










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
versão On-line ISSN 2078-676Xversão impressa ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.40 no.1 Pretoria Mar. 2024
https://doi.org/10.7196/SAJCC.2024.v40i1.1396
RESEARCH
Nutrition support practices in the intensive care unit of a tertiary hospital in Ghana
E K AnkuI; L O SamadII; G AkafityIII; S A AmooIV; L T HillV
IMPH, RD; Department of Dietherapy and Nutrition, Cape Coast Teaching Hospital, Cape Coast, Ghana
IIMB ChB, DA WACS, MGCS; Department of Anaesthesia and Critical Care, Cape Coast Teaching Hospital, Cape Coast, Ghana
IIIBSc; Department of Research, Monitoring and Evaluation, Cape Coast Teaching Hospital, Cape Coast, Ghana
IVMN, RN; Department of Anaesthesia and Critical Care, Cape Coast Teaching Hospital, Cape Coast, Ghana
VPhD, RD (SA); Critical Point Critical Care Nutrition Consultancy, Cape Town, South Africa
ABSTRACT
BACKGROUND. Nutrition support is recognised as an important therapy for attenuating the catabolic effects of critical illnesses, including malnutrition prevention. However, variations in nutrition support practices make it difficult to achieve optimal outcomes in the intensive care unit (ICU).
OBJECTIVES. To explore current nutrition support practices among healthcare professionals (doctors and nurses) in the ICU of a tertiary hospital in Ghana.
METHODS. Via a cross-sectional survey, the nutrition support practices and self-reported skills of 30 ICU healthcare professionals (23 nurses and 7 doctors) providing nutrition support were explored. Results are presented as themes with frequencies and proportions. Categorical data were analysed using Fisher's exact test. Statistical significance was set at p<0.05.
RESULTS. Most of the respondents were young and had limited ICU experience. Almost half of the respondents were unaware of or were not familiar with the content of an in-house feeding protocol for both enteral nutrition (EN) and parenteral nutrition support, despite a majority reporting the feeding protocol as the main source of nutrition support information. There was a general lack of standardisation of execution of most nutrition support practices, especially with the pattern of EN delivery, usual method of optimising EN, and gastric residual volume threshold used to guide practice. Most respondents self-reported being average/satisfactory in the management of nutrition support.
CONCLUSION. The study revealed that healthcare professionals in our ICU had varying nutrition support practices and competencies. There is a need for standardised and practical feeding protocols in accessible formats, ongoing education, and training in nutrition support to improve nutrition support practices and competencies of healthcare professionals providing nutrition support in the ICU setting.
Keywords: Nutrition support practices, ICU nutrition, nutrition protocols, enteral nutrition, parenteral nutrition.
Nutrition support has been recognised as an important therapy for attenuating the catabolic effects of critical illness.[1,2] This is because medical nutrition therapy aims to avoid malnutrition in well-nourished patients and prevent further deterioration in malnourished or high-risk individuals.[3] Studies have revealed that attenuation of the catabolic effects of critical illness is associated with improved outcomes in the intensive care unit (ICU).[4,5] Despite the benefits of medical nutrition therapy in the ICU, optimal nutrition approaches remain a challenge.[1,3,6]
One of the challenges in achieving optimal nutrition support is variations in actual clinical nutrition practices[4,5,7] delivered to ICU patients. Implementation and adherence to nutrition support practice guidelines may not be as easy as it seems[5] and nutrition support is often overlooked in critical cases.[8] Some of the factors contributing to the reduced implementation of nutrition support guidelines include a high workload, resistance to change, lack of awareness, lack of knowledge, lack of critical care experience, complex patient conditions, inadequate resources, obstructive administrative processes, lack of evidence, or outdated guidelines.[8,9]
Observational studies across various ICUs have shown wide variations in nutrition support practices.[10] A Ghanaian hospital survey revealed that enteral and parenteral nutrition support decisions were guided by clinical judgment and professional experience,[11] implying that a greater proportion of nutrition support decisions were not based on evidence. This finding suggests that there is a gap in the implementation of nutrition support guidelines. In addition, a substantial proportion of healthcare professionals in Ghana do not have the comprehensive skills or competence to provide nutrition support.[11] To the best of our knowledge, the cited study by Abban[11] is the first to report findings on nutrition support practices in Ghanaian hospitals. However, these findings are not specific to ICU settings, therefore reducing their ability to address issues specific to ICU nutritional care.
