










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work/Maatskaplike Werk
On-line version ISSN 2312-7198Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.55 n.2 Stellenbosch 2019
https://doi.org/10.15270/52-2-716
ARTICLES
Dual Diagnosis: How Adults Diagnosed with Bipolar Disorder Experience In-patient Substance Abuse Treatment for Stimulant Use Disorder
Karina van ZylI; Stephan GeyerII
IPostgraduate Student; Department of Social Work and Criminology, University of Pretoria, Pretoria, South Africa
IIDepartment of Social Work and Criminology, University of Pretoria, Pretoria, South Africa
ABSTRACT
Dual diagnosis has become a topic of interest in recent years. In South Africa individuals diagnosed with dual diagnosis are left without adequate services as a result of the separation of substance abuse and mental health treatment services. Through a phenomenological study the authors aimed to explore how adults diagnosed with both bipolar disorder and stimulant use disorder experienced treatment at treatment centres. Considered from a bio-psychosocial perspective, the findings give insight into service users' living world with a dual diagnosis, their experiences, their unique needs for treatment and requirements to maintain abstinence. Recommendations for social work services at treatment centres are offered.
Keywords: dual-diagnosis, bipolar disorder, stimulant use disorder, substance use disorder, adult, in-patient treatment
Introduction AND problem statement
The United Nations Office on Drugs and Crime (UNODC) (2017:9) estimated that in the year 2015 approximately 250 million adults were abusing illicit drugs globally. Illicit drugs are generally divided into four categories: opioids, stimulants, depressants and psychedelics (Nutt, 2012:38). The use of stimulant-type drugs is responsible for a significant portion of the global burden of disease ascribed to substance use, and the growing market for these types of drugs indicates higher rates of use (UNODC, 2017:9). Stimulant drugs are defined as drugs that "increase respiration, heart rate, motor activity, and alertness" (Fisher & Harrison, 2013:21). Stimulant use disorder is defined by the American Psychiatric Association (2013b) as "[a] pattern of amphetamine-type substances, cocaine, or other stimulant use leading to clinically significant impairment or distress" (APA, 2013a:561). Even though most African countries have insufficient methods of tracking and reporting the prevalence of substance use disorders (SUD), the UNODC West African Commission on Drugs (WACD) (2014:40) reports an increase in the manufacture and seizure of methamphetamines - a stimulant drug. SUD is defined as "a cluster of cognitive, behavioural, and physiological symptoms indicating that the individual continues using the substance despite significant substance-related problems" (APA, 2013a:483).
The Republic of South Africa (RSA) is a developing country consisting of nine provinces, home to a multicultural society, with the Gauteng province earning the highest per capita income in the country (RSA, 2018). Pretoria, located in the Gauteng province, is the administrative capital of the RSA and is the location of the research population reported on in this article (RSA, 2018). The South African Community Epidemiology Network on Drug Use (SACENDU) (2017:5) reported that between January and June of 2017 a total of 3 870 individuals were admitted to seventeen treatment centres in the Gauteng province, of whom 23% reported amphetamine-type stimulants as their primary or secondary drug of choice. The use of methcathinone (CAT), which is an amphetamine-based synthetic stimulant, is increasing in all provinces, but more so in the Gauteng province, where 9% of patients admitted to treatment reported CAT as their drug of choice (SACENDU, 2017:12). In addition, SACENDU (2017:12) reports that 39% of the 10 047 patients admitted to 80 treatment centres across South Africa during the first half of 2017 reported mental health problems upon admission.
The National Institute on Drug Abuse in the United States of America (USA) (NIDA 2010:10) defines dual diagnosis (DD) as "[t]he occurrence of two disorders or illnesses in the same person, either at the same time (co-occurring comorbid conditions) or with a time difference between the initial occurrence of one and the initial occurrence of the other". In the RSA mental disorders are diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders (DSM), compiled by the APA. The APA (2013b:4) explains that bipolar disorder (BD) was previously classified as a mood disorder, but became a separate category in the fifth edition of the DSM (DSM-5) as changes in energy levels and activity are as important as mood changes (APA, 2013a:810). Whenever the authors refer to BD in this article it is with reference to all types of BD as classified in the DSM-5 (APA, 2013a).
A study conducted by Fabricius, Langa and Wilson (2007:7) aimed at establishing the prevalence of DD among individuals in a treatment centre in Johannesburg. It was found that 57% of the 419 patients had a DD. Swann (2010:278) maintains that patients diagnosed with BD are more inclined to use stimulant drugs as they want to achieve the level of mania they experience during a manic episode of BD. The higher prevalence of DD, however, is not limited to the RSA. Tiet and Mausbach (2007:513) explain that in the USA 60% of individuals who seek treatment for drug abuse are diagnosed with mental disorders, such as BD, and 56% of individuals seeking treatment for BD have a co-occurring substance use disorder.
The presence of a DD complicates treatment in both disorders as individuals with a DD are less likely to comply with treatment and less likely to maintain abstinence in general, according to the National Alliance on Mental Illness (NAMI, 2013:1). Finding effective ways to treat these patients is made more difficult as there is a significant lack of information on the co-occurrence of BD and SUD, as well as the effects each has on the other (Swann, 2010:276). Information is limited as studies focusing on the treatment of BD usually exclude individuals with substance use disorders, thus little is known about the treatment of these patients (Weiss, Griffin, Jaffee, Bender, Graff, Gallop & Fitzmaurice, 2009:212). Fabricius et al. (2007:3) assert that it is no surprise that there is often no consensus concerning the treatment of DD, as there is no consensus on what causes it in the first place.
The first author became aware of the complexity of treating DD patients while working at a long-term substance abuse treatment centre in Pretoria. It was noted that those patients with a DD were more prone to relapse, but very little information was available on treating these individuals more effectively. The DD of BD and stimulant substance abuse was chosen as a starting point for a dedicated study, as it was identified as a common co-occurrence among the individuals admitted to treatment. Even though most researchers as well as SACENDU (2017:27) and the Department of Social Development (DSD, 2013a:3) acknowledge the high prevalence of DD in the RSA and calls for the development of treatment focused on this phenomenon, the authors were not able to identify research (EBSCOhost and Google Scholar) focused on intervention strategies. The authors agree with Matsea (2017) that the voice of service users should be heard to ensure that they are involved in the design of treatment programmes, as this has the potential to increase adherence to treatment, it generally improves the outcomes and prevents unnecessary expenditure. Therefore, the authors of this article aimed to explore how adult service users living with a DD of stimulant use disorder and BD experience treatment in in-patient treatment centres for SUD. The authors aimed to answer the following research question: "How do adults living with stimulant use disorder and bipolar disorder experience treatment at in-patient treatment centres for SUD in the Gauteng province?"
In order to contextualise DD all literature and research findings presented will be informed by a theoretical framework, viz. the bio-psychosocial perspective.
