










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.80 n.1 Johannesburg Feb. 2025
ETHICS
Adverse event, negligence or malpractice: The debate revisited
L SykesI; J BesterII; B EvansIII
IBSc, BDS, MDent, IRENSA, Dip Forensic Path, Dip ESMEA, FCD (Pros), Head of Department of Prosthodontics, University of Pretoria, South Africa. ORCID: 0000-0002-2002-6238
IIPhD, Department of Physiology, School of Medicine, Faculty of Health Sciences, University of Pretoria, South Africa. ORCID: 0000-0002-8931-9194
IIIBDS, Dip Orth, ex Department of Orthodontics, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
Determining whether an incident in healthcare is an adverse event, negligence or malpractice can be challenging. The authors previously proposed a three-pronged model considering the magnitude of harm, the frequency of similar incidents and the intention behind the actions. However, on reflection and testing, they have identified limitations in the model. Magnitude is subjective, frequency is difficult to gauge and intention is impossible to assess. The authors now propose a refined template that replaces Frequency with Perceived Harm, better defines how Magnitude can be gauged and replaces Intention with a more objective measure of Fitness for Purpose. It also introduces a fourth category of Accountability (a measure of professionalism). The updated model includes a graphical representation using Visual Analogue Scales, with the aim to aid in determining whether an incident is an adverse event, negligence or malpractice. The respondents/assessors will mark a point on each of the four scales that best indicates their assessment of that category. These points can then be measured and the totals used to rank the severity of the incident. This paper once again emphasises how important it is for clinicians to maintain accurate and detailed records, the need for teaching and practicing evidence-based medicine, of prioritising the patient's best interests, and of timely reporting of suspected misconduct to the HPCSA in order to protect patients.
INTRODUCTION
In a previous paper the authors explored the challenges faced in considering cases of suspected negligence.1 They proposed guidelines to help practitioners decide when an unfortunate incident could be considered an adverse event, and when it may be regarded as negligence or malpractice. One of the most popular and objective standards by which conduct is usually judged is the "reasonable person rule". This states that "a person has acted negligently if he/she has departed from the conduct expected of a reasonably prudent person acting under similar circumstances.2,3 Legally, to establish negligence it must be proven that the defendant had a duty to the claimant, the defendant breached that duty by failing to conform to the required standard of conduct, the claimant was harmed in some way, and that the defendant's negligence was the cause of the harm or damage incurred.2,3 The previous paper delved into the history of how this measure came into existence and use, noting that in the medical/dental context, the standard by which conduct is measured is that expected of a reasonably skilled, competent and experienced person who is also a trained and qualified member of the profession.2,3 The law does recognise that in emergencies "even a reasonable person could make errors in judgement, and that conduct is evaluated in light of whether he/she acted reasonably under the circumstances".2,3 The paper then explored the issue of trying to establish proof of negligence. This usually entails an expert witness evaluating the incident based on the Information provided, scientific evidence, consideration of how a reasonable clinician, under the same circumstances, would be expected to act, and the standard of care that was given.2,3 The expert may also comment on situations where the patient acted negligently and so added to the injury. This sort of "contributory negligence" by the patients generally results in them not being able to claim for damages.2,3 The authors of the previous paper proposed a three-pronged model that could be used to help determine if an unfortunate outcome was an adverse event or the result of negligence or even malpractice. That model evaluates each case by looking at three factors - the magnitude of the harm, the frequency with which the practitioner had committed similar damages and the intention behind the initial actions.
However, after some years of reflection, and testing the model on real-life situations, the authors have become uncomfortable with it for several reasons. Magnitude is difficult to determine and is open to subjective interpretation. What a clinician may consider as minor harm may be felt and experienced by a patient as a major problem, and vice versa. Furthermore, practitioners may not agree among themselves on what constitutes minor or major harm. Similarly, some patients will be able to endure and heal from extensive trauma while others may continue to suffer from seemingly insignificant damages. The perception of harm can therefore vary significantly between individuals, influenced by factors such as personal experiences, cultural background and psychological resilience.
