










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.79 n.9 Johannesburg 2024
RADIOLOGY CORNER
Focal osteomyelitis with proliferative periostitis
Zarah Yakoob
BChD, PDD (Maxillofacial and Oral Radiology), MSc (Maxillofacial and Oral Radiology), PGDip General Management, MBA (GIBS Pret). Department of Oral and Maxillofacial Pathology, School of Dentistry, Faculty of Health Sciences, University of Pretoria, South Africa. ORCID: 0000-0003-1966-5574
CASE
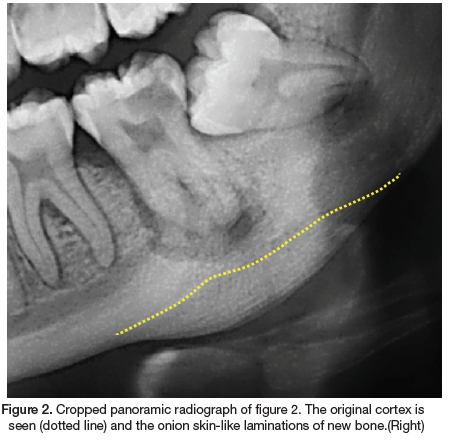
A 22-year-old female presented to our clinic with the main complaint of pain and swelling in the left mandible. The medical history revealed no co-morbidities. Extraoral examination revealed a draining sinus and a hard, firm swelling in the posterior left mandible. Intraoral examination revealed multiple carious teeth and healthy overlying mucosa. A panoramic radiograph was performed (Figure 1). Radiographic examination revealed a missing 18, impacted 28, 38, 48 and carious lesions on the 17, 15, 37 and 36. A periapical radiolucency is associated with the grossly carious 37 and in addition a convex radiopacity and onion skin-like periosteal reaction is noted, whereby numerous layers of new cortical bone is deposited in relation to the 37. The radiopacity extent includes the 37 area, with the affected bone appearing more sclerotic and dense. The adjacent cortical bone is normal. The periosteal reaction resulted in expansion of the cortical border, whilst remaining intact. There is a clear demarcation of the original cortical border and the new bone deposition (Figure 2). As the clinical and radiographic features were consistent with that of focal osteomyelitis with proliferative periostitis, a definitive diagnosis was made without the need for histological investigations. Subsequently, the grossly carious 37 was extracted and antibiotics was prescribed. The patient responded well to the treatment and treatment of the other carious lesions has commenced.
INTERPRETATION
The entity of focal osteomyelitis with proliferative periostitis has been referred to as Garre's osteomyelitis and periostitis ossificans. In 1893 Carl Garre first described this form of periosteal reaction and it was subsequently termed Garre's osteomyelitis.1,2 Many authors in recent years reported that Garre's osteomyelitis is considered a misnomer. The term periostitis ossificans is also considered incorrect as the periosteum itself does not ossify. Therefore, the most accepted term is focal osteomyelitis with proliferative periostitis. In the jaw bones, the posterior mandible and first molar region is the most common site. Due to the periosteal osteoblastic activity in younger individuals, this entity is common in children and adolescents and rarely found in the elderly. Odontogenic infections, in particular severe dental caries with associated periapical inflammation is the most commonly reported cause of focal osteomyelitis with proliferative periostitis.3,4 There have been reports of other less common causes, including post operative infection after an extraction and periodontitis. In cases where there is no obvious source of infection, an immunologically mediated aetiopathogenesis should be explored.5
As a response to inflammation caused by a persistent low-grade infection, subperiosteal bone is formed over the surface of the affected bony area. Clinically, this results in a hard tissue-like swelling of the affected side, that may result in facial asymmetry. Pain may be associated and in severe cases trismus may occur. In addition, the overlying skin may present with signs of inflammation such as redness and sinus tracts. Intraorally, the affected mucosa typically appears normal.1,2
Histologically, the affected bone forms multiple layers of bone in a parallel fashion, with an intact cortex. Radiographically, a convex radiopaque area is seen in the affected area, with parallel layers in relation to the source of infection. Depending on the radiographic angulation, occasionally radiolucent layers can be seen as a soft tissue zone between the bony laminations and the original cortex. This radiographic appearance is often referred to as "onion skin".3
The thickened periosteum over time results in a thickened sclerotic bony appearance. These unique radiographic features can often be missed on a periapical radiograph. A panoramic radiograph, occlusal radiographs and cone beam computed tomography have the ability to visualise the new bone formation.2
As the cause of focal osteomyelitis with proliferative periostitis is usually as a result of odontogenic infection, it has been accepted that elimination of the cause and antibiotic therapy will result in resolution of the infection with eventual remodelling of the affected bone. The most common treatment option is extraction of the affected tooth, however, there have been reported cases of successful outcomes through endodontic treatment.2,4
AUTHORS DECLARATION
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethics approval
This study was approved by the University of Pretoria Ethics Committee (Reference no.: 599/2024). All procedures followed the ethical standards of the Helsinki Declaration of 1975, as revised in 2008.
REFERENCES
1. Oulis C, Berdousis E, Vadiakas G, Goumenos G. Garre's osteomyelitis of an unusual origin in a 8-year-old child. A case report. Int J Paediatr Dent. 2000;10(3):240-4. [ Links ]
2. Kim H, Kwon J, Kim HJ, Oh S, Kim DS, Jang JH. Garre's osteomyelitis of the mandible managed by nonsurgical re-endodontic treatment. Restor Dent Endod. 2024;49(2):1-7. [ Links ]
3. Tong ACK, Ng IOL, Yeung KMA. Osteomyelitis with proliferative periostitis: an unusual case. Oral Surgery, Oral Med Oral Pathol Oral Radiol Endod. 2006;102(5):14-9. [ Links ]
4. Fukuda M, Inoue K, Sakashita H. Periostitis Ossificans Arising in the Mandibular Bone of a Young Patient: Report of an Unusual Case and Review of the Literature. J Oral Maxillofac Surg [Internet]. 2017;75(9):1834.e1-1834.e8. Available from: http://dx.doi.org/10.1016/j.joms.2017.04.015 [ Links ]
5. Georgaki M, Delli K, Paschalidi P, Gkizani S, Tsiklakis K, Nikitakis NG. Chronic Osteomyelitis with Proliferative Periostitis of the Mandible in a Child: Report of a Case Managed by Immunosuppressive Treatment. Pediatr Infect Dis J. 2022;41(1):E10-5. [ Links ]
 Correspondence:
Correspondence:
Name: Zarah Yakoob
Contact details: zarah.yakoob@up.ac.za
Authors contribution:
Zarah Yakoob Primary author - 100%

{kind=link}