BIO-PSYCHOSOCIAL PERSPECTIVE
In 1977 George Engel introduced the bio-psychosocial (BPS) perspective to the medical field, urging medical professionals to consider the biological, psychological and social components influencing the lived experiences of individuals (Hatala, 2012:52). Routledge (2005:39) explains that the perspective focuses on three components of an individual: (1) bio, for biology, focuses on the genetic, biochemical and physical factors of a person; (2) psycho, for psychological, focuses on the developmental, psychological and psychopathological aspects of an individual; (3) social, focuses on family systems, diversity, culture, governments and social justice, which are all incorporated into the individual's interpersonal relationships. The isolation of culture as a fourth component has, however, been suggested in recent years, as culture saturates the other three components (Hatala, 2012:58); this is particularly so in countries such as the RSA where traditional healthcare forms part of many cultures and is often consulted before conventional (Western) health care (Jack, Wagner, Petersen, Thorn, Newton, Stein, Kahn, Tollman & Hofman, 2014:4).
In the RSA social workers are mainly responsible for the implementation of SUD treatment and usually focus on BPS components that 'cause' addiction and inform rehabilitation (Jack et al., 2014:4; Rassool, 2011:94). In addition, the BPS perspective was adopted as the theoretical framework guiding this study as both BD and stimulant use disorder have shared biological, psychological and social components that influence the cause, progression and treatment of both disorders. The BPS perspective allowed the exploration of the multivariate nature of DD as expressed by participants themselves, for example, the effects that a physical component such as lifestyle have on the psychological well-being of individuals while in treatment.
A brief overview of the causes, effects and treatment of both SUD and BD as separate disorders, as well as a DD, will be presented to shape the context of this study.
SUBSTANCE USE DISORDERS: CAUSES, EFFECTS AND TREATMENT
The causes of SUD are ascribed to various factors. The first is biological factors, such as genetics or neurochemicals, or a combination of them; the second, psychological factors such as turbulent home environments and undiagnosed mental health problems, and finally, social factors such as political turmoil, media and the school/work environment (Jack et al., 2014:3; Rassool, 2011:36).
Increased levels of substance abuse inhibit educational and occupational progress as these are detrimental to the physical, cognitive and psychological health of individuals, and place stress on interpersonal relationships (Fisher & Harrison, 2013:171). In 2005 the costs related to the treatment of methamphetamine in the USA, a developed country, were US$23 billion (±R1.92 billion), including costs related to crime, environmental damage, lost productivity, infectious diseases, family disruptions, cognitive dysfunction and premature death (Brensilver, Heinzerling & Shoptaw, 2013:45). In the RSA, a developing country, the social and economic costs associated with SUDs was estimated at R105 billion in 2013, placing an immense burden on healthcare and social welfare systems (DSD, 2013a:37). SUD is associated with worsened disease outcomes for various disorders, such as HIV and TB (DSD, 2013a:37).
Stimulants increase the activity of the central nervous system, which causes high levels of energy and mental functioning with a loss of appetite, followed by a phase of extreme fatigue, paranoia, anxiety and depression known as a "crash" (Rassool, 2011:83). The use of stimulant drugs is prevalent among individuals diagnosed with mental disorders and, in some cases, the diagnosis of BD can be overlooked as stimulants counter depressive mood cycles (Swann, 2010:278). Biological effects associated with stimulant drug abuse include nausea, insomnia, paranoia, anxiety, irregular heartbeat, excessive sweating, severe headaches, pressure on the chest, myocardial infarction, arrhythmias, cardiomyopathy, acute myocardial ischemia and sudden death (Nutt, 2012:118; Rassool, 2011:225).
The treatment of SUD varies significantly, but most effective treatment interventions include and take into account the following aspects (Rassool, 2011:278):
· Services should be available and accessible;
· Treatment should change according to the needs of an individual;
· The period spent in treatment should be adjusted and adequate for every individual;
· Both counselling and behavioural therapies should be included;
· Mental disorders and substance abuse should be diagnosed and treated concurrently;
· Involuntary treatment should not be deemed ineffective;
· Detoxification should not be seen as part of treatment, but rather as the first step in preparing for treatment;
· The diagnosis and treatment of infectious diseases should be part of treatment;
· Treatment should focus on the risk reduction of all spheres of functioning.
In the Framework for Social Welfare Services, the DSD (2013b:29) encourages social welfare practitioners to provide a continuum of services, informed by the individual needs of every service user and ultimately promoting the self-reliance and social functioning of these individuals.
The following section will focus on the causes, effects, and treatment of bipolar disorder.
BIPOLAR DISORDER: CAUSES, EFFECTS, AND TREATMENT
The DSM-5 (APA, 2013a:810) points out that the focus of BD falls on changes in mood as well as changes in energy and activity involvement, and is therefore not deemed a pure mood disorder. In terms of a BD, moods are clustered into two groups, manic and depressive symptoms. Manic symptoms include euphoria, increased energy, increased drive to achieve goals and an increase in irritability, the need for sleep decreases, distractibility and self-confidence are heightened, and there is an increased involvement in activities despite damaging consequences (APA, 2013a:124). Depressive symptoms include a decrease in energy levels, an increase in feelings of hopelessness and/or worthlessness, low self-confidence, weight loss, sleep difficulty, an inability to concentrate and psychomotor retardation (APA, 2013a:125). The DSM-5 distinguishes between several types of bipolar and bipolar-related disorders which are diagnosed based on the severity of the manic and depressive symptoms and the period of time these symptoms remain present or active (APA, 2013a:123).
The causes of BD are complex and can be ascribed to numerous factors such as genetics and neurochemicals, illicit drug use, the presence of other mental disorders and/or stressful life events (Miklowitz, 2010:41). The effects of BD are well documented and impact negatively on the physical, cognitive, emotional, financial, occupational and interrelational aspects of those affected (Archambeault, 2009:108). In recent years researchers have started to notice that ethnicity can play a role in the presentation of symptoms as well, after noticing higher levels of manic symptoms among black individuals in both the RSA and the United Kingdom (Grobler, 2012:164). In a study conducted by Lachman, Nessen, Hawkridge, and Emsley (2012) with 139 adolescents in a psychiatric hospital in the Western Cape Province, the use of methamphetamine was associated with high numbers of psychotic and mood disorders.
The DSM-5 indicates that SUD among individuals living with BD is high and that more research focused on this phenomenon is necessary (APA, 2013a:144). Weiss et al. (2009:212) reiterate the lack of research on DD, more so on BD coupled with SUD, as most researchers deliberately exclude individuals abusing drugs from BD treatment studies. Swann (2010:278) warns that the DD of stimulant use disorder and BD are as difficult to diagnose as it is to treat, as stimulants can hide depressive moods or mimic manic symptoms; thus either diagnosis can be overlooked.
Although the treatment of BD mostly focuses on pharmacotherapy, Archambeault (2009:107) encourages practitioners responsible for the treatment of BD to focus on all the bio-psychosocial aspects causing and maintaining any psychiatric diagnosis. Swann (2010:276) warns that SUD is the rule rather than the exception among individuals diagnosed with BD and is often detrimental to the effective treatment and recovery of individuals diagnosed with BD.