The present study aimed to explore current nutrition support practices among healthcare professionals in the ICU of a tertiary hospital in Ghana, as well as to evaluate whether protocols currently in place are clinically applicable or useful. In addition, this study aimed to provide baseline data to guide protocol development, policies, and quality improvement initiatives in a Ghanaian hospital setting.
Methods
Study design
The present study was a cross-sectional survey of healthcare professionals in the ICU of a tertiary hospital in Ghana. A survey questionnaire with closed-end responses was used to explore the nutrition support practices, as well as self-reported skills and competence of healthcare professionals providing nutrition support to ICU patients.
Study site
This single-centre study was conducted in the ICU of a tertiary hospital in Ghana. The ICU is a 4-bed level 1 unit ICU. It caters for both paediatric and adult patients. The staffing capacity of the ICU included 42 nurses (4 critical care nurses and 38 general nurses), 7 doctors, a dietitian to cover the ICU, and a pharmacist. The ICU was monitored by an anaesthesiologist. Nurses in the ICU work rotationally in three 8-hour shifts with 5 nursing staff and 3 doctors per shift.
Study population
The study was conducted among full-time healthcare professionals. Student nurses, house officers, nurses on internships, and healthcare professionals who were part of the anaesthesia and critical care department of the hospital but did not work in the ICU, were not asked to participate in the survey.
Sampling technique
The total enumeration sampling technique was used in this study. The expected sample size was 48. The survey was distributed over a 1-month period via internal, departmental channels and via social media platforms of various professional designations in the ICU, as well as a general ICU social media platform. Reminders were provided weekly after the initial survey distribution.
Data collection
The Hill Questionnaire[5] was adapted and modified for this study. Hill's study evaluated nutrition support practices with sub-themes on nutrition screening and assessment, nutrition decision-making, enteral nutrition delivery, administration and monitoring; parenteral nutrition delivery, administration and monitoring; and the types of nutrition products used. Hill[5] asked questions regarding perceptions and self-reporting of nutrition support skills.
The questionnaire was modified with guidance from the written nutrition protocol in our ICU and discussions with study investigators. The questionnaire was piloted among four key healthcare professionals in the ICU. The results of this pilot survey were included in the main survey; however, the survey distribution and data collection processes were streamlined following the pilot phase.
Data handling and analysis
Survey responses were anonymously submitted to protect the identities of the participants. Data were collected via a protected link and exported as a spreadsheet. Data were imported and cleaned using various tidyverse[12]packages, and analysed using R version 4.2.1. The results of this study are organised into subthemes with frequencies and proportions. Categorical data were analysed using Fisher's exact test. Statistical significance was set at p<0.05.
Ethical considerations
The study was approved by the Ethical Committee of the Cape Coast Teaching Hospital in Ghana (ref. no. CCTHERC/EC/2022/102). The responses were anonymous, and the analysis was performed at the group level. Invited healthcare professionals were informed of their right to not participate in the study without any consequences.
ICU nutrition protocol
The ICU at the tertiary hospital has a written protocol in the form of a manual, written as a guideline for the management of critically ill patients. Healthcare professionals working in the ICU are expected to be aware of the availability of such protocols and to comply with their use. The ICU nutrition protocol covers aspects of nutrition screening and assessment, fluid determination, nutrition requirements determination, enteral and parenteral nutrition, and gastric residual volume for monitoring of feeding tolerance, and is fundamentally based on clinical practice guidelines published by international professional societies.[13,14] The protocol makes recommendations regarding these elements of nutrition support without specifying or prescribing the techniques or methods to be used.
There are no formal training requirements for ICU healthcare professionals regarding the ICU protocols, so it was unclear to what extent the protocol was implemented, or the uniformity of nutrition support practices among various ICU staff in our facility before this survey. The protocol was last updated prior to the publication of newer clinical practice guidelines, and it was put together by a group of staff with ICU insight, mainly anaesthetists and nurses. Part of the rationale for the survey was to evaluate adherence to the protocol and identify any inconsistencies to inform a pending substantial overhaul of the ICU nutrition protocol and highlight any training needs that might be identified in supporting quality nutrition practices in our ICU.
