to before lockdown (both p < 0.050).
Figure 3 shows changes in symptoms of insomnia (ISI, 3A), anxiety (GAD-7, 3B) and depression (PHQ-2, 3C) in response to the lockdown for the Insomnia and No-Insomnia groups. ISI (p < 0.001) categories, GAD-7 (p = 0.001) and PHQ-2 (p = 0.001) scores increased significantly for all participants during lockdown compared to before lockdown. A time-by-group interaction effect was observed for ISI, GAD-7 and PHQ-2 (all p < 0.001). Specifically, post-hoc analyses indicate that the Insomnia group reported greater increases in ISI (p < 0.001), GAD-7 (p < 0.001) and PHQ-2 (p < 0.001) scores compared to the No-Insomnia group during lockdown.
The self-reported ISI severity categories of the two groups before and during lockdown are presented in Table 3. In all cases, there were significant changes when comparing during lockdown with before lockdown (all p < 0.001), except for the participants with subthreshold insomnia in the Insomnia group (p = 0.201).
Figure 4 compares the percentage of participants in the Insomnia and No-Insomnia groups whose ISI symptoms worsened, improved or remained unchanged during lockdown. "Got worse' was defined as moving from a lower to higher ISI category (e.g. moving from the subthreshold group to the clinical group), while 'Got better' was defined as moving from a higher to a lower category. Within the ISI-defined 'No clinical insomnia' category before lockdown, more people in the Insomnia group reported worsening of insomnia symptoms during lockdown compared to the No-Insomnia group (80% vs 44.6%; p < 0.001). More participants in the No-Insomnia group (53.4%) remained unchanged compared to the Insomnia group (20.0%; p < 0.001). Likewise, in the ISI-defined 'Subthreshold insomnia' category before lockdown, more people in the Insomnia group (57.7%) reported worsening of insomnia symptoms during lockdown compared to the No-Insomnia group (26.5%; p < 0.05) and more of those in the No-Insomnia group reported improvement (29.9%) compared to the Insomnia group (33.8%; p < 0.05, post-hoc tests on Chi-squared; overall p < 0.001). Of the participants who were classified as having ISI-defined 'Clinical insomnia' before lockdown, no differences were observed in the number of participants who 'got worse', were 'unchanged' or who 'got better' between the Insomnia and No-Insomnia groups (p = 0.474).
Discussion
In this online survey of sleep and lifestyle behaviours before and during the stringent Alert Level 5 lockdown (25 March to 1 May 2020) in South Africa, a third of participants reported having a sleep disorder, most commonly insomnia, with an overall worsening of insomnia symptoms in the whole population during lockdown when compared to before lockdown. Participants with self-reported insomnia before lockdown were more likely to have worse insomnia during lockdown compared to those with no self-reported sleep disorder. This was particularly true for those who, despite self-identifying as having insomnia, endorsed no or subthreshold insomnia symptoms on a standardised insomnia questionnaire, indicating an increased vulnerability to the circumstances of lockdown in these participants.
The number of people presenting with sleep disorders in our participants (33%) was similar to that found in other studies of South Africans, although in older age groups.17,18 The observations of self-reported obstructive sleep apnoea and restless legs syndrome were lower than expected in our study, but we speculate that this may be due to the younger age of respondents and the likely limited awareness of sleep disorders in the South African population. Two studies using South African data have estimated the prevalence of moderate-to-severe obstructive sleep apnoea in middle-aged and older South Africans to be over 25%.19,20 The occurrence of insomnia (18.8%) was lower than that found in a previous study across many countries including South Africa (45%)17 and higher than a study on South African students (7.5%)21. More population studies are required for more accurate prevalence data of all sleep disorders in South Africa.
We observed discrepancies in insomnia symptoms when comparing the No-Insomnia and Insomnia groups. There was an unexpectedly higher proportion of participants with self-reported insomnia who did not have an ISI score greater than 14. It may be that South Africans in this cohort misunderstood the meaning and criteria for a diagnosis of insomnia, or that participants who had previously had insomnia but did not currently suffer from it also answered in the affirmative. One possibility is that these participants have an insomnia identity22 or, simply, that they just remembered having had insomnia at some point in their lives. Despite this inconsistency, the Insomnia group overall had higher mean ISI scores compared to the No-Insomnia group. A high proportion of asymptomatic patients with previous insomnia in the Insomnia group may explain why there was no difference in most of the sleep measures between the Insomnia and No-Insomnia groups before lockdown.