This subjectivity in assessing harm extends beyond the patient-clinician relationship to include differences among healthcare professionals, patients' family members and even regulatory bodies. Moreover, the long-term impact of an adverse event may not be immediately apparent, further complicating the assessment of its magnitude and potential consequences. With regards to frequency, the original paper argued that "an isolated adverse occurrence could be due to patient factors, the clinical situation, unavoidable damage or human error; however, repeated injurious incidents contribute towards the suspicion that the practitioner is guilty of negligence or malpractice".1 But the frequency may be hard to gauge as the evaluator generally does not know how much other harm the practitioner has caused, to how many patients, over what period, under what circumstance, and the extent of the harm. In addition, there may be many patients who have suffered some form of harm but do not know where or how to report these experiences. Unless the evaluators are provided with this additional information they can base their opinions only on the immediate case at hand. The major gap in the previous model revolves around the issue of intent. Intention is defined as "a purpose, objective, hope or aim. It's something a person means to do, and which guides their planned actions, regardless of whether they manage to achieve this goal or not."4 In the event of an adverse event, it is very difficult to assess whether it happened as a result of a malicious intention, in which case it could constitute negligence or malpractice. While it is admittedly perplexing to identify, or to accurately postulate, the intent behind another person's actions, nevertheless the authors believe that regardless of the frequency or magnitude, a bad intention can never be condoned, and any treatment emanating from this is potentially unethical. Consequently, any adverse event that resulted from an unintentional lapse should automatically be considered negligence, malpractice if there was a deliberate departure from what was expected.5
Proposed updated model
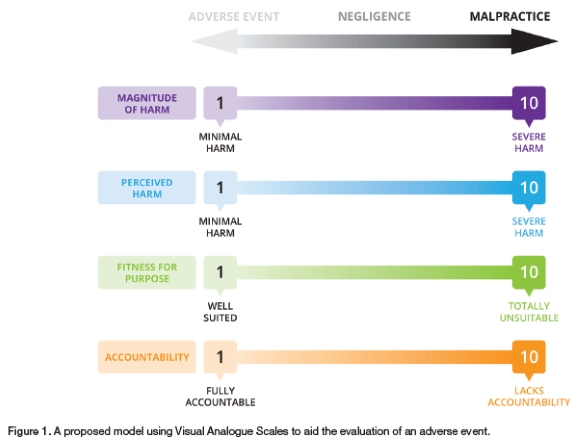
Based on the above limitations and shortfalls in the original model, the authors now propose a more detailed and refined template (Figure 1). Magnitude is still an important consideration and can be judged by comparing the behaviour with what would be expected from another clinician acting in a similar situation using the "reasonable clinician rule".Frequency has now been replaced with Perceived Harm. There are a variety of harms that a person may have suffered. In the medical context these may include, but are not limited to: pain and suffering, physical damage, unacceptable aesthetics, time and costs, stress, psychological duress or inconvenience. The extent, severity and impact of the perceived harm may be evaluated by engaging in conversations with the patients to try to determine how it has impacted on their quality of life. Regarding Intent, as mentioned, nobody can know precisely the motivation behind another person's actions. However, the situation and therapy provided can be evaluated under a new category of Fitness for Purpose. By definition this entails "an undertaking, whether expressed or implied, that imposes an obligation on the provider to plan and deliver a service that is appropriate for its intended purpose and is suited to the patient's individual needs".6
Here one may consider issues such as accuracy of the diagnosis, appropriateness of the intervention, correctness of choice, necessity, anticipated therapeutic benefits, whether it was within the practitioner's scope of practice, risk versus benefits, expected outcomes and prognosis, fees charged, provision of added excessive services, planning, communication and patient autonomy. Remember that in some cases, treatment may seem to have been for purely cosmetic purposes, and it is easy to accuse the practitioner of avarice. However, we must be cognisant that many times patients will demand these services regardless of the biological costs and will "shop around" until they find someone who is prepared to deliver. The ethical concern is that the patient may resort to being treated by non-medical persons who could cause even more harm. A clinician may feel justified to accede to the patient's demands if the treatment may limit or mitigate against possible future harm. At such times communication and detailed record-keeping are mandatory to protect the practitioner.It is important to recognise that patient autonomy plays a significant role in these situations, and practitioners often face difficult ethical dilemmas when balancing patient desires with potential health risks.
In the updated model, the modified three factors are still considered together, but a fourth category has now been added, that of Accountability.5 This requires four actions from the practitioner: acknowledgment of the harm, taking responsibility for its occurrence, communicating the relevant details to the patient, and instituting reasonable actions of management in order to either rectify or remediate the situation to lessen the patient's distress.5
The proposed new model then suggests using Visual Analogue Scales (VAS) of each of the four elements to help assess and measure the severity of an adverse event. VAS are measurement tools used to assess subjective experiences such as pain, discomfort or other sensations, and subjective opinions. They are useful in clinical and research settings to quantify feelings or perceptions that are difficult to measure directly. A VAS is a straight line, the ends of which are labelled as the extreme boundaries of the condition being measured. Participants are asked to respond by placing a mark through the line at a position which best represents their current perception of a given phenomenon between the labelled extremes.7 The position of the mark on the line can then be measured to provide a numerical value. The numerical value can be interpreted according to established thresholds or norms for the specific experience being measured. The lines may be horizontal or vertical, and any length deemed appropriate, but the most common form is a 100 millimetre (10cm) horizontal line, as studies have shown this configuration to produce a more uniform distribution of scores with less error variance.8,9 Visual analogue scales are valuable tools due to their simplicity, being easy to administer and understand and requiring minimal training for users. They are considered to be sensitive enough to detect small changes in feelings or conditions since they provide a continuum of responses. They are non-invasive, and don't need any special tools or laboratory procedures.