Results
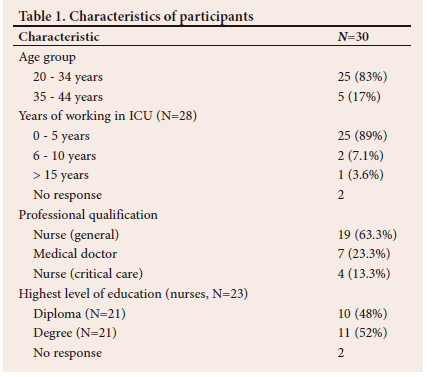
Thirty responses were received, representing 63% of the expected sample size. Most healthcare professionals were aged between 20 and 34 years (85%), and the majority had worked in the ICU for 0 - 5 years. In terms of professional qualifications, most respondents were general nurses (63%), followed by medical doctors (23%) and critical care nurses (13%). Among the nurses, 48% had a diploma as their highest level of education, while 52% had a degree (Table 1).
Nutrition screening, assessment and nutrition support decision-making
Most respondents reported that this task was routine in the ICU and mostly performed by dietitians (Fig. 1A). However, there was variation in the reported methods used to achieve this task, with 30% of respondents being uncertain of the method used (Fig. 2).
Most respondents (52%) reported the availability of a written protocol for both enteral and parenteral nutrition; 11% reported a protocol for enteral nutrition only, and 7.4% reported parenteral nutrition only. Thirty percent of respondents did not report the availability of a written protocol (Table 2). General doctors (47%) were mainly reported as the decider on the route of nutrition support, followed by dietitians (33%), and anaesthesiologists (20%), while fluid allocations were reported as a multi-disciplinary decision. Most respondents (83%) reported having a formal nutrition support team. There were no significant differences in any of these findings between doctors and nurses.
Most respondents reported not knowing how to estimate the nutritional requirements of ICU patients, indicating that clinical judgment and body weight methods were the common approaches (Fig. 3).
Enteral nutrition support practices
Enteral nutrition (EN) was mainly initiated when reasonable gastrointestinal tract (GIT) function was present (the subjective view according to clinical judgment that adequate motility, digestion and other gut functions would support tolerance of enteral feeding) or when bowel sounds were present (Fig. 4A). There was general agreement on the widespread use of nasogastric enteral delivery as well as practices around placement and replacement of enteral feeding tubes. By report, there was no uniform method used to optimise EN although gastric acid suppression was commonly reported to be employed (Table 3). The results showed a lack of standardisation in the use of gastric residual volume (GRV) thresholds to guide practice, the timing for the initiation of EN, and the frequency of assessing EN tolerance. Most respondents indicated that EN was monitored in compliance with EN protocol (Fig. 5A).
Aspects of the daily routines of EN delivery were not uniformly reported. While there was general agreement that EN was started within 24 hours of ICU admission, or when pre-determined GRV thresholds had been met, there were discrepant reports of the role and importance of GRVs in guiding practice. Nurses mainly reported that there was no GRV standard volume to guide practice, while most doctors indicated the threshold was <250 mL. The reported pattern of EN delivery varied widely, with 39% of respondents reporting intermittent boluses, 18% reporting continuous infusions during the day and stopped during the night for several hours, and 21% reporting continuous infusions but with short holds for tolerance testing and gastric aspirations. Intermittent bolus delivery was found to be a common practice in our ICU, as reported by most respondents.
Practices around assessment of enteral feed tolerance were also not well aligned. The GRV as a guide for enteral feeding was not standardised in our ICU setting, and neither was the timing for the initiation of EN, with different doctors and nurses reportedly using different criteria. According to the survey results, the use of post-pyloric enteral feed delivery was not routine in the ICU (48%) and, when reported, it was most commonly due to unsuccessful gastric deliveries (20%). Nevertheless, 24% of respondents overall reported post-pyloric feeding to be routine in the ICU. There were no statistically significant differences in reports from different healthcare professional groups.
Parenteral nutrition support practices
Criteria to commence parenteral nutrition (PN) and timing of PN commencement is shown in Figs 4B and 6, respectively. PN was commenced mainly in GIT failure or inaccessibility, while the timing of PN initiation was reported by most respondents as immediate once the clinical indication emerged.