DUAL DIAGNOSIS: CAUSES, EFFECTS AND TREATMENT
The causes of DD are mainly attributed to four factors: (1) SUD allows individuals to feel that they are managing psychiatric symptoms; (2) SUD triggers the onset of psychiatric symptoms; (3) the same biological and social components predispose an individual to both; and (4) a high level of co-occurrence is merely coincidental (Fabricius et al., 2007:2; NIDA, 2010:3). When considering these explanations it is evident that identifying the causes of DD is complex, as it is the combination of the causes and effects of both disorders that leads to the development of the DD.
There are similar effects in both stimulant use disorder and BD. These effects seem to escalate when grouped together, as chaotic use patterns are more prominent (Rassool, 2011:36). Some of the effects associated with DD include the following: shorter periods of recovery; more visits to emergency units and hospitalisation; higher rates of suicidal thoughts and attempts; frequent displays of impulsivity and violence; higher occupational impairment and school drop-out rates; regular non-adherence to treatment; mixed mood states; higher levels of anxiety disorders; diminished quality of life; and poor treatment outcomes associated with HIV and TB (Lachman et al., 2012; Rassool, 2011:22).
Effective treatment outcomes greatly depend on early detection as, with time, symptoms become so intertwined that determining where one disorder ends and the other begins becomes impossible (Salloum, Pani & Cooke, 2010:354). Early detection is unfortunately not the norm, as individuals presenting with psychotic symptoms are generally not accepted into SUD treatment programmes in the RSA until symptoms have been treated (Lachman et al., 2012). Grobler (2012:6) acknowledges that as research on mental health care in the RSA is lacking, it is difficult to encourage people to seek treatment and provide accurate information. Even if individuals seek treatment, the primary health care system is already flooded and resources limited, thus making an accurate diagnosis and effective treatment very unlikely. The treatment gap is a major concern as most researchers agree that both disorders should be treated simultaneously and that the severity of both disorders should determine the time that treatment should continue (Fabricius et al., 2007:4; Rassool, 2011:218).
Pasche and Myers (2012:340) highlight that the historic separation of two sectors - the DSD heading substance abuse treatment and the Department of Health (DoH) providing mental health treatment - leaves both sectors poorly equipped to deal with DD effectively and concurrently. Despite the fact that the DSD (2013a:3) acknowledges the lack of available DD services in the RSA, available services remain inaccessible and unaffordable to the majority of the population (Lachman et al., 2012; Pasche & Myers, 2012:339).
Treatment specific to the RSA context is complex as most research focuses on the treatment or course of either SUD (Pasche & Myers, 2012:340) or BD (Grobler, 2012:6). Completed research that focused mostly on DD concentrated on determining its prevalence, rather than establishing specific treatment experiences of patients (Fabricius et al., 2007:14). Hence, the literature underscored the rationale for the study, namely to explore how adult service users living with a DD of stimulant use disorder and BD experience treatment within in-patient treatment centres for SUD.
An overview of the research methods will be offered, followed by a discussion on the findings of the study, presented as themes and sub-themes, as well as conclusions and recommendations highlighting the most important aspects of this phenomenon as it relates to treatment.
Research Methods
Rooted in phenomenology as research paradigm (Nieuwenhuis, 2016:60-62), a qualitative research approach enabled the authors to explore how people diagnosed with both bipolar disorder and stimulant use disorder experience treatment at in-patient treatment centres in the Gauteng province (Isaacs, 2014:318). The study had an exploratory purpose to gain as much understanding of the participants' personal experiences, especially as the study was the first of its kind in the RSA. The phenomenological research design, specifically the transcendental sub-design, was used as the authors aimed to describe authentically the lived experiences of adults living with a DD while in treatment without detailed interpretations by the authors (Creswell, 2013:80).
The research population was comprised of adults who had been admitted to three treatment centres in Pretoria (Gauteng province), who had been diagnosed with both BD and stimulant use disorder. All patients diagnosed with BD were included in the study, irrespective of the subtype of the bipolar diagnosis. Purposive sampling was used in a three-phase process to identify the research sample. In phase one purposive sampling was used to select three treatment centres in Pretoria where potential participants could be recruited. After permission was obtained from the treatment centres, inclusion criteria were provided to a social worker at each treatment centre, which aided in the identification of possible participants. Phase two of the sampling process, which was also purposive sampling, revolved around the identification of participants based on specific inclusion criteria, namely:
· Individuals who were older than 18 years;
· Individuals who had a stimulant drug addiction, which includes cocaine, CAT, khat or meth;
· Individuals who were not in the detoxification phase of treatment;
· Individuals living with the DD of stimulant use disorder and BD, which was confirmed by a medical practitioner or psychiatrist;
· Individuals could be either male or female;
· Individuals could be part of any religious and/or ethnic group;
· Individuals who could converse in Afrikaans or English.
In the third phase of the sampling process, all possible participants who met the inclusion criteria were approached by the social worker of the treatment centre and could volunteer to participate in the study. Even though the authors hoped to include a larger sample, four participants eventually participated. Nonetheless, Creswell (2013:78) states that sample sizes for phenomenological studies are often small (e.g. three participants).
The data-collection method used was a semi-structured one-on-one interview that was guided by an interview schedule. One interview, lasting up to 90 minutes, was conducted with each participant at his or her treatment site. The particular data-collection method was beneficial as it allowed enough freedom to explore the personal experiences of each participant (Isaacs, 2014:321).
All data collected were analysed through the process of thematic analysis (Clarke, Braun & Hayfield, 2015:223). Even though thematic analysis is not commonly associated with a phenomenological research design, Clarke and Braun (2013:120) explain that in recent years this form of analysis has received recognition along methodologies such as interpretative phenomenological analysis (IPA). Thematic analysis is also not confined to fixed theoretical frameworks and is seen as a basic method that is appropriate for any sample size (Clarke & Braun, 2013:120).
A number of strategies were adopted to ensure the trustworthiness of the study. Auditability was ensured by keeping field notes and a journal, consulting with a co-researcher and developing transcripts, which could be reviewed (Lietz & Zayas, 2010:195; Padgett, 2017:220). Credibility, how accurately data are presented, was maintained by discussing all themes and sub-themes with the co-author, as well as by performing member checking with one of the research participants (Lietz & Zayas, 2010:192; Padgett, 2017:219). Confirmability was achieved as most research findings could be confirmed by comparing research findings with literature (Lietz & Zayas, 2010:197). Transferability is possible when research findings could contribute to future research, theories, or practice. Transferability was ensured in this study by declaring all research processes, which could enable replication of the study (Lietz & Zayas, 2010:195).
Ensuring confidentiality, obtaining written informed consent from all participants and no harm were some of the ethical considerations that were adhered to during the study (Rubin & Babbie, 2017:85-90). The research study also received ethical clearance from the Research Ethics Committee of the university (Ref no.: GW20160523HS).