Disadvantages are that they are subjective and rely on individual perceptions, which can vary from person to person. They are prone to cognitive bias wherein responses may be influenced by various factors, including mood or understanding of the task. There may be cultural differences in perceptions which can potentially affect the validity of results. However, it is generally agreed that VAS can be valuable tools in both clinical practice and research, allowing for a quantifiable assessment of subjective experiences. When used appropriately, they can enhance our understanding of feelings and guide decisions.This model proposed using four simple 10-point VAS (or an open line of 10cm) as illustrated in Figure 1 to help external assessors rate and appraise any unforeseen outcome of treatment. They will make a mark along the line at the point that most closely reflects their perceived judgement of that category. These points will be measured and a score of between 1 and 10 recorded based on the measured distance. The four scores can be added and averaged to give a final numerical value.
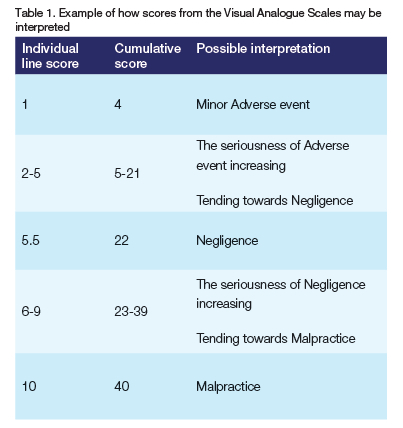
This can then be used to help justify the decision as to whether the incident should be considered an adverse event, negligence or malpractice. By default, the minimal score in any of the four categories has to be 1 and not zero, as zero would reflect that there had been no unforeseen occurrence. Thus, scores may range from 4 to 40, with 4 reflecting a minor adverse event and 40 unquestionable malpractice. The mid-point of 22 would be considered negligence. Table 1 illustrates how the individual and cumulative VAS ratings may be interpreted. Note that the baseline is 1 and not zero, resulting in 9 (36) possible scoring points. The assessor needs to consider each line independently, as well as the cumulative total, as the latter gives a more rounded, global and objective overview. It could also allow a high score in one category, which when viewed in isolation is worrying, to be cancelled out or lessened by low scores in the others.
CONCLUSIONS
All healthcare interventions carry with them a risk of error or failure. Complications can and do occur, and it is impossible to restore every patient to optimal states of health or to satisfy all their medical needs. However, in determining whether a less-than-ideal outcome is due to some fault on the part of the clinician, and if so whether it should be considered an unfortunate adverse event, negligence or malpractice, some pertinent questions may be asked. These include whether the intervention was aimed at providing a therapeutic benefit, protecting the patient, preventing harm, removing conditions that could lead to future harm and promoting the best interests of the patient. The proposed model can be used as an aid when evaluating the situation as it allows one to consider several crucial factors simultaneously. All suspected incidents of negligence or malpractice should be documented and ideally also be reported timeously to the HPCSA. Repeated offences could signify a trend that would warrant Council investigation and intervention to protect future patients. At the same time, to protect clinicians against malpractice suits, there needs to be a stronger emphasis on teaching and practicing "evidence-based" medicine along with meticulous and accurate record keeping, while also emphasising the need to always place the patient's best interest at the centre of any intervention.
REFERENCES
1. Sykes LM, Evans WG, Dullabh HD. Negligence versus Malpractice. Part 14: The "Reasonable Person Rule". SADJ 2017, Vol 72, 9, 430-432 [ Links ]
2. Legal Dictionary L. The free dictionary - Negligence. Accessed on: 10-05-2017; Accessed at: http://legal-dictionary.thefreedictionary.com/Negligence [ Links ]
3. Law and Legal Definitions. Reasonable Man Theory Law & Legal Definition. definitions. uslegal.com/r/reasonable-man-theory. Accessed on: 01-05-2016; Accessed at: definitions.uslegal.com/r/reasonable-rnan-theory [ Links ]
4. Cambridge Dictionary. Definition of Intention. Accessed at: https://dictionarycambridge.org/dictionary/english/intention [ Links ]
5. Negligence versus malpractice: Understanding the key differences https://cummingsinjurylaw.com/medical-malpractice/negligence-vs-malpractice-understanding-the-key-differences/5. Naidoo S, Moodley K. Ethics and the dental team. Schaik V editor. Hatfield, Pretoria: Van Schaik; 2009. 136 [ Links ]
6. Theessen T & Milner H. Fitness for purpose clauses in construction contracts should be approached with caution. Accessed at: https://www.webberwentzel.com/News/Pages/fltness-for-purpose-clauses-in-construction-contracts-should-be-approached-with-caution.aspx#; Accessed on 21-11-2024 [ Links ]
7. Wewers ME & Lowe NK. A critical review of visual analogue scales in the measurement of clinical phenomena. Research in Nursing & Health, 1990, 13, 227-236 [ Links ]
8. Revill SI, Robinson JO, Rosen M & Hogg MIJ. The reliability of a linear analogue for evaluating pain. 1976; Anesthesia,31, 1191-1 198 [ Links ]
9. Scott J & Huskisson EC. Graphic representation of pain. 1976; Pain, 2, 175-184 [ Links ]
 Correspondence:
Correspondence:
Leanne Sykes
Email: Leanne.sykes@up.ac.za
Author's contribution
1. Leanne Sykes - primary author (60%)
2. Janette Bester (20%)
3. Bill Evans (20%)