There was an increase in the severity of insomnia symptoms and severity categories in the whole population during lockdown compared to before lockdown, consistent with other studies.23 Most of these previous studies, however, did not differentiate between patients with sleep disorders and those without.23 Our data show that in a group of individuals where other sleep disorders have been specifically excluded, there is a worsening of insomnia, depression and anxiety scores during lockdown when compared to pre-lockdown scores. The association between poor sleep health and an increase in anxiety and depression during the pandemic has been shown across multiple countries and studies.24,25 Lockdown and the pandemic itself would have exacerbated anxiety for various reasons, including fear of contracting the virus, separation from loved ones, worries about the economy, potential job losses and financial hardship.
Participants in the Insomnia group were significantly more likely to be women and have chronic conditions, especially depression and anxiety, similar to patients with insomnia worldwide. This finding confirms the strong and consistent association between sleep problems and self-reported anxiety and depression.25 When compared to the No-Insomnia group during lockdown, the Insomnia group had more severe changes in insomnia, depression and anxiety symptoms, indicating an increased vulnerability to a stressful situation. We had anticipated such findings as both anxiety and depression have bidirectional relationships with poor sleep.25 The association found does not, however, imply a causative mechanism. It is unclear whether this vulnerability will lead to chronic insomnia, anxiety and depression post-lockdown, as shown in some studies26, or whether this worsening is acute and self-limiting, as in intermittent acute insomnia27. Our data show that individuals who self-reported current or previous insomnia, but who had no or subthreshold insomnia symptoms before lockdown, were disproportionately likely to experience worsening symptoms during lockdown, in comparison to those who did not self-identify as having insomnia. Two possible explanations may account for these findings. Firstly, individuals may have an insomnia identity with which they align, even if they are not currently experiencing insomnia symptoms.22 Additionally, or alternatively, based on their previous insomnia experience, they may be vulnerable to insomnia when stressful experiences present themselves (that is, they may show sleep reactivity10). Both of these mechanisms independently predict an increased likelihood of worsening of sleep under stressful conditions in people who have had previous episodes of insomnia.
Limitations
Respondents of this survey were mainly young adults (mean age: 27 years) with access to the Internet, and thus the data cannot be extrapolated to an older population or the general population in South Africa. The population was limited to the social media networks of the researchers and their professional societies and the student populations, which, while unavoidable due to lockdown, limited the reach of the survey. We acknowledge that there may have been a recall bias in our participants when asked to evaluate their symptoms before lockdown. The study also relied on self-reported data for insomnia, depression and anxiety diagnoses, which may be clinically inaccurate.
Conclusion
In these participants, South Africans experienced worsening of insomnia, depression and anxiety during lockdown. These effects were more pronounced in individuals who self-identified as suffering from insomnia, either currently or previously. Furthermore, participants with self-identified insomnia, but who reported either no or subthreshold insomnia symptoms before lockdown, were more likely to experience worsened insomnia during lockdown in comparison with those who did not identify with current or previous insomnia. These findings highlight a higher vulnerability to mental-health-altering situations in individuals with self-identified insomnia, and thus the necessity to provide mental health support for this patient population.
Finally, there is also a need for better prevalence data and more insight into the understanding of sleep disorders in the South African population.
Acknowledgements
J.R. was supported by a postdoctoral research fellowship from the University of the Witwatersrand's University Research Council.
Data availability
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the data, they cannot be made available.
Author contributions
A.B.: Conceptualisation, data collection, writing - the initial draft, writing -revisions. L.R.: Conceptualisation, data collection, writing - revisions. J.D.: Conceptualisation, data collection, writing - revisions. S.I.: Conceptualisation, data collection, writing - revisions. RX.G-O.: Conceptualisation, data collection, writing - revisions. K.S.: Conceptualisation, data collection, writing -revisions. R.L.: Conceptualisation, data collection, writing - revisions. G.L.: Conceptualisation, data collection, writing - revisions. J.R.: Conceptualisation, data collection, writing - revisions. C.C.: Conceptualisation, data collection, writing - revisions. S.W.: Conceptualisation, data collection, writing -revisions. D.R.: Conceptualisation, data collection, writing - revisions, statistical analysis, figure compilation.