Overall, the results indicate that respondents use clinical judgment as the primary basis for PN decision-making (59%), commonly use central venous catheters (CVCs) for PN delivery, while 21% were uncertain about the basis for PN use. Use of clinical guidelines to inform PN decisions was very low (3.4%) (Table 4). Most respondents reported using PN to provide requirements only when EN was not possible, followed by PN supplementation in all patients who did not meet their requirements with EN (28%), and not being sure (6.9%). Clinical signs/ symptoms of intolerance were reported as the main method used to monitor PN (Fig. 5B). There were no significant differences between responses from nurses and those from doctors.
However, doctors and nurses differed in their frequency of biochemical monitoring of PN safety and tolerance. ICU healthcare professionals reported their frequency of biochemical monitoring of PN safety and tolerance, with 23% reporting 1 - 3 times weekly, 19% reporting daily, 27% reporting no standard, and 31% reporting randomly, as clinically indicated. Doctors were more likely to report monitoring PN safety and tolerance 1 - 3 times weekly (86%) than nurses were (0%) (p<0.001). Instead, the response to this question from nurses showed that nurses did not perceive biochemical monitoring in any standardised pattern for patients on PN, with 31% reporting 'randomly' and a further 27% reporting 'no standard'.
Skills and competence
The results (Table 5) showed that most respondents self-reported as average/satisfactory in their competence in nutrition support (45%) and 38% considered themselves above average. In terms of formal (meaning structured or accredited) nutrition education or training, 55% of respondents have reportedly received such education or training. No statistically significant differences were found between nurses and doctors regarding competence in nutrition support, formal nutrition education, or training. Regarding the main source of information for nutrition support, the most reported source was the feeding protocol (34%), followed by in-service training (21%), and colleagues (17%). A small proportion of healthcare professionals reported journal articles and workshops/conferences. No statistically significant difference was found between nurses and doctors in terms of the main source of nutrition support information.
Discussion
The results of this survey showed discrepant nutrition support practices in the ICU, with a high degree of uncertainty over multiple aspects of nutrition support in the ICU. This is probably related to the finding that 30% of ICU staff were unaware of the existence of the ICU Nutrition Protocol or were unfamiliar with the protocol content. Survey responses were similar between nurses and doctors, with the main thematic responses being nutrition support decision-making, EN support practices, PN support practices, and self-reported skills and competence. There was a sense that nutrition support was a team approach, with the decisions around fluid allocations to nutrition and route of nutrition support generally being made jointly. Clinically important aspects of nutrition support that showed overall agreement among respondents were the commonly used route of EN delivery, vascular access for PN delivery, and method for checking the position of EN tubes, while there was more disparity in the pattern of EN delivery, frequency of EN monitoring, usual method of optimising EN, usual frequency of assessing EN, GRV threshold used to guide practice, and frequency of biochemical monitoring of PN safety and tolerance.
It was noted that most ICU healthcare professionals did not know how to estimate the nutritional requirements of patients. The hospital's ICU protocol recommends using indirect calorimetry (IC), weight-based equations, and predictive equations to estimate the energy requirements of patients, consistent with international guidelines.[13,14] However, IC is not available, which hampers the ability to personalise the needs of patients in the ICU. The usual methods for estimating energy needs are weight-based equations which also present unique challenges owing to the unavailability of weight measurements. Continuous weight monitoring is challenging. As such, energy and nutrient requirements are largely based on clinical judgment or ideal body weight estimates, as indicated by some respondents. This observation was made in other Ghanaian hospitals,[11] indicating that this practice may be the general approach to nutrition care for critically ill patients in this country. In South African ICUs, a combination of methods such as body weight-based methods combined with guidelines was shown to be used.[5] The inability to appropriately estimate the nutritional requirements of ICU patients may lead to underfeeding and overfeeding which can result in poor outcomes in critically ill patients.[15] Alternative predictive equations have also been shown to be less accurate in estimating energy requirements,[15] and their potential use in our setting is hampered by the aforementioned challenges owing to the difficulty in obtaining accurate weight measurements. Strategies are needed to improve the estimation of the nutrient needs of critically ill patients in our setting, as it is the starting point for all nutrition support practices that follow.