Findings
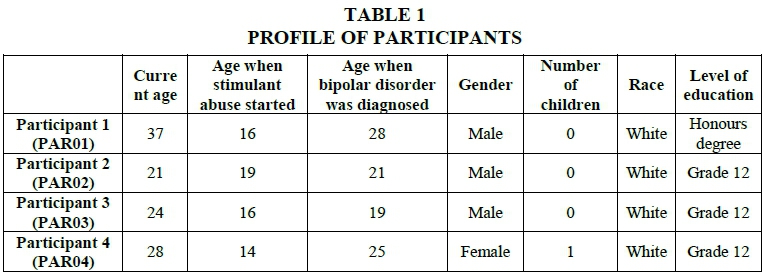
Table 1 contains the biographical details of the participants.
Merikangas and Peters (2010:55) state that BD affects men and women equally, but women over-represent the population in psychiatric treatment centres. In addition to this NIDA (2010:9), in the USA, reports that in terms of DD men seem to access rehabilitation programmes more frequently, while women are more inclined to access psychiatric treatment.
All the participants had previously been admitted to SUD treatment programmes, three participants also mentioned prior admission to psychiatric treatment centres, a finding that correlates with Lachman et al. (2012), who reported re-admission rates of 41% to psychiatric treatment programmes among South African youths. It is noteworthy that all participants started using stimulants before they were diagnosed with BD.
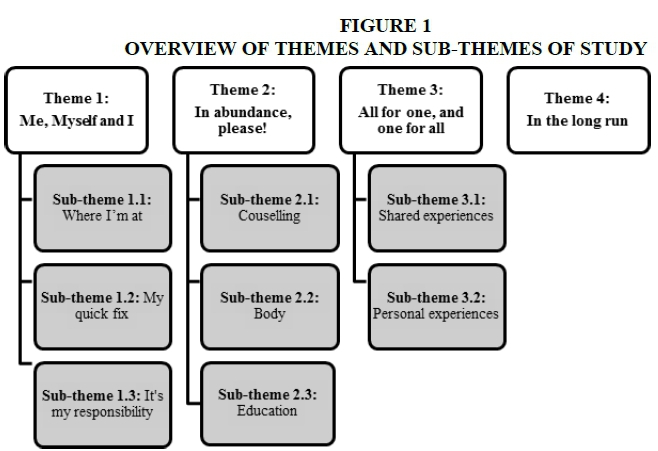
The study's findings will be presented in the format of themes and sub-themes (Figure 1).
Theme 1: Me, Myself and I
The consideration of all BPS aspects influencing the development, course, and progression of both disorders should be considered throughout the treatment process to promote recovery.
Sub-theme 1.1: Where I'm at
Prior to treatment, participants used stimulants as a means of managing rapid mood changes. As all participants received pharmacological treatment, it would be assumed that their moods were stable. However, regardless of pharmacological treatment focused on biological aspects, participants still experienced unstable mood patterns on a psychological level that triggered cravings for drugs on a physical level.
"… my mood … in the space of one day goes … up-and-down, up-and-down, up-and-down. You can't ask me how did I feel today. Because you'd have to ask me that like every hour." (PAR02)
"A lot of the times, I'm down and it makes me wish that I could get back to drugs to get like that quick fix to get happy and high again." (PAR03)
Participants explained how their mood would fluctuate multiple times during one day; however, it is during depressive cycles that they craved stimulants most, as they longed to experience manic symptoms. As participants did not have access to substances of abuse during treatment, they resorted to other means of managing moods, as discussed in the following section.
Sub-theme 1.2: My quick fix
Generally, individuals display behaviour or use products to alleviate emotional discomfort and manage moods. As seen in the previous section most participants reverted to stimulants to manage moods; however, while in the treatment they resorted to other 'quick fixes'.
"I need something to be happy, all the time. Whether it is drugs, or watching a movie, or, something needs to be there to make me happy." (PAR02)
"If I'm extremely, extremely depressed and I can't do anything… Go to the bathroom. Slit. Come out. Then I'm happy. Healed." (PAR02)
"Uhm psychologically this is tough hey. Like in the other rehabs, you can call your parents … you can get like tuck (tuck shop) every single day … you eat chocolate every day so you can like feed some kind of … a need or a lack or whatever, you can fill yourself with, with, with nonsense." (PAR01)
"I just wanted to go and lie down and just escape the world, you know." (PAR01)
Medication, food, sugar, contact with significant others, coffee, cigarettes, and self-mutilation are some of the 'fixes' that were mentioned by participants which offered psychological relief. As these products and behaviours can become habitual, referred to as cross-addictions, they carry their own set of risks, indicating that the root of the problem is still not being treated despite pharmacotherapy.
As a result of the continued mood instability, most participants considered discontinuation of treatment at some point. Reasons for remaining in treatment were mostly rooted in the sense of responsibility that the participants felt.
Sub-theme 1.3: It's my responsibility
Most participants believed that by remaining in treatment they took responsibility for various BPS factors.
"Uhm … I think that for my relationship with my parents a long-term programme is the only option I have. So, me not being here isn't actually an option."(PAR01)
"So inside I'm super sad, I'm destroying myself, I'm depressed, I'm thinking about suicide, but on the outside, I'm putting up this face and trying to work the programme, and trying to advance in the programme, you know."(PAR02)
Participants remained in treatment in an attempt to convince family members that they are committed, or because they are at an age or time in their life when they believe it is necessary to take responsibility for their actions. Other participants, however, remained in treatment to "get it over and done with" regardless of the psychological discomfort they experience during treatment. Interestingly, responsibility was expressed in terms of SUD, but not in terms of BD, a component that will be addressed in sub-theme 2.3.
The following theme will report on aspects of treatment which participants found beneficial.
Theme 2: In Abundance, Please!
In this theme, the need for physical and psychological aspects of treatment will be indicated.
Sub-theme 2.1: Counselling
The following statements indicate that counselling is one aspect of treatment that all participants esteemed:
"I need to speak about what's going on with me ... I don't know how to process the hurt." (PAR01)
"I live from one counselling session to the next." (PAR01)
"I struggle to uhm handle my own like emotions and things that I'm not in control of and they don't teach you how to control that in the beginning." (PAR03)
Two participants stated that they live from one counselling session to the next, as they need counselling to process what is going on in their mind. Counselling was seen as the most beneficial component in managing emotions and stress, and participants indicated that they would not recover without it. Most participants expressed a need for more counselling and most called for at least two sessions per week. One participant who received counselling twice a week, one session with a case manager and a second with a clinical psychologist, was satisfied, validating the need expressed by other participants.
Even though it appears as if counselling would be sufficient for recovery, participants valued a focus on physical aspects of treatment as well.
Sub-theme 2.2: Body
Concerning the physical components of treatment, participants said the following:
"... there is 'gymming' equipment … that's how I handle emotion. Because emotion handles me." (PAR02)
"... exercise is good especially when you are having a difficult time…" (PAR03)
Participants considered exercise as a valuable component of treatment in terms of managing mood and emotions. Other participants mentioned that healthy lifestyle factors, such as eating habits and sleep patterns, held great benefits and aided recovery. Education in terms of the role of a healthy lifestyle after treatment was, however, a need for one participant. The subsequent section will focus on other areas where education should take place as part of treatment.