Declarations
We have no competing interests to declare. We have no AI or LLM use to declare. All authors read and approved the final manuscript.
References
1. Bertrand L, Schroder C, Bourgin P, Maruani J, Atoui d'Ortho MP et al. Sleep and circadian rhythm characteristics in individuals from the general population during the French COVID-19 full lockdown. J Sleep Res. 2022;31(2), Art. #13480. https://doi.org/10.1111/jsr.13480 [ Links ]
2. Cellini N, Conte F, De Rosa O, Giganti F, Malloggi S, Reyt M, et al. Changes in sleep timing and subjective sleep quality during the COVID-19 lockdown in Italy and Belgium: Age, gender and working status as modulating factors. Sleep Med. 2021;77:112-119. https://doi.org/10.1016/j.sleep.2020.11.027 [ Links ]
3. Romdhani M, Rae DE, Nedelec M, Ammar A, Chtourou H, Al Horani R, et al. COVID-19 lockdowns: A worldwide survey of circadian rhythms and sleep quality in 3911 athletes from 49 countries, with data-driven recommendations. Sports Med. 2022;52(6):1433-1448. https://doi.org/10.1007/s40279-021-01601-y [ Links ]
4. Davy JP, Scheuermaier K, Roden LC, Christie CJ, Bentley A, Gomez-Olive FX, et al. The COVID-19 lockdown and changes in routine-oriented lifestyle behaviors and symptoms of depression, anxiety, and insomnia in South Africa. J Rhys Act Health. 2021;18(9):1046-1057. https://doi.org/10.1123/jpah.2020-0863 [ Links ]
5. Huang Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Rsychiatry Res. 2020;288, Art. #112954. https://doi.org/10.1016/j.psychres.2020.112954 [ Links ]
6. Rossi R, Socci V Talevi D, Mensi S, Niolu C, Racitti F, et al. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front Rsychiatry. 2020;11, Art. #790. https://doi.org/10.3389/fpsyt.2020.00790 [ Links ]
7. Van Mulukom V, Muzzulini B, Rutjens BT, van Lissa CJ, Farias M. The psychological impact of threat and lockdowns during the COVID-19 pandemic: Exacerbating factors and mitigating actions. Transl Behav Med. 2021;11(7):1318-1329. https://doi.org/10.1093/tbm/ibab072 [ Links ]
8. Varma R Junge M, Meaklim H, Jackson ML. Younger people are more vulnerable to stress, anxiety and depression during cOvID-19 pandemic: A global cross-sectional survey. Rrog Neuro-Rsychopharmacol Biol Rsychiatry. 2021;109, Art. #110236. https://doi.org/10.1016/j.pnpbp.2020.110236 [ Links ]
9. Spielman AJ, Caruso LS, Glovinsky RB. A behavioral perspective on insomnia treatment. Rsychiatr Clin North Am. 1987;10(4):541-553. https://doi.org/10.1016/S0193-953X(18)30532-X [ Links ]
10. Kalmbach DA, Cuamatzi-Castelan AS, Tonnu CV, Tran KM, Anderson JR, Roth T, et al. Hyperarousal and sleep reactivity in insomnia: Current insights. Nat Sci Sleep. 2018;10:193-201. https://doi.org/10.2147/NSS.S138823 [ Links ]
11. Levenson JC, Kay DB, Buysse DJ. The pathophysiology of insomnia. Chest. 2015;147(4):1179-1192. https://doi.org/10.1378/chest.14-1617 [ Links ]
12. Riemann D, Baglioni C, Bassetti C, Bjorvatn B, Dolenc Groselj L, Ellis JG, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):675-700. https://doi.org/10.1111/jsr.12594 [ Links ]
13. Bastien CH, Vallieres A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297-307. https://doi.org/10.1016/S1389-9457(00)00065-4 [ Links ]
14. Kroenke K, Spitzer RL, Williams JB. The patient health questionnaire-2: Validity of a two-item depression screener. Med Care. 2003;41(11):1284-1292. https://doi.org/10.1097/01.MLR.0000093487.78664.3C [ Links ]
15. Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med. 2006; 166(10):1092-1097. https://doi.org/10.1001/archinte.166.10.1092 [ Links ]
16. Morin CM, Belleville G, Belanger L, Ivers H. The Insomnia Severity Index: Rsychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34(5):601-608. https://doi.org/10.1093/sleep/34.5.601 [ Links ]
17. Soldatos CR, Allaert FA, Ohta T Dikeos DG. How do individuals sleep around the world? Results from a single-day survey in ten countries. Sleep Med. 2005;6(1):5-13. https://doi.org/10.1016/j.sleep.2004.10.006 [ Links ]
18. Stranges S, Tigbe W, Gomez-Olive FX, Thorogood M, Kandala NB. Sleep problems: An emerging global epidemic? Findings from the INDERTH WHO-SAGE study among more than 40,000 older adults from 8 countries across Africa and Asia. Sleep. 2012;35(8):1173-1181. https://doi.org/10.5665/sleep.2012 [ Links ]
19. Benjafield AV, Ayas NT, Eastwood PR, Heinzer R, Ip MSM, Morrell MJ, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir Med. 2019;7(8):687-698. https://doi.org/10.1016/S2213-2600(19)30198-5 [ Links ]
20. Roche J, Rae DE, Redman KN, Knutson KL, von Schantz M, Gomez-Olive FX, et al. Impact of obstructive sleep apnea on cardiometabolic health in a random participants of older adults in rural South Africa: Building the case for the treatment of sleep disorders in underresourced settings. J Clin Sleep Med. 2021;17(7):1423-1434. https://doi.org/10.5664/jcsm.9214 [ Links ]
21. Peltzer K, Pengpid S. Nocturnal sleep problems among university students from 26 countries. Sleep Breath. 2015;19(2):499-508. https://doi.org/10.1007/s11325-014-1036-3 [ Links ]
22. Lichstein KL. Insomnia identity. Behav Res Ther. 2017;97:230-241. https://doi.org/10.1016/j.brat.2017.08.005 [ Links ]
23. Jahrami H, BaHammam AS, Bragazzi NL, Saif Z, Faris M, Vitiello MV. Sleep problems during the COVlD-19 pandemic by population: A systematic review and meta-analysis. J Clin Sleep Med. 2021;17(2):299-313. https://doi.org/10.5664/jcsm.8930 [ Links ]
24. Casagrande M, Favieri F, Tambelli R, Forte G. The enemy who sealed the world: Effects quarantine due to the COVlD-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020;75:12-20. https://doi.org/10.1016/j.sleep.2020.05.011 [ Links ]
25. Lewis R, Roden LC, Scheuermaier K, Gomez-Olive FX, Rae DE, Iacovides S, et al. The impact of sleep, physical activity and sedentary behaviour on symptoms of depression and anxiety before and during the COVID-19 pandemic in a participants of South African participants. Sci Rep. 2021;11(1), Art. #24059. https://doi.org/10.1038/s41598-021-02021-8 [ Links ]
26. Gorgoni M, Scarpelli S, Mangiaruga A, Alfonsi V, Bonsignore MR, Fanfulla F, et al. Persistence of the effects of the COVID-19 lockdown on sleep: A longitudinal study. Brain Sci. 2021;11(11), Art. #1520. https://doi.org/10.3390/brainsci11111520 [ Links ]
27. Ellis JG, Perlis ML, Bastien CH, Gardani M, Espie CA. The natural history of insomnia: Acute insomnia and first-onset depression. Sleep. 2014;37(1):97-106. https://doi.org/10.5665/sleep.3316 [ Links ]
 Correspondence:
Correspondence:
Gosia Lipinska
Email:gosia.lipinska@uct.ac.za
Received: 16 Aug. 2024
Revised: 29 Apr. 2025
Accepted: 29 Apr. 2025
Published: 29 May 2025
Editors: Pascal Bessong, Shane Redelinghuys
Funding:None

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}