Besides the need to inform nutrition prescribing more accurately, optimisation of EN delivery is key to feeding success. In this survey, most respondents reported no routine method for optimising EN. The hospital's ICU protocol recommends reduced volume of feed, post-pyloric feeding, and use of prokinetics; however, these methods do not include practical recommendations or algorithmic approaches to guide nursing staff in their decision-making or implementation. Various nutrition guidelines recommend[1314,16] feeding into the small bowel in cases where patients are at high risk of aspiration. However, post-pyloric feeding is not routinely practiced in our ICU. Surprisingly, some respondents mentioned that post-pyloric feeding is a routine practice in our ICU. The unavailability of the post-pyloric technique in our setting means that certain patients who may have indications, such as gastroparesis, acute pancreatitis, gastric outlet stenosis, hyperemesis, severe aspiration, tracheoesophageal fistula, or stenosis in gastroenterostomy,[16] may not have access to optimal nutrition support. Post-pyloric feeding is also generally administered via the continuous infusion route[16] which is not a routine pattern of EN delivery in our ICU. Surprisingly, some respondents reported continuous infusion as a pattern of EN delivery in our ICU. This may be due to a technical misunderstanding of the meaning of continuous infusion. Post-pyloric feeding is a challenge because enteral formulas and continuous infusion bags are not readily available in our setting. Elemental and semi-elemental formulas are also not available to support the feasibility of post-pyloric feeding in our setting, although polymeric feeds are used in some cases.[16] Post-pyloric feeding has also been demonstrated as an alternative to PN in some instances.[16] However, both approaches to providing nutrition are not routine in our setting. The cost and unavailability of parenteral products make it difficult to recommend PN to patients who present with contraindications for EN. In such situations, ICU healthcare professionals tend to resort to waiting for an appropriate time to commence EN, when the patient would have deteriorated in relation to their nutritional status.
Aspirating EN every 4 hours is standard practice in our ICU, with a GRV of 250 mL used as a threshold for feeding intolerance. The reports from the survey were consistent with this daily nursing practice. This frequency of assessing tolerance is a common practice in other Ghanaian hospitals[11] and is similar in South African ICUs.[5] Most respondents were unaware of this recommendation, despite it being part of daily practice. A possible explanation is that when issues arise with EN, doctors may provide different recommendations which reflect the fact that 35% of respondents report different standards used. In South African ICUs, different volumes were used as a threshold.[5] Tolerance in European ICUs is assessed every 24 hours, reflecting the dominant pattern of feeding EN in their setting being continuous[4] rather than intermittent bolus. Some international guidelines[13,16,18] recommend using GRV to assess feed tolerance whereas others do not.[14] This apparent variability tends to confuse healthcare staff and affects the implementation of GRV recommendations[10] and decision making in the ICU.
Staff uncertainty around expected nutrition delivery practices in a single ICU unit may be a more important determinant of medical nutrition therapy success than the validity of any particular practice itself. It was observed on more than one point/survey question that staff indicated answers not applicable to the ICU setting in which they work; for example, the selection of IC as a method for estimating nutritional requirement and the use of nutrition screening tools. This is clearly a problematic finding and may suggest that insight into nutrition support, or comprehension of the protocol, is in fact weaker than initially apparent. Either way, this type of finding reveals a deficiency in the training of ICU staff on nutrition support options available to them, or the need to improve awareness of such tools. The purpose of protocolised operations in clinical practice is to achieve standardisation to drive quality of care.[10,19] It has been shown numerous times, as published by Heyland's group,[19,20] that EN success in particular is enhanced by lower variation in the implementation equipment such as IC automatically translate into improved quality of care. Rather, a dedicated focus on consistent quality nutrition support practices by a multidisciplinary team lead to better nutrient delivery.[20,21] For our small unit, the current survey is the first audit step in driving improved quality of nutritional care, because it has of nutrition guidelines according to individual staff perceptions. The adherence to nutrition guidelines can be complex,[19] as it involves multiple enabling factors, but it is achievable.[21] Despite resource limitations being identified as a hindrance to following guidelines,[19] neither the sophistication of a clinical setting nor the availability of enabled the identification of points of misunderstanding and divergent practice, and identification of key training areas. This is particularly relevant considering the unique staff demographics (young and less experienced) in our facility and the lack of self-reported expertise and confidence in nutrition support.