Sub-theme 2.3: Education
Participants mentioned a need for education focused on a broad spectrum of topics:
"… knowledge of your addiction … and to learn to cope and a healthy lifestyle outside… what they do here is very good… there just needs to be more." (PAR02)
"The drug use and the bipolar… I know they might be similar but … I would like to differentiate between the two and get to know myself better as well." (PAR03)
Topics of interest included education on BD and addiction as diseases, developing coping skills, understanding how a healthy lifestyle promotes recovery and how BD and stimulant use influence each other. Most participants felt education should take place one-on-one with a professional as well as in groups consisting of individuals who share the same diagnosis.
It was thought-provoking to see that all participants saw education focused on both SUD and BD as a means of promoting recovery and verifying their BD diagnosis, as seen below:
"... like a lot of uhm psychiatrist just label uhm a lot of drug addicts as bipolar so that's why I'd like to learn more about it, and you can maybe differentiate between the two." (PAR03)
"I don't think it is really treated here… we get sent to the psychiatrist but … basically just to get me on pills it's not actually to help me manage… I haven't gained any knowledge of my BD." (PAR02)
Another participant explained that anyone going to a psychiatrist while intoxicated or withdrawing from stimulants would be diagnosed with BD. Yet another participant explained that substance use suppresses emotions and, when the use of drugs is discontinued, years of emotions rush out and create unstable moods that can be mistaken for BD. From these statements, it appears as if most participants firstly, view BD as a label or misdiagnosis, and secondly, deems knowledge on the causes, effects and management of their diagnosis as more beneficial than pharmacological treatment. In light of sub-theme 1.3, it appears that the participants found it difficult to take responsibility for managing a disorder when they question the accuracy of the diagnosis from the onset.
The following statement represents participants' belief that education should be extended to significant others as well:
"The people that are close to us, uhm should also be taught on uhm how to handle cravings … how to handle … us as, as addicts … because we are manipulative as well and they should be able to see past that." (PAR03)
With this quotation, it is evident that participants desire exposure to and the inclusion of other individuals in treatment.
Theme 3: All for One and One for All
All for one and one for all is a phrase used to indicate (1) that a group can support an individual, if the individual contributes to the group, and (2) that when individuals work together they can achieve both the group's goals and their personal goals. The interplay between shared experiences, while still maintaining individualised treatment, is explained in the next two sub-themes.
Sub-theme 3.1: Shared experiences
Group therapy and support groups are common in the treatment of both SUD and mental disorders, for example, Alcoholics Anonymous (AA), and Narcotics Anonymous (NA) groups. The following statements indicate why participants found groups beneficial:
"… in group therapy sessions … you process so much there and you just connect with the other people…and you're like 'oh my goodness I can relate to that'… it's not just me…" (PAR01)
"…the people that are here… that have been clean for long, and to see how they live and how their lives are coming right. It shows that there is hope." (PAR04)
"…we should invite people from the outside to join our groups or we should travel to the outside groups, which are already set out there and hear stories from different people … what got them through it." (PAR03)
It appears that groups can validate and normalise experiences for participants. One participant explained that having contact with other people who have recovered and are able to live 'normal' lives are a source of hope. In addition to hope, knowledge was an additional benefit derived from interaction with individuals who have maintained abstinence. Confrontation by counsellors and other individuals in recovery has long been a part of SUD treatment and was a beneficial and valued component of treatment for participants when appropriately utilised.
Sub-theme 3.2: Personal experiences
Exposure to individuals who share similar experiences appears to promote recovery; however, when experiences are generalised, individual needs are neglected and recovery demoted, as seen in the following quotations:
"… they must help guide you through that certain situation … because they tend to generalise it… instead of helping you through specific problems…" (PAR03)
"… for them, it was like a communication thing, they were like "aw, no we understand the way you feel if you have issues" and I was like oh well that's one way of looking at it. I was just doing it because it makes me feel better. Point. [explaining response from staff to self-harm]." (PAR02)
During interviews, two participants shared that they self-mutilated during treatment. The first participant saw self-mutilation as a means of communication, to show the treatment centre that he did not agree with certain aspects of treatment. The second participant experienced emotional relief when he self-mutilated; however, the treatment centre saw it as a way of communicating, instead of teaching him more effective coping mechanisms. It is evident that consideration of individual treatment needs should be taken into account as failing to do so could jeopardise long-term recovery.
Theme 4: In the Long Run
Essentially the objective of treatment is to ensure that an individual is able to achieve and maintain the highest possible personal level of functioning and not merely abstinence from substances of abuse. It appears that the most detrimental factor to long-term recovery is opposing treatment goals, as seen in the following quotes:
"I said to her specifically … I won't take anything that will make me pick up weight because I've got very bad body dysmorphic disorder... it's a trigger for me you know; when I used meth [methamphetamine] I was so lean it was the most beautiful feeling." (PAR01)
"...they have more addressed the issue of the substance abuse than the bipolar. No matter if, even if I come to them with my emotional problems, they rather just address religion and substance abuse." (PAR03)
In this case it appears as if the goal of the psychiatrist was to prescribe the most effective medication to address the biological component of BD. The goal of the participants was, however, to maintain a certain image that was being threatened by the prescribed medication, regardless of the fact that this concern was mentioned, and ignored. It can be assumed that this participant is at a high risk of non-adherence and relapse, as the negative effects associated with medication triggers discomfort, a discomfort that can be addressed by a stimulant.
Other participants stated that they believe that they were in the wrong 'type' of treatment centre because the goals they had for treatment and the focus of the treatment centre were different. The following comments expand on the participants' views:
"…spiritually, they do a good job here…That's why there is lacking in the other things." (PAR02)
"…I need to get affirmation…I seek that stuff…" (PAR01)
"…I think there should be more…confrontation group [sic], where we call people out on their bad behaviour, their addictive behaviour." (PAR03)
The quotations above highlight some opposing treatment goals, such as spirituality, confrontation and rewards.
Discussion
Generally, the initial focus of treatment falls on addressing biological components, for example, the prescription of medication to stabilise mood cycles in BD (Archambeault, 2009:108), and the use of medication to manage withdrawal symptoms associated with stimulant drug abuse (Rassool, 2011:94). Despite pharmacological intervention, most participants reported unstable moods that appeared to cause psychological discomfort and triggered cravings for stimulants. On the basis of similar observations, authors such as Fisher and Harrison (2013:151) described medication as a merely complementary therapy. Unfortunately, as researchers still debate the causes of DD, there are few studies focused on its treatment, apart from pharmacological interventions (Weiss, Griffin, Kolodziej, Greenfield, Najavits, Daley, Doreau & Hennen, 2007:100). As non-adherence to BD medication is estimated at 70%, there is a dire need for alternative forms of treatment (Miklowitz, 2010:45).
As participants did not have access to stimulant drugs during treatment, they turned to other substances and behaviours, termed cross-addictions, in an attempt to manage psychological stress, a phenomenon that is common among individuals in treatment for SUD (Fisher & Harrison, 2013:40). Common cross-addictions include food, sweets, exercise, caffeine, sex, gambling, nicotine, relationships and self-mutilation (Evren & Evren, 2005:19; Fisher & Harrison, 2013:290). As cross-addiction plays a functional role, it indicates that treatment needs are not being met and that certain BPS factors are neglected (Engel, 1981:103). Empowering individuals with skills to manage psychological stressors is crucial as cross-addiction poses a risk to recovery; for example, Frye and Perugi (2010:33) report that nicotine inhibits the effectiveness of bipolar treatment and aggravates symptoms.
In addition to cross-addiction, certain internal motivators such as a sense of responsibility encouraged participants to remain in treatment. Taking responsibility for recovery appeared to be an individual process, not deliberate or guided, motivated by personal drive or the anticipation of gaining something. One participant perceived 'taking responsibility' for recovery as an opportunity to restore interpersonal relationships, where another was so focused on getting through treatment that he neglected to disclose and address psychological discomfort, thus not taking responsibility for recovery. 'Taking responsibility' should be a topic of interest during treatment and reintegration; however, treatment goals should be realistic and take place in an appropriate timeframe to promote recovery (Miklowitz, 2010:27). Social workers should ensure that service users take responsibility for their treatment and cooperate with the treatment plan, which includes disclosure of underlying disparities that caused stress (Engel, 1981:102). It is noteworthy that responsibility was only expressed concerning SUD treatment as, so we believe, all participants questioned their BD diagnosis, describing it as a label or misdiagnosis. Swann (2010:278) acknowledges that misdiagnosis is common as stimulant drugs mimic symptoms of hypomania; however, NIDA (2010:7) emphasises the need for an accurate diagnosis, as treatment goals and ultimately treatment outcomes will depend on the diagnosis made.
All participants considered counselling as the most beneficial part of treatment, as it was the most effective way of relieving psychological stressors and managing unstable moods, despite medication. In support of this view, research findings indicate that a safe environment where individuals can share perceptions and experiences has been found to be beneficial in the treatment of both SUD (Fisher & Harrison, 2013:57) and BD (Archambeault, 2009:118). Focusing on various BPS components of treatment is necessary, as focus on only one indicates possible neglect of another (Hatala, 2012:52). Most participants expressed a need for more counselling, while one participant, receiving counselling from different professionals, expressed satisfaction with counselling. Services provided by different disciplines seem to be effective and is encouraged by Rassool (2011:228), who describes addiction and mental disorders as a multidisciplinary problem and encourages professionals to work together.
Pharmacotherapy in the treatment of both BD and SUD aids in the management of symptoms because of their effect on neurotransmitters (Miklowitz, 2010:41; Nutt, 2012:69). Zastrow (2012:359) explains that, in addition to other physiological and psychological effects, physical exercise influences these same neurotransmitters. In support of these views, participants appeared to value the psychological benefits associated with exercise more than its physiological benefits. Bordbar and Faridhosseini (2012:324) hold that knowledge regarding how lifestyle influences psychological symptoms and the effectiveness of medication, as well as knowledge regarding side effects of medication, needs to form part of treatment. Interestingly, some participants expressed a need for education in this regard.
Psycho-education that includes emotional, behavioural and cognitive therapies can ensure that individuals develop coping skills to manage psychological and social stressors as well as identifying triggers for both disorders (Miklowitz, 2010:27; Weiss et al., 2007:101). Acceptance of a diagnosis is important, as individuals are more likely to access services if they believe they need it and if they believe the service provider can fulfil these needs (Engel, 1981:102). Acceptance and utilisation of treatment lead to lower relapse rates, which ensures better health outcomes for individuals as well as lowered psychological and financial strain on families and healthcare systems (Fisher & Harrison, 2013:56). Some participants mentioned that psycho-education should include family members, a need supported by researchers, who indicate that lower relapse rates occur when patients and families received information on both disorders and treatment options, while fostering realistic expectations regarding recovery and treatment (Miklowitz, 2010:27; Rassool, 2011:226).
Social workers and other members of the multidisciplinary team should consider the effect of culture, because high instances of social exclusion and political turmoil, as is the case in the RSA and most developing countries, generally leads to higher rates of mental health problems and SUD (Lachman et al., 2012). Additionally, treatment of mental health is often insufficient in multicultural countries, as Western culture primarily informs treatment methods, which are not always appropriate in multicultural settings (Allott, cited in Archambeault, 2009:27). In fact, the Framework for Social Welfare Services (DSD, 2013b:29) calls on service providers to render services on a continuum ranging from prevention to aftercare and reintegration services and discourages over-reliance on treatment along.
Traditional treatment of both mental disorders and SUD includes group therapy, as it creates a platform where individuals can share experiences, achieve the common goal of recovery, and build supportive relationships while gaining knowledge and hope (Fisher & Harrison, 2013:144). Fisher and Harrison (2013:151) warn that the needs of individuals should be considered and guide treatment, as not everyone will derive the same benefits from groups. The idea that individuals should receive treatment based on their individual needs is the very essence of the BPS perspective (Engel, 1981:102). Therefore, adapting programmes to the multivariate nature of SUD and BD is essential to promote effective treatment (Merikangas & Peters, 2010:56).
In terms of the treatment of DD, most researchers agree that both disorders need to be treated simultaneously as the neglect of one disorder can cause relapse in both disorders (Camacho & Frye, 2010:190). In the USA Weiss (2004) implemented outpatient groups focused on the DD of BD and general SUD when they discovered that separate treatment groups often had opposing goals, triggering a relapse. For example, should an NA group discourage the use of any medication and a BD support group is uninformed regarding the behaviours indicating SUD, the relapse of either disorder could be overlooked thus leaving service users (i.e., participants) without appropriate support to maintain the best possible quality of life given their DD (Miklowitz, 2010:301). Salloum et al. (2010:354) explain that treating an acute disorder is normally successful and achieved easily, but the focus shifts to maintaining long-term stability when multiple chronic disorders such as BD and SUD need to be treated simultaneously. As recovery is a lifelong process, it is important to ensure that service users and their families are included in goal setting and that they understand and approve the treatment plan, as this promotes treatment adherence and long-term recovery in both disorders (Fisher & Harrison, 2013:151; Miklowitz, 2010:27). Discomfort caused by opposing treatment goals was evident during interviews with participants and was caused by various aspects, such as disagreements in terms of medication, religion, a lack of rewards and the inappropriate use of confrontation in treatment. In an attempt to deliver adequate services, social workers are urged to understand the BPS aspects determining the onset, course and progression of both disorders to ensure effective treatment and allow sufficient time for recovery and reintegration (Fisher & Harrison, 2013:49).
All the findings reached in this study should ultimately inform policy development. Archambeault (2009:118) urges social workers to accept the influence they have on policies that guide the development of intervention protocols. Policies should ensure that treatment respects multicultural societies such as the RSA, where appropriate interventions should especially infiltrate the primary health care system (Jack et al., 2014:7). Jack et al. (2014:2) acknowledge that, unfortunately, discussions regarding the implementation of the national health insurance in the RSA do not focus on mental health care services as part of the primary health care system at this stage, although a lack of trained staff is another pitfall facing the RSA.