Considering the importance of nutrition for optimal outcomes in critically ill patients, there is a need for nutrition professionals to be better integrated into the care of critically ill patients. The role of dietitians in our ICU was recognised in this survey, particularly regarding nutrition assessment and as part of multidisciplinary team decision-making for nutrition support. This is consistent with the findings from other settings.[7] A recent survey among nutrition professionals in Ghana showed that dietitians were less involved in nutrition support decisions in hospitals.[22] This is because the primary training of dietitians in Ghana is not focused on advanced practice areas such as nutrition support in the ICU setting, and few dietitians work in this discipline. There is work to be done in developing cross-professional insight about the value of clinical nutrition. Because critical care as a specialty in Ghana is new, upskilling professional capacity, and building medical nutrition therapy competence and capacity, will be helpful in optimising care for critically ill patients in the country.[22]
The presence and formalisation of a nutrition support team may be essential to improve decision-making in relation to nutrition support. Most respondents reported the presence of a formal nutrition support team, although this was not the case in practice. This report may be due to the perceptions of respondents about what a team is. Working with the same people on a daily basis around all aspects of patient care, including nutrition, may lead an individual to perceive that a nutrition team is present. This observation was also made in South African ICUs.[5] Nutrition support teams is not a major feature of ICUs across the world.[4,5,7,23,24] Two possible reasons include a lack of interest from healthcare professionals and a lack of clinical leadership.[25] Nutrition support teams, together with a comprehensive feeding protocol, are tools for improving nutrition support practices in our setting.
Although most respondents (34%) reported the in-house protocol as the major source of nutrition support information (Table 5), which was not surprising, close to half of the respondents did not know of the availability of a nutrition protocol. This may be because the ICU nutrition protocol is not accessible to most healthcare professionals in its current format. Evidence suggest that text-based resources are less often used[10] when decisions need to be made, especially at the bedside. Also, nurses do not frequently consult feeding protocols even if they are readily available.[26] In addition, there are no formal requirements for knowledge with respect to nutrition support, and ICU healthcare staff may assume that they know about nutrition support from daily practice. This was evidenced by the fact that some respondents reported colleagues as being the main source of nutrition support information. It is not particularly concerning, especially if ICU healthcare professionals have expertise in nutrition, and information from colleagues has been shown as a preferred method of obtaining information by some healthcare professionals.[10] It should be noted that most respondents self-reported their competence as average, implying that they were not particularly confident about approaching nutrition support in the ICU. Even among nutrition professionals in Ghana, perceived confidence in providing EN and PN is low.[22] This finding supports the need for additional post-qualification training[26] to improve the competence of healthcare professionals to provide nutrition support. The in-house feeding protocol, reported as a major source of nutrition support information, suggests the importance of feeding protocols for nutrition support practices.[19] However, accessibility and implementation steps seemed to have failed. Therefore, developing a practical feeding protocol in accessible formats such as infographics, help guides and frequently asked questions (FAQs) may help disseminate timely and appropriate nutrition support information for healthcare professionals in our setting. Feeding protocols have been shown to empower nurses[14] who may not be involved in nutrition support decision-making,[5] despite nurses being at the forefront of implementing nutrition support decisions.[10,26] Additionally, identifying local barriers and enablers to feeding may be necessary to enhance the implementation of recommended nutrition support guidelines.[19]
Study limitations
The present study pertained to a single ICU in a tertiary hospital; as such, results may not reflect nutrition support practices across ICUs in Ghana. Variations reported among clinicians may have been non-significant only because of the small sample size. Future studies can explore the nutrition support practices of key informants in the ICU using a qualitative approach[9] to identify barriers and enablers of nutrition support practices. Regular audits of nutrition support practices in ICU may also be useful'19,271 to evaluate the impact of training to minimise variations in nutrition support practices. The current study did not focus on calorie or protein delivery from EN or PN. This can be the focus of future studies to ascertain the nutrient provision in the ICU setting in Ghana.
Conclusion
Nurses and doctors did not differ significantly with respect to nutrition assessment, nutrition support decision-making, enteral and parenteral nutrition support practices, and competence in the management of nutrition support in our ICU. Various disparities in reported nutrition support practices were shown in the results of the study among respondents in the ICU. This suggests an overall lack of awareness and inconsistent application of nutrition support protocols in the ICU. There is a need for standardised and practical feeding protocols in accessible formats for clinicians, ongoing education, and training in nutrition support to improve nutrition support practices and competencies of respondents providing nutrition support in the ICU setting. Further studies are required to assess the impact of these interventions on nutrition support practices among ICU healthcare professionals in our setting.