The article aimed to describe how adults living with the DD of stimulant use disorder and BD experience treatment. The authors believe this is the first study in the RSA that aimed to explore how treatment is experienced. The research sample, however, does not represent the experiences of individuals in public or psychiatric treatment programmes, or those diagnosed with different dual diagnoses. Another limitation includes the absence of all ethnic groups in the RSA, as all the participants who volunteered their participation in this study were white.
The goal of phenomenological studies is not generalisability but rather understanding the meanings assigned to experiences. The goal of the phenomenological approach coupled with steps taken to ensure the trustworthiness of the study has the potential not only to have an impact on individual lives in the RSA, but also on those in other developing countries, especially those in Southern Africa.
Conclusions
The nature of the study allowed for the gathering of rich data focusing on a diverse range of aspects moulding the experiences of participants. The authors believe that the conclusions and recommendations outlined below highlight the most important aspects of this phenomenon.
In general, DD has become a topic of interest in recent years and research focused on various types of DD is necessary for the establishment of effective treatment. A lack of epidemiological data on the prevalence of both stimulant use disorder and BD globally, and in the RSA specifically, means the prevalence and actual impact of this DD on individuals and society is unknown. In addition, the development of effective treatment will be inhibited as well, effectively delaying recovery and escalating negative effects, supporting the call of various authors for more research.
Similarities regarding the effects of stimulant use and BD overlap on various levels. Biologically, the same neurotransmitters are involved in the course and progression of both stimulant use disorder and BD. Compared to individuals with no diagnosis, those diagnosed with SUD or BD has been found to have poor psychological health in general. The financial and emotional strain placed on social systems, such as families and governments, are more severe when BD or stimulant use is diagnosed. As numerous risk factors, causes and effects associated with the development and course of BD and stimulant use overlap, it can be assumed that individuals will be prone to develop both disorders. In the absence of a DD and the holistic treatment thereof, the poor outcome of treatment is inevitable.
Concerning the treatment, pharmaceuticals are common in the treatment of biological components associated with BD and managing withdrawal associated with stimulants. Treatment of psychological components seems more complex as stimulants are described as more psychologically addictive than physically addictive, whereas individuals diagnosed with BD need to become comfortable with the idea of living without the presence or anticipation of manic episodes. In general, treatment outcomes are more favourable when social systems are included in treatment and support recovery.
It is clear that pharmacological treatment and a formal diagnosis was not sufficient in managing symptoms or encouraging individuals to take ownership of their recovery. Rather, psycho-education and counselling were seen as the most beneficial aspects addressing the psychological needs of individuals living with this specific DD. Education in terms of lifestyle, treatment options and outcomes of treatment should be addressed. The individual needs of patients should be respected and guide treatment on a continuous basis and all physical, cognitive and interpersonal factors that can promote recovery should be included; for example, exercise, group therapy and religion/spirituality. Treatment groups seem to have the most profound impact and act as a source of education and motivation while providing hope for full recovery while addressing the lack of available social workers and other service providers in the RSA.
Social workers, service users and family members should understand and acknowledge the risks and effects of secondary problems as well; for example, nicotine can aid in managing depressive moods; however, individuals using nicotine have been found to be more resistant to BD medication, making mood relapse more probable. More in-depth and treatment-specific education for social workers in DSD and other service providers in DoH in the RSA is, however, a crucial step in developing and treating DD effectively.
The inclusion of professionals and policy developers is important, as the divide between psychiatric services headed by the DoH, and SUD services headed by the DSD has caused a treatment gap to develop where those most in need of services are lost. Echoing this recommendation, SACENDU (2017:27) expresses a need for lobbying for resources directed to understanding and addressing this growing phenomenon.
Future research should repeat this study in private and government-based treatment centres across the RSA. Results from different studies should also be compared to determine the most prominent treatment needs. Treatment programmes should be developed, implemented and evaluated to determine if treatment needs have been met.
References
APA - American Psychiatric Association. 2013a. Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Association. [ Links ]
American Psychiatry Association. 2013b. Highlights of changes from DSM-IV-TR to DSM-5. [Online] Available: http://www.dsm5.org/documents/changes%20from%20dsm-iv-tr%20to%20dsm-5.pdf [Accessed: 07/08/2018]. [ Links ]
Archambeault, J. 2009. Reflective reader: Social work and mental health. London: Learning Matters Ltd. [ Links ]
Bordbar, M.R.F. & Faridhosseini, F. 2012. Psychoeducation for Bipolar Mood Disorder. In: Juruena, M.F. (ed). Clinical, Research and Treatment Approaches to Affective Disorders. [Online] Available: http://edengalaxy.com/images/PDFs/6%20bipolar%20expert%20specialist%20manic%20treatment%20psychology.pdf [Accessed: 07/07/2018]. [ Links ]
Brensilver, M., Heinzerling, K.C. & Shoptaw, S. 2013. Pharmacotherapy of amphetamine-type stimulant dependence: An update. Drug and Alcohol Review, 32:449-460. [ Links ]
Camacho, A., Ng, B. & Frye, M.A. 2010. Modafinil for bipolar depression with comorbid methamphetamine abuse. American Journal on Addiction, 19:190-191. [ Links ]
Clarke, V. & Braun, V. 2013. Teaching thematic analysis: Overcoming challenges and developing strategies for effective learning. Psychologist, 26(2):120-123. [ Links ]
Clarke, V., Braun, V. & Hayfield, N. 2015. Thematic Analysis. In: Smith, J.A. (ed). Qualitative Psychology: A Practical Guide to Research Methods. (3rd ed). London: Sage. [ Links ]
Creswell, J.W. 2013. Qualitative inquiry & Research design: Choosing among five approaches. (3rd ed). London: Sage Publications. [ Links ]
DSD - Department of Social Development. 2013a. National Drug Master Plan 2013-2017. [Online] Available: http://www.gov.za/sites/www.gov.za/files/National%20Drug%20Master%20Plan_2013-17.pdf. [Accessed: 07/08/2018] [ Links ]
DEPARTMENT OF SOCIAL DEVELOPMENT. 2013b. Framework for Social Welfare Services. [Online] Available: http://www.dsd.gov.za/index2.php?option=com_docman&task=doc_view&gid=515&Itemid=19. [Accessed: 18/09/2018]. [ Links ]
Engel, G.L. 1981. The clinical application of the biopsychosocial model. Journal of Medicine and Philosophy, 6:101-123. [ Links ]
Evren, C. & Evren, B. 2005. Self-mutilation in substance-dependent patients and relationship with childhood abuse and neglect, alexithymia and temperament and character dimensions of personality. Drug and Alcohol Dependence, 80:15-22. [ Links ]
Fabricius, V., Langa, M. & Wilson, K. 2007. An exploratory investigation of co-occurring substance-related and psychiatric disorders. Journal of Substance Use, 1-16. [ Links ]
Fisher, G.L. & Harrison, T.C. 2013. Substance abuse: Information for schools counselors, social workers, therapists and, counselors. (5th ed). Upper Saddle River, NJ: Pearson Education. [ Links ]
Frye, M.A. & Perugi, G. 2010. Comorbidity in bipolar disorder: A focus on addiction and anxiety disorders. In: L.N. Yatham, & Maj, M. (eds.). Bipolar disorder: Clinical and neurobiological foundations. West Sussex: Wiley-Blackwell. [ Links ]
Grobler, C. 2012. A cross-sectional descriptive study of clinical features and course of illness in a South African population with bipolar disorder. Pretoria: University of Pretoria. (Medicinae Doctor dissertation) [ Links ]
Hatala, A.R. 2012. The status of the "Biopsychosocial Model in health psychology: Towards an integrated approach and a critique of cultural conceptions. Open Journal of Medical Psychology, 1:51-62. [ Links ]
Isaacs, A.N. 2014. An overview of qualitative research methodology for public health researchers. International Journal of Medicine and Public Health, 4(4):318-323. [ Links ]
Jack, H., Wagner, R.G., Petersen, I., Thorn, R., Newton, C.R., Stein, A., Kahn, K., Tollman, S. & Hofman, K.J. 2014. Closing the mental health treatment gap in South Africa: A review of the costs and cost-effectiveness. Global Health Action, 7(23431). [Online] Available: http://dx.doi.org/10.3402/gha.v7.23431 [Accessed: 07/08/2018]. [ Links ]
Lachman, A., Nassen, R., Hawkridge, S., & Emsley, R.A. 2012. A retrospective chart review of the clinical and psychosocial profile of psychotic adolescents with co-morbid substance use disorders presenting to acute adolescent psychiatric services at Tygerberg Hospital. South African Journal of Psychiatry, 18(2):53-60. [Online] Available: http://www.sajp.org.za/index.php/sajp/article/view/351/308. [Accessed: 07/08/2018]. [ Links ]
Lietz, C.A. & Zayas, L.E. 2010. Evaluating qualitative research for social work practitioners. Advances in Social Work, 11(2):188-202. [ Links ]
Matsea, T.C. 2017. Strategies to destigmatize mental illness in South Africa: Social work perspective. Social Work in Health Care, 56:367-380. [ Links ]
Merikangas, K.R. & Peters, T.L. 2010. Update on the Epidemiology of Bipolar Disorder. In: Yatham, L.N. & Maj, M. (eds.). Bipolar Disorder: Clinical and Neurobiological Foundations. West Sussex: Wiley-Blackwell. [ Links ]
Miklowitz, D.J. 2010. Bipolar disorder: A family-focused treatment approach. (2nd ed). New York, NY: Guilford Press. [ Links ]
NAMI - National Alliance on Mental Illness. 2013. Dual Diagnosis: Fact Sheet. [Online] Available: http://www2.nami.org/factsheets/dualdiagnosis_factsheet.pdf. [Accessed: 28/04/2015] [ Links ]
National Institute on Drug Abuse. NIDA 2010. Comorbidity: Addiction and other mental illnesses. [Online] Available: http://www.drugabuse.gov/publications/research-reports/comorbidity-addiction-other-mental-illnesses/letter-director [Accessed: 28/04/2015]. [ Links ]
NIEUWENHUIS, J. 2016. Introducing qualitative research. In: Maree, K. (ed). First steps in research. (2nd ed). Pretoria: Van Schaik. [ Links ]
Nutt, D. 2012. Drugs without the hot air: Minimising the harms of legal and illegal drugs. Cambridge: UIT Cambridge. [ Links ]
PADGETT, D.K. 2017. Qualitative methods in social work research. (3rd ed). London: Sage. [ Links ]
Pasche, S. & Myers, B. 2012. Substance misuse trends in South Africa. Human Psychopharmacology: Clinical and Experimental, 27:338-341. [ Links ]
Rassool, G.H. 2011. Understanding addiction behaviours: Theoretical & clinical practice in health and social care. Hampshire: Palgrave Macmillan. [ Links ]
Republic of South Africa. (RSA) 2018. South Africa's provinces. [Online] Available: https://www.gov.za/about-sa/south-africas-provinces. [Accessed: 07/08/2018]. [ Links ]
Routledge, L. 2005. Substance abuse and Psychological Well-being of South African Adolescents in an urban context. Pretoria: University of Pretoria. (Master of Arts dissertation) [ Links ]
RUBIN, A. & BABBIE, E. 2017. Research methods for social work. (9th ed). Boston, MA: Cengage Learning. [ Links ]
Salloum, I.M., Pani, L. & Cooke, T. 2010. Management of comorbidity in bipolar disorder. In: L.N. Yatham, & Maj, M. (eds). Bipolar disorder: Clinical and neurobiological foundations. West Sussex: Wiley-Blackwell. [ Links ]
SACENDU - South African Community Epidemiology Network on Drug Use. 2017. Research Brief: Monitoring Alcohol, Tobacco and Other Drug Use Trends in South Africa (July 1996 - June 2017). [Online] Available: http://www.mrc.ac.za/sites/default/files/attachments/2017-10-27/SACENDUBriefJuly2017.pdf. [Accessed: 07/08/2018]. [ Links ]
Swann, A.C. 2010. The strong relationship between bipolar and substance-use disorder: Mechanisms and treatment implications. Annals of the New York Academy of Sciences, 1187:276-293. [ Links ]
Tiet, Q.Q. & Mausbach, B. 2007. Treatments for patients with dual diagnosis: A review. Alcoholism: Clinical and Experimental Research, 31(4):513-536. [ Links ]
United Nations Office on Drugs and Crime. 2017. World Drug Report: Executive Summary. [Online] Available: https://www.unodc.org/unodc/en/scientists/world-drug-report-2017---executive-summary-conclusions-and-policy-implications.html. [Accessed: 07/08/2018]. [ Links ]
Weiss, R.D. 2004. Treating patients with bipolar and substance dependence: Lessons learned. Journal of Substance Abuse Treatment, 27:307-312. [ Links ]
Weiss, R.D., Griffin, M.L., Jaffee, W.B., Bender, R.E., Graff, F.S., Gallop, R.J. & Fitzmaurice, G.M. 2009. A "community-friendly" version of integrated group therapy for patients with bipolar disorder and substance dependence: A randomized controlled trial. Drug and Alcohol Dependence, 104:212-219. [ Links ]
Weiss, R.D., Griffin, M.L., Kolodziej, M.E., Greenfield, S.F., Najavits, L.M., Daley, D.C., Doreau, H.R. & Hennen, J.A. 2007. A randomized trial of integrated group therapy versus group drug counselling for patients with bipolar mood disorder and substance dependence. American Journal of Psychiatry, 164:100-107. [ Links ]
West African Commission on Drugs. 2014. Not just in transit: Drugs, the state, and society in West Africa. [Online] Available: http://www.wacommissionondrugs.org/report/ [Accessed: 07/08/2018] [ Links ]
Zastrow, C.H. 2012. Social work with groups: A comprehensive worktext. (8th ed). Stamford, CT: Cengage Learning. [ Links ]

{kind=link}
{kind=link}