Declaration. We declare that this article is our original work and we take full responsibility for its content and authenticity.
Acknowledgements. We acknowledge the respondents of this study for their participation. EKA thanks Prince Kweku Yalley Abban for his suggestions during the development stage of the study. GA received mentorship from the European Society of Clinical Microbiology and Infectious Diseases via Prof. Dr Jordi Rello.
Author contributions. All authors contributed to the conceptualisation and design of the study. EKA contributed to the primary draft of the manuscript and data analysis. All authors contributed to revisions and the final draft for publication. All authors read and approved the final article.
Funding. The authors received no specific funding for this study.
Conflicts of interest. The authors have no conflicts to disclose with regard to this study. However, LTH has formerly and currently consults professionally to various companies involved in the manufacture and marketing of medical nutrition therapy products.
Data availability statement. Datasets and code used for analysis of this study are available at: https://github.com/KomlaRD/nutrition_support_practices
References
1. Chowdhury R, Lobaz S. Nutrition in critical care. BJA Educ 2019;19(3):90-95. https://doi.org/10.1016/j.bjae.2018.11.007 [ Links ]
2. Ferrie S, McWilliam D. Failure of a quality improvement process to increase nutrition delivery to intensive care patients. Anaesth Intensive Care 2006;34(2):191-196. https://doi.org/10.1177/0310057x0603400211 [ Links ]
3. Hill A, Elke G. Nutrition in the intensive care unit - a narrative review. Nutrients. 2021;13(2851):1-26. https://doi.org/10.1186/cc360 [ Links ]
4. Roynette CE, Bongers A, Fulbrook P, Albarran JW, Hofman Z. Enteral feeding practices in European ICUs: A survey from the European federation of critical care nursing associations (EfCCNa). e-SPEN 2008;3(2). https://doi.org/10.1016/j.eclnm.2007.10.004 [ Links ]
5. Hill LT. Nutrition support practices in South African ICUs: Results from a nationwide pilot survey. South Afr J Crit Care 2015;31(2):42-50. https://doi.org/10.7196/SAJCC.2015.v31i2.252 [ Links ]
6. Gentles E, Mara J, Diamantidi K, et al. Delivery of enteral nutrition after the introduction of practice guidelines and participation of dietitians in pediatric critical care clinical teams. J Acad Nutr Diet 2014;114(12):1974-1980.e3. https://doi.org/10.1016/jjand.2014.04.027 [ Links ]
7. Heyland DK, Schroter-Noppe D, Drover JW, et al. Nutrition support in the critical care setting: current practice in Canadian ICUs--opportunities for improvement? J Parenter Enter Nutr 2003 1;27(1):74-83. https://doi.org/10.1177/014860710302700174 [ Links ]
8. Yang L, Dong Z. Adherence to guidelines on nutritional support by medical residents in an intensive care unit in China: A prospective observational study. Med Sci Monit 2019;25:8645-8650. https://doi.org/10.12659/MSM.917684 [ Links ]
9. Jones NE, Suurdt J, Ouelette-Kuntz H, Heyland DK. Implementation of the Canadian Clinical Practice Guidelines for Nutrition Support: A multiple case study of barriers and enablers. Nutr Clin Pract 1;22(4):449-457. https://doi.org/10.1177/0115426507022004449 [ Links ]
10. Marshall BAP, Cahill NE, Gramlich L, Macdonald G, Alberda C, Heyland DK. Optimizing nutrition in intensive care units: Empowering critical care nurses to be effective agents of change. Am J Crit Care 2012;21(3):186-194. https://doi.org/10.4037/ajcc2012697 [ Links ]
11. Abban PKY. Nutrition support practices in Ghanaian hospitals. University of Ghana; 2020. https://ugspace.ug.edu.gh/handle/123456789/35926 [ Links ]
12. Wickham H, Averick M, Bryan J, et al. Welcome to the Tidyverse. J Open Source Softw 2019;4(43):1686. https://doi.org/10.21105/joss.01686 [ Links ]
13. Critical Care Nutrition. 2015 Canadian Clinical Practice Guidelines. https://www.criticalcarenutrition.com/resources/cpgs/past-guidelines/2015. (accessed 31 January 2020). [ Links ]
14. McClave SA, Taylor BE, Martindale RG, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). J Parenter Enter Nutr 2016;40(2):159-211. https://doi.org/10.1177/0148607115621863 [ Links ]
15. Zusman O, Theilla M, Cohen J, Kagan I, Bendavid I, Singer P. Resting energy expenditure, calorie and protein consumption in critically ill patients: A retrospective cohort study. Crit Care 2016;20(1):1-8. https://doi.org/10.1186/s13054-016-1538-4 [ Links ]
16. Singer P, Blaser AR, Berger MM, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr 2019;38(1):48-79. https://doi.org/10.1016/jxlnu.2018.08.037 [ Links ]
17. Niv E, Fireman Z, Vaisman N. Post-pyloric feeding. World J Gastroenterol 2009;15(11):1281-1288. https://doi.org/10.3748/wjg.15.1281 [ Links ]
18. Blaser AR, Starkopf J, Alhazzani W, et al. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intensive Care Med 2017;43(3):380-398. https://doi.org/10.1007/s00134-016-4665-0 [ Links ]
19. Cahill NE, Suurdt J, Ouellette-Kuntz H, Heyland DK. Understanding adherence to guidelines in the intensive care unit: Development of a comprehensive framework. J Parenter Enter Nutr 2010;34(6):616-624. https://doi.org/10.1177/0148607110361904 [ Links ]
20. Dodek P, Cahill NE, Heyland DK. The relationship between organisational culture and implementation of clinical practice guidelines: A narrative review. Knowl Transl 2018;34(6):6669-6674. https://doi.org/10.2307/j.ctv5vdf1q [ Links ]
21. Cahill NE, Dhaliwal R, Day AG, Jiang X, Heyland DK. Nutrition therapy in the critical care setting: What is "best achievable" practice? An international multicenter observational study. Crit Care Med 2010;38(2):395-401. https://doi.org/10.1097/CCM.0b013e3181c0263d [ Links ]
22. Ayande REA, Agordoh PD, Salino VJ, et al. Knowledge, attitudes, and practices of registered dietitians and nutritionists regarding enteral and parenteral nutrition support in Ghana: A needs assessment study. Front Nutr 2023;10(June):1-10. https://doi.org/10.3389/fnut.2023.1197610 [ Links ]
23. Sharifi MN, Walton A, Chakrabarty G, Rahman T, Neild P, Poullis A. Nutrition support in intensive care units in England: A snapshot of present practice. Br J Nutr 2011;106(8):1240-1244. https://doi.org/10.1017/S0007114511001619 [ Links ]
24. Fulbrook P, Bongers A, Albarran JW. A European survey of enteral nutrition practices and procedures in adult intensive care units. J Clin Nurs 2007 1;16(11):2132-2141. https://doi.org/10.1111/j.1365-2702.2006.01841.x [ Links ]
25. Guenter P, Blackmer A, Malone A, Phillips W, Mogensen KM, Becker P. Current nutrition assessment practice: A 2022 survey. Nutr Clin Pract 2023;1-11. https://doi.org/10.1002/ncp.10998 [ Links ]
26. Ramuada L, Veldsman L, Livhuwani N, Blaauw R. Assessment of knowledge, attitude and practice of nurses regarding enteral nutrition at a military hospital. South Afr J Clin Nutr 2023;36(2):63-69. https://doi.org/10.1080/16070658.2022.2076970 [ Links ]
27. Sinuff T, Cahill NE, Dhaliwal R, Miao Wang, Day AG, Heyland DK. The value of audit and feedback reports in improving nutrition therapy in the intensive care unit: A multicenter observational study. J Parenter Enter Nutr 2010;34(6):660-668. https://doi.org/10.1177/0148607110373484 [ Links ]
 Correspondence:
Correspondence:
E K Anku
ankueric1@gmail.com
Accepted 8 January 2024
Contribution of the study
This study is the first to describe challenges of nutrition support practices in an intensive care unit (ICU) in Ghana and is among limited data on this topic from African countries. This study has provided important insights into both the needs and opportunities for enhancing clinical nutrition skills and knowledge, and the practical application of such improved knowledge. As such, these data are important for local quality improvement for both clinical care of ICU patients and for professional development of healthcare personnel in resource-constrained hospital settings